

Subscribe to RSS
DOI: 10.1055/s-0045-1814744
Postnatal Outcome of Prenatally Diagnosed Intra-Abdominal Cysts
Authors

Abstract
Aim
This article compares the antenatal diagnosis of fetal intra-abdominal cysts with postnatal diagnosis and determines the diagnostic accuracy of ultrasound in correctly diagnosing the origin of prenatal abdominal cysts.
Methods
A prospective study of antenatally diagnosed fetal intra-abdominal cysts was conducted from January 2022 to December 2023. Cases of fetal intra-abdominal cysts that fulfilled the criteria were included in the study. The imaging characteristics of various types of cysts were summarized and compared with postnatal follow-up results.
Result
In our study, the fetal intra-abdominal cysts were prenatally diagnosed in 24 cases. Of 24 cases, postnatal follow-up was available for 19 (79.16%) cases. The antenatal diagnosis was confirmed postnatally in 18 cases (94.73%). Five cases could not be examined postnatally, as in two cases pregnancy was terminated, two babies died after birth before investigations, and one case was lost to follow-up.
Conclusion
An appropriate ultrasound examination, combined with comprehensive analysis and careful judgment, leads to an accurate diagnosis and proper postnatal management.
Introduction
Fetal abdominal cysts are rare. With recent advances in ultrasound (US) techniques and increasing clinical experience, routine US screening has facilitated the early detection of fetal structural abnormalities.[1] [2] [3] [4] The abnormal cystic structure mainly originates from either the gastrointestinal (GI) tract or the genitourinary tract.[5] [6] [7] [8] [9] However, since abdominal cysts may originate from different reproductive, urinary, and digestive systems,[6] [7] [8] [9] it is challenging to accurately determine the origin of cysts antenatally via US and predict postnatal outcome. Most of the GI tract is located in the abdominal cavity, which contains other structures such as the liver, choledochal system, pancreas, mesentery, and omentum.
Genitourinary tract related organs are the kidneys, adrenals, and ovaries in females. One of the main difficulties in the sonographic examination of the fetal abdomen is establishing the origin of an intra-abdominal cyst during examination, which could be from any of the structures mentioned here or from abnormal development of early embryonic structures and embryonic abdominal totipotential cells, such as teratomas. Location, sonographic appearance, associated anomalies, gestational age at diagnosis, and fetal sex provide important information directing toward a possible diagnosis. In many cases, it remains difficult to be certain about the origin of the cyst until delivery. Assessment of the fetal sex is necessary when an abdominal cyst is detected, as some cysts are sex-related (ovarian cysts or hydrometrocolpos occur exclusively in females) or may present a sex predominance (choledochal cysts are more frequent in female fetuses). Finally, a cyst may be differentiated by the assessment of its sonographic appearance (shape, echogenicity, wall margins, or other specific features), and it is mandatory to carefully examine to detect other possible associated sonographic findings. The use of color Doppler allows examination of the vascular supply to the cyst, its anatomic relations with the abdominal blood vessels, and the possible diagnosis of its vascular origin. This is helpful in cases of umbilical vein varix or hepatic arteriovenous malformation.
Risk factors associated with intra-abdominal cystic lesions include:
-
Gonadal cyst: Placental human chorionic gonadotropin, fetal gonadotropins, Rh isoimmunization, and preeclampsia.
-
Adrenal cyst: Congenital adrenal hyperplasia and ambiguous genitalia.
-
Extralobar pulmonary sequestration: Idiopathic.
-
Mesenteric cyst: Small bowel lymphangioma.
-
Megacystis: Male fetus (posterior urethral valve), neurologic syndromes, genetic syndrome (MMIH-megacystis microcolon intestinal hypoperistalsis syndrome).
Aim of the Study
This article aims to compare the antenatal diagnosis of the intra-abdominal cyst with the postnatal diagnosis and to determine the diagnostic accuracy of US in correctly diagnosing the origin of prenatal abdominal cyst.
Methods
This is a prospective study of all cases of intra-abdominal cysts diagnosed in a tertiary fetal medicine center. US scanning for all cases was performed on a GE Voluson E8 or E10 machine equipped with a 2 to 9 MHz curvilinear, RAB 6 probe, and the Mindray Neuva I9 machine with SC6-1S probe. All antenatally diagnosed cases of intra-abdominal cyst from the period between January 2022 and December 2023 were monitored for their progress/resolution, any change in the appearance of the cyst, and any newly developed ultrasonography findings.
Cysts were differentiated by assessment of their sonographic features like size, shape, echogenicity, cyst wall, single cyst or multiple, vascularity, proximity to other abdominal organs, or other specific features.
In all cases where the cyst had not resolved antenatally, postnatal scans (US, computed tomography [CT] scan, or magnetic resonance imaging) were conducted. Antenatal diagnosis, postnatal diagnosis, and the ultimate outcome were recorded.
Only solitary cysts were included in the study. Cysts were divided into subgroups according to their prenatal suspected origin, like ovarian, GI, gallbladder, renal, mesenteric, and vascular.
Result and Discussion
[Table 1] shows that 144 intra-abdominal cysts were identified over a 2-year study period, with 120 cases involving multiple cysts and 24 cases involving solitary cysts. Cases with solitary cysts were included in the study.
|
Total intra-abdominal cyst |
144 |
|
Solitary cyst |
24 |
|
Multiple cyst |
120 |
[Table 2] shows that out of 24 antenatally diagnosed cases of intra-abdominal solitary cyst, 12 were gonadal cysts, 3 were choledochal cysts, 1 was an adrenal cyst, 1 was a hepatic cyst, 1 was an extralobar pulmonary sequestration, 1 was a renal cortical/mesenteric cyst, 1 was megacystis, 3 were umbilical vein varix, and 1 was an enteric duplication cyst.
[Table 3] shows that the origin of fetal intra-abdominal cysts was prenatally diagnosed in 24 cases.
Abbreviation: US, ultrasound.
Out of 24 cases, postnatal follow-up was available in 19 (79.16%) cases. The antenatal diagnosis was confirmed postnatally in 18 cases (94.73%), and in one case, the postnatal diagnosis was different. Five cases could not be examined postnatally, as in two cases pregnancy was terminated (hepatic cyst and megacystis), in two cases the baby died after birth (ovarian cyst and enteric duplication cyst), and one case was lost to follow-up (mesenteric cyst).
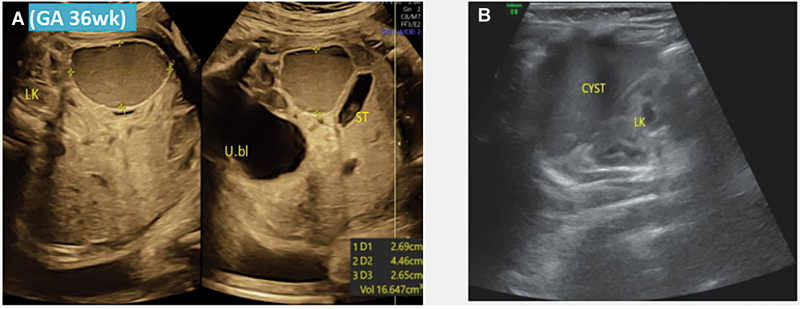
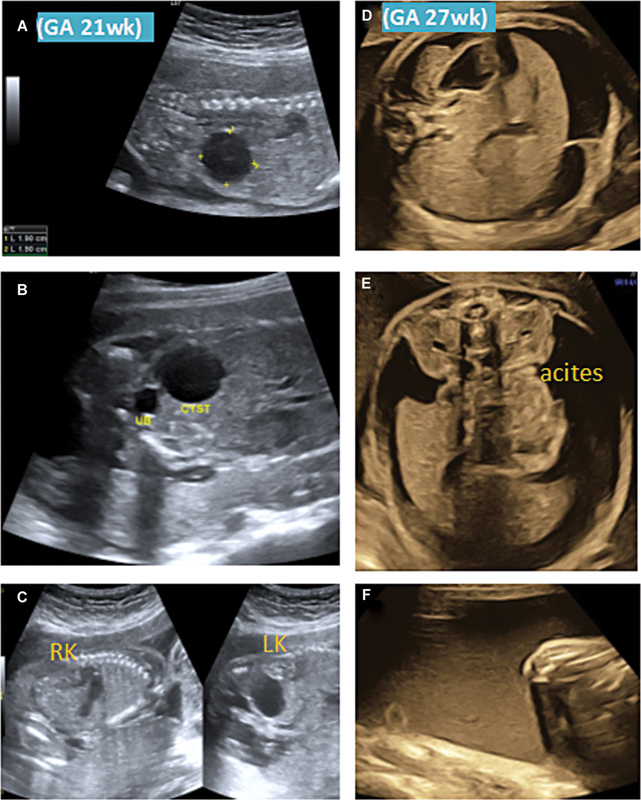
Gonadal cysts were typically seen in female fetuses only. They were all ovarian cysts. Ovarian cyst represents the response of fetal ovaries to increased maternal hormones (estrogen, human chorionic gonadotropins) and fetal gonadotropins. They are usually located in the lower abdomen close to the urinary bladder. The shape of cysts is generally regular, round/oval and cyst wall is generally thin with smooth contour. Intracapsular bleeding may occur in the cyst and hemorrhage makes the appearance of the cyst “complex” with diffuse echogenicity ([Fig. 1]). The presence of daughter cyst in ovarian cyst pathologically represents a stimulated ovarian follicle and is diagnostic of ovarian origin of the cyst[10] ([Fig. 2A]). Ascites may result from rupture of the cyst or transudation due to partial obstruction of the GI tract. Complication such as polyhydramnios develops due to impaired fetal swallowing occurring due to increased pressure on the bowel from the cyst ([Fig. 3A–F]). Majority of cases are benign. In the present study, the gonadal cyst was seen in 12 cases. All were found in female fetuses. One case was seen at 21 week, 3 cases were seen between 32 and 34 weeks, 6 cases between 35 and 37 weeks, and 2 cases between 38 and 40 weeks. Mean gestational age of presentation was 32.6 weeks. Out of 12 gonadal cysts, 3 cysts persisted even after 2 months postnatally and 1 cyst was ruptured causing ascites (follow-up scan at 27 weeks) and 8 cysts were resolved within 1 month after birth. In the present study, the accuracy of antenatal US in diagnosing gonadal cyst is 91.66%.

A choledochal cyst is also known as congenital bile duct dilatation, primary bile duct dilatation, or bile duct cystic dilatation. It is a rare condition occurring due to pancreaticobiliary maljunction that may cause pancreatic enzyme reflux into the bile ducts and result in bile duct dilatation. Choledochal cysts are found in the right upper quadrant of the abdomen near the gallbladder. They are predominantly oval in shape and have thick walls. A definitive diagnosis can be made by demonstrating the communication between the bile duct and the cyst. In the present study, three intra-abdominal cysts were diagnosed as choledochal cyst antenatally ([Figs. 4] [5] [6]). In the third case, postnatal US was suggestive of enteric duplication cyst ([Fig. 5A–C]), the patient underwent surgery for resection and anastomosis. Postoperatively, baby is alive and healthy. In the present study, accuracy of antenatal US in diagnosing choledochal cyst is 66.66%.



Fetal adrenal glands are located on the superior pole of the kidneys. The adrenal cortex is of lower echogenicity adjacent to the liver or kidney and the medulla is more echogenic than the cortex. They have a classic inverted V-shape appearance in the longitudinal section. The adrenal anomalies include cyst, hemorrhage, hypertrophy, and tumors. An adrenal cyst can be detected in the third trimester in a characteristic location, cephalad to the kidney, with an anechoic, smooth margin and a clear boundary. In the case of hemorrhage, the cyst becomes hypoechoic with an organized blood clot. In the present study, one case was diagnosed with an adrenal cyst ([Fig. 7A] and [B]). Postnatal US confirmed the diagnosis of adrenal cyst ([Fig. 7C]). In the present study, the accuracy of antenatal US in diagnosing an adrenal cyst is 100%.

The hepatic cyst usually develops due to canalicular maldevelopment. They are more commonly unilocular and are visualized on the left side. In our study, there was one case of hepatic cyst ([Fig. 8A] and [B]) with associated findings of bilateral dysplastic kidneys ([Fig. 8C] and [D]), suggestive of Meckel–Gruber syndrome, at 20 weeks of gestation. Patient terminated pregnancy.

Subdiaphragmatic extralobar pulmonary sequestration appears as a well-defined, homogenously hyperechoic lesion supplied by systemic circulation. In the present study, one case was diagnosed with extralobar intra-abdominal pulmonary sequestration (Figure ). It consisted of an island of lung parenchyma that did not communicate with the bronchial tree ([Fig. 9A–C]) and was fed by systemic circulation ([Fig. 9D]). Postnatal contrast-enhanced CT thorax confirmed the antenatal findings of intra-abdominal extra lobar pulmonary sequestration ([Fig. 9E]).

The mesenteric cyst is generally unilocular/multilocular, hypoechogenic with variable size, thin wall, and devoid of peristalsis, located anywhere in the abdominal cavity. In the present study, one case was diagnosed as a mesenteric cyst ([Fig. 10]); however, the patient was lost to follow-up.

Megacystis is defined as a longitudinal urinary bladder diameter ≥ 7 mm (in the first trimester, 11 to 13 + 6 weeks), and ≥ 30 mm in the second trimester. It may be due to an obstructive or nonobstructive cause. In the present study, megacystis was diagnosed at 13 weeks ([Fig. 11A]), with hydroureter ([Fig. 11B]), left dysplastic kidney, and right echogenic kidney ([Fig. 11C]). The bladder wall becomes thick and hyperechoic ([Fig. 11D]). The patient opted for the termination of pregnancy.

Umbilical vein varix is a focal dilatation of the intra-abdominal part of the umbilical vein. It is usually anechoic, located between the anterior abdominal wall and the lower edge of the liver, confirmed by color Doppler and pulsed Doppler examination. The measurement of the cyst should be > +2 standard deviation of the mean for gestational age. If it presents before 26 weeks, there is an increased incidence of spontaneous fetal death.[11] The present study showed three cases of umbilical vein varix at the gestational age of 37 ([Fig. 12A]), 28 ([Fig. 12B]), and 27 ([Fig. 12C] and [D]) weeks. The postnatal outcome was favorable in all three.

Enteric duplication cysts are either spherical or tubular structures with a thick wall, usually sharing a common wall with the normal GI tract. They may be anechoic or hyperechoic and with/without septations ([Table 4], and [Fig. 13A, B]). In the present study, one case with an enteric duplication cyst was diagnosed. The baby was delivered preterm 33 weeks and admitted to the neonatal critical care unit for respiratory distress. As baby was in the neonatal intensive care unit on ventilator, further investigations were not done. The baby died on day 5 after birth.

Factors associated with poor outcome:
-
Anatomical location of the cyst[12]
-
Size of the cyst > 40 mm[12]
-
Number of the cyst
-
Trimester at the time of diagnosis[12]
-
Associated abnormalities
-
Gender of fetus[13]
-
Those who require postnatal surgical treatment[13]
According to Sanna et al,[14] the most common presentation of fetal abdominal cyst is unilocular anechoic mass with no vascularity, and it is most frequently diagnosed in the third trimester, which is consistent with our findings.
Compared to Garcia-Aguilar et al,[15] in our study we have reported hepatic cyst, umbilical vein varix, and extralobar pulmonary sequestration.
Agreement between pre- and postnatal diagnosis is around 65 to 70% according to other authors,[16] which is consistent with our results.
Conclusion
In the present study, out of 24 cases, in 19 cases, postnatal follow-up was available (79.16%). The antenatal diagnosis was confirmed postnatally in 18 cases (94.73%). There are various types of fetal intra-abdominal cysts that are distinguished by their location, gestational age, sex, sonographic appearance, vascularity, and associated anomalies. Prenatal US is important to identify the cause and nature of the cyst, its progress, assessment of disease outcome, and to determine the choice of treatment. An appropriate US examination with comprehensive analysis and careful judgment therefore leads to accurate diagnosis and proper postnatal management. Advancements in imaging, that is, CT scan, significantly enhanced diagnostic accuracy, allowing better characterization and informed perinatal/postnatal management. Where most cystic lesions are benign and self-resolving, some may require postnatal surgical management and a multidisciplinary approach involving obstetricians, fetal medicine experts, neonatologists, and pediatric surgeons. Continued research and long-term follow-up are mandatory for a better understanding of the natural history of lesions and improved management protocols.
|
Cyst type |
Location |
US features |
Postnatal outcome |
|---|---|---|---|
|
Gonadal |
Lower abdomen/Pelvis of female fetus |
Late 2nd/ 3rd trimester anechoic Unilocular Thin-walled |
Most of them resolve without sequelae within 6 months |
|
Choledochal |
Right upper quadrant of liver |
Anechoic, unilocular, thick walled |
Spontaneous resolution |
|
Adrenal |
Upper pole of kidney |
Upper pole of kidney |
|
|
Hepatic |
They usually occur in the right lobe of the liver More common in females (F:M 4:1) |
Unilocular, solitary cyst |
|
|
Extralobar pulmonary sequestration |
Basal region of left hemithorax, 10% located in the upper abdomen below the diaphragm |
Hyperechoic lesion with typical feeding vessel from thoracic/ abdominal aorta |
Excellent outcome after postnatal surgical correction |
|
Mesenteric |
Intestinal |
Thick walled, heterogeneous |
Spontaneous resolution |
|
Megacystis |
Lower abdomen and pelvis, common in male fetus[17] |
Large urinary bladder > 7 mm in sagittal section with thick wall > 2 mm |
Bladder length ≥ 7 mm and 7–15 mm between 11 and 14 weeks, it is associated with chromosomal abnormalities, remaining group shows 90% spontaneous resolution, 10 % develop renal problems[18] |
|
Umbilical vein varix |
Focal dilatation between anterior abdominal wall and lower edge of liver |
Anechoic, measuring +2 SD of the mean GA, confirmed by color Doppler and pulse wave Doppler |
If diagnosed early in pregnancy, fetuses are at high risk of in utero death, UV thrombosis.[14] [19] Those diagnosed later in pregnancy careful monitoring required |
|
Enteric duplication |
40% will involve the ileum,[12] rectum, and colon |
Anechoic, thick walled, “signature gut sign” |
Postnatal surgical correction |
Abbreviations: F, female; GA, gestational age; M, male; SD, standard deviation; US, ultrasound; UV, umbilical vein.
Conflict of Interest
None declared.
-
References
- 1 Snijders RJ, Noble P, Sebire N, Souka A, Nicolaides KH. Fetal Medicine Foundation First Trimester Screening Group. UK multicentre project on assessment of risk of trisomy 21 by maternal age and fetal nuchal-translucency thickness at 10-14 weeks of gestation. Lancet 1998; 352 (9125) 343-346
- 2 Nicolaides KH. Nuchal translucency and other first-trimester sonographic markers of chromosomal abnormalities. Am J Obstet Gynecol 2004; 191 (01) 45-67
- 3 Souka AP, Pilalis A, Kavalakis Y, Kosmas Y, Antsaklis P, Antsaklis A. Assessment of fetal anatomy at the 11-14-week ultrasound examination. Ultrasound Obstet Gynecol 2004; 24 (07) 730-734
- 4 Malone FD, Canick JA, Ball RH. et al; First- and Second-Trimester Evaluation of Risk (FASTER) Research Consortium. First-trimester or second-trimester screening, or both, for Down's syndrome. N Engl J Med 2005; 353 (19) 2001-2011
- 5 Gabrielli S, Rizzo N, Reece EA. Gastrointestinal and genitourinary anomalies. In: Reece EA, Hobbins JC. eds. Clinical Obstetrics. The Fetus & Mother. 3rd ed.. Malden, MA: Blackwell Publishing; 2007: 377-400
- 6 Hyett J. Intra-abdominal masses: prenatal differential diagnosis and management. Prenat Diagn 2008; 28 (07) 645-655
- 7 McEwing R, Hayward C, Furness M. Foetal cystic abdominal masses. Australas Radiol 2003; 47 (02) 101-110
- 8 Nyberg DA, Neilson IR. Abdomen and gastrointestinal tract. In: Nyberg DA, McGahan JP, Pretorius DH, Pilu G. eds. Diagnostic Imaging of Fetal Anomalies. Philadelphia, PA: Lippincott Williams & Wilkins; 2003: 547-602
- 9 Hill LM. Ultrasound of fetal gastrointestinal tract. In: Callen PW. ed. Ultrasonography in Obstetrics and Gynecology. 4th ed.. Philadelphia, PA: W. B. Saunders; 2000: 457-487
- 10 Quarello E, Gorincour G, Merrot T, Boubli L, D'Ercole C. The ‘daughter cyst sign’: a sonographic clue to the diagnosis of fetal ovarian cyst. Ultrasound Obstet Gynecol 2003; 22 (04) 433-434
- 11 Fung TY, Leung TN, Leung TY, Lau TK. Fetal intra-abdominal umbilical vein varix: what is the clinical significance?. Ultrasound Obstet Gynecol 2005; 25 (02) 149-154
- 12 Ozkose ZG, Suzen Caypinar S, Bestel A, Ozdemir O. Predictive value of prenatal ultrasound in foetal intraabdominal cystic lesions and evaluation of perinatal outcomes: a single-centre study results. J Obstet Gynaecol 2022; 42 (07) 2659-2664
- 13 Sauvat F, Sarnacki S, Brisse H. et al. Outcome of suprarenal localized masses diagnosed during the perinatal period: a retrospective multicenter study. Cancer 2002; 94 (09) 2474-2480
- 14 Sanna E, Loukogeorgakis S, Prior T. et al. Fetal abdominal cysts: antenatal course and postnatal outcomes. J Perinat Med 2019; 47 (04) 418-421
- 15 Garcia-Aguilar P, Maiz N, Rodó C. et al. Fetal abdominal cysts: predicting adverse outcomes. Acta Obstet Gynecol Scand 2023; 102 (07) 883-890
- 16 Lv M, Zhao B, Luo Q. Prenatal diagnosis and prognosis assessment of fetal intra-abdominal cystic lesions: a retrospective study in 264 cases. J Obstet Gynaecol 2019; 39 (07) 922-927
- 17 Casale AJ. Early ureteral surgery for posterior urethral valves. Urol Clin North Am 1990; 17 (02) 361-372
- 18 Liao AW, Sebire NJ, Geerts L, Cicero S, Nicolaides KH. Megacystis at 10-14 weeks of gestation: chromosomal defects and outcome according to bladder length. Ultrasound Obstet Gynecol 2003; 21 (04) 338-341
- 19 Viora E, Sciarrone A, Bastonero S, Errante G, Campogrande M. Thrombosis of umbilical vein varix. Ultrasound Obstet Gynecol 2002; 19 (02) 212-213
Address for correspondence
Publication History
Article published online:
09 January 2026
© 2026. Society of Fetal Medicine. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Snijders RJ, Noble P, Sebire N, Souka A, Nicolaides KH. Fetal Medicine Foundation First Trimester Screening Group. UK multicentre project on assessment of risk of trisomy 21 by maternal age and fetal nuchal-translucency thickness at 10-14 weeks of gestation. Lancet 1998; 352 (9125) 343-346
- 2 Nicolaides KH. Nuchal translucency and other first-trimester sonographic markers of chromosomal abnormalities. Am J Obstet Gynecol 2004; 191 (01) 45-67
- 3 Souka AP, Pilalis A, Kavalakis Y, Kosmas Y, Antsaklis P, Antsaklis A. Assessment of fetal anatomy at the 11-14-week ultrasound examination. Ultrasound Obstet Gynecol 2004; 24 (07) 730-734
- 4 Malone FD, Canick JA, Ball RH. et al; First- and Second-Trimester Evaluation of Risk (FASTER) Research Consortium. First-trimester or second-trimester screening, or both, for Down's syndrome. N Engl J Med 2005; 353 (19) 2001-2011
- 5 Gabrielli S, Rizzo N, Reece EA. Gastrointestinal and genitourinary anomalies. In: Reece EA, Hobbins JC. eds. Clinical Obstetrics. The Fetus & Mother. 3rd ed.. Malden, MA: Blackwell Publishing; 2007: 377-400
- 6 Hyett J. Intra-abdominal masses: prenatal differential diagnosis and management. Prenat Diagn 2008; 28 (07) 645-655
- 7 McEwing R, Hayward C, Furness M. Foetal cystic abdominal masses. Australas Radiol 2003; 47 (02) 101-110
- 8 Nyberg DA, Neilson IR. Abdomen and gastrointestinal tract. In: Nyberg DA, McGahan JP, Pretorius DH, Pilu G. eds. Diagnostic Imaging of Fetal Anomalies. Philadelphia, PA: Lippincott Williams & Wilkins; 2003: 547-602
- 9 Hill LM. Ultrasound of fetal gastrointestinal tract. In: Callen PW. ed. Ultrasonography in Obstetrics and Gynecology. 4th ed.. Philadelphia, PA: W. B. Saunders; 2000: 457-487
- 10 Quarello E, Gorincour G, Merrot T, Boubli L, D'Ercole C. The ‘daughter cyst sign’: a sonographic clue to the diagnosis of fetal ovarian cyst. Ultrasound Obstet Gynecol 2003; 22 (04) 433-434
- 11 Fung TY, Leung TN, Leung TY, Lau TK. Fetal intra-abdominal umbilical vein varix: what is the clinical significance?. Ultrasound Obstet Gynecol 2005; 25 (02) 149-154
- 12 Ozkose ZG, Suzen Caypinar S, Bestel A, Ozdemir O. Predictive value of prenatal ultrasound in foetal intraabdominal cystic lesions and evaluation of perinatal outcomes: a single-centre study results. J Obstet Gynaecol 2022; 42 (07) 2659-2664
- 13 Sauvat F, Sarnacki S, Brisse H. et al. Outcome of suprarenal localized masses diagnosed during the perinatal period: a retrospective multicenter study. Cancer 2002; 94 (09) 2474-2480
- 14 Sanna E, Loukogeorgakis S, Prior T. et al. Fetal abdominal cysts: antenatal course and postnatal outcomes. J Perinat Med 2019; 47 (04) 418-421
- 15 Garcia-Aguilar P, Maiz N, Rodó C. et al. Fetal abdominal cysts: predicting adverse outcomes. Acta Obstet Gynecol Scand 2023; 102 (07) 883-890
- 16 Lv M, Zhao B, Luo Q. Prenatal diagnosis and prognosis assessment of fetal intra-abdominal cystic lesions: a retrospective study in 264 cases. J Obstet Gynaecol 2019; 39 (07) 922-927
- 17 Casale AJ. Early ureteral surgery for posterior urethral valves. Urol Clin North Am 1990; 17 (02) 361-372
- 18 Liao AW, Sebire NJ, Geerts L, Cicero S, Nicolaides KH. Megacystis at 10-14 weeks of gestation: chromosomal defects and outcome according to bladder length. Ultrasound Obstet Gynecol 2003; 21 (04) 338-341
- 19 Viora E, Sciarrone A, Bastonero S, Errante G, Campogrande M. Thrombosis of umbilical vein varix. Ultrasound Obstet Gynecol 2002; 19 (02) 212-213