

Subscribe to RSS
DOI: 10.1055/s-0044-1788046
Ureaplasma urealyticum as a Cause of Ventriculitis in an Extremely Low Birth Weight Infant
Authors

Abstract
Ureaplasma urealyticum (Uu) has rarely been described as a cause of ventriculitis in preterm infants. We report a preterm infant in whom Uu was detected in the tracheal secretion. Concurrent intraventricular hemorrhage III° with posthemorrhagic hydrocephalus occurred, necessitating the bilateral insertion of ventriculostomy access devices for treatment. Persisting high cerebrospinal fluid (CSF) protein and pleocytosis in the otherwise clinically unremarkable neonate subsequently led to the targeted detection of Uu in the CSF. Normalization of CSF parameters occurred only after prolonged intravenous and oral macrolide therapy.
Bacteria of the genus Ureaplasma represent frequent commensals in the lower genital tract of sexually active women. In the context of perinatal medicine, ascending Ureaplasma infections are relevant triggers of chorioamnionitis, which itself is one of the main risk factors for preterm birth.[1] Of the two known Ureaplasma species, Ureaplasma parvum and Ureaplasma urealyticum (Uu), U. parvum is more frequently detected in cases of chorioamnionitis, preterm birth, and neonatal CNS infections.[2] Neonatal colonization results in increased morbidity, particularly due to the development of congenital pneumonia, septicemia, and meningitis, as well as increased overall mortality.[3] Respiratory colonization with Uu in extremely low birth weight infants (ELBWI) increases the risk of developing bronchopulmonary dysplasia (BPD).
Only single-case reports of Ureaplasma meningitis or central nervous infections in preterm are available.[4] [5] [6] [7] Animal models have demonstrated mechanisms which may be indicative of an impaired blood-brain barrier after Ureaplasma exposure and may thus promote neuroinflammation.[8]
Case Presentation
We report on an ELBWI born by caesarean section at 245/7 weeks of gestation with a birth weight of 630 g. Postnatal care was initially uncomplicated in the context of prematurity; surfactant (porcine) application was administered after endotracheal intubation. Invasive ventilation via endotracheal tube was necessary until the 26th day of life (DOL), followed by noninvasive ventilation up to 51st DOL. In view of postnatal detection after routine testing of Uu by targeted polymerase chain reaction (PCR) in tracheal secretion (TS), macrolide therapy (azithromycin 10 mg/kg, p.o. over 5d) was initiated in the first week of life. Serum CRP, serum IL-6, and white blood cell count (WBC) were unremarkable. There were neither typical clinical symptoms of a Uu infection of the respiratory tract nor any signs of BPD in the chest X-rays that were taken repetitively.
On the third DOL, bilateral IVH III° with parenchymal involvement was diagnosed on routine cranial ultrasound (CUS). Progressive posthemorrhagic ventricular dilatation (PHVD) was developed and managed with three consecutive lumbar punctures in the 3rd week of life. Considering progressive PHVD and suspected blockage of the foramen of Monro, bilateral insertion of ventriculostomy access devices' (VAD's) placed in both lateral horns was performed on the 23rd DOL. Following daily CSF drainage via VAD's, ventricular width was stable. The CSF volume taken was adjusted to the ventricular width according to sonographic findings. The CSF was examined twice weekly by conventional microbiology (not for Uu) and CSF biochemistry marker (protein, glucose, lactate, and WBC).
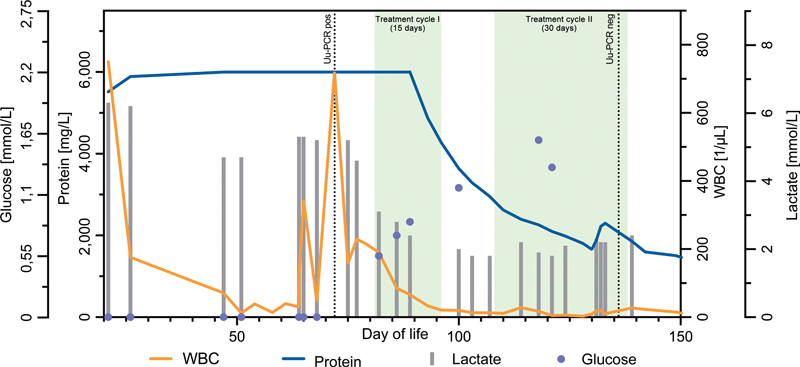
On the 65th DOL, the CSF showed granulocytic pleocytosis (344 cells per µL, 85% granulocytes) with persistent high protein levels, which further increased on the 72nd DOL (721 cells per µL, 85% granulocytes) ([Fig. 1]). CSF culture and multiplex PCR of the CSF (BioFire FilmArray ME Panel, used 2022) failed to detect any microorganisms. On CUS, membranes in the lateral ventricles were detected at this time, first on the right and later on the left side ([Fig. 2]).

Serum CRP and IL-6 measurement did not reveal systemic inflammation and conventional CSF microbiology was negative. In view of the clinical picture of ventriculitis, intrathecal administration of vancomycin (5 mg each) was performed on the 65th DOL via the right VAD and on the 72nd and 77th DOL via the left VAD.[9] CSF pleocytosis and protein elevation persisted during therapy, and microbial cultures remained negative. The clinical condition was always stable.
Uu was detected by specific PCR in the CSF and in the oro-pharyngeal secretion (OPS). Microbiological CSF cultural testing for Uu performed in a reference laboratory to assess antimicrobial susceptibility was unsuccessful. For the treatment of suspected Uu ventriculitis macrolide therapy with clarithromycin (10 mg/kg body weight, intravenously for 10 days, then p.o. for 5 days) was administered starting on the 81st DOL, 64 days after the completion of the first macrolide therapy. An attempt of therapeutic drug monitoring (TDM) was made but yielded undetectable levels of clarithromycin in the CSF.
Nonetheless, a decrease in WBC and protein levels in the CSF (from > 6,000 to 4,500 mg/L on day 15 of therapy) was eventually observed under the targeted therapy. Molecular biology continued to detect Ureaplasma DNA during therapy. Although DNA detection does not equal the presence of vital and reproducing bacteria (cultures remained negative), we decided to start a second cycle of oral therapy for 30 days, until negative Uu-PCR results were obtained from CSF, to achieve safe eradication. The protein level in the CSF further decreased to 1,900 mg/L. Clarithromycin treatment showed no adverse effects, even during prolonged therapy. There were no QT prolongation, cardiac arrhythmias, or significant interactions with other drugs due to CYP3A4 inhibition. Additionally, no hepatotoxic or nephrotoxic effects were observed. In addition to Uu therapy, apart from the prophylactic administration of an antibiotic for PPROM for 3 days within the first 14 days, empirical single administration was necessary twice in the context of clinical deterioration until the infection was ruled out. Magnetic resonance imagings of the brain performed two times (on 114th and 195th dol) showed the findings already known from the sonography.
At the time of discharge, at the corrected age of 4 months, neurological examination demonstrated unremarkable early childhood movement pattern, mild generalized muscular hypotonia with trunk instability and only short phases of head control, and unremarkable newborn reflexes; regardless of the necessity of a ventriculoperitonal shunt.
Discussion
Clinical symptoms, like a bulging fontanel as well as unexpected additional findings on CUS, as demonstrated in this case, may be indicative of an infectious process, notably of device-associated bacterial ventriculitis, and should prompt further investigation. Gram-positive bacteria, such as staphylococci, are the most common cause of device-associated ventriculitis, with an incidence of 6% reported in the literature.[10] No incidence can be given for Uu-ventriculitis due to the few cases described so far.[4] [5] [6] [7] Molecular or cultural detection of Uu in CSF in cases of suspected CNS infection is not routinely performed. Nevertheless, in the setting of culture-negative ventriculitis characterized by elevated WBC and persistently high CSF protein levels despite regular CSF drainage via VAD, a targeted investigation for non-culturable pathogens should be performed, especially in patients with a history of colonization with Uu. Even though Uu has long been known as a pathogen associated with premature birth and CNS infections,[11] a long time usually elapses before a diagnosis is established.[4] [7] This is because these cell wall-less bacteria cannot be cultured with conventional methods in routine laboratories, and appropriate detection methods (targeted PCR for urogenital Ureaplasma and Mycoplasma spp.) are only requested based on clinical suspicion. In addition, the usual empirical therapy regimens in suspected ventriculitis do not cover atypic bacteria like Ureaplasma. The possible therapeutic approaches for covering Ureaplasma are associated with relevant adverse drug reactions in infants; for example, doxycycline leads to permanent tooth damage, and fluoroquinolones can lead to tendon inflammation and rupture.[12] The treatment of CNS infections with macrolides is the subject of controversy. Erythromycin shows poor CSF penetration and is known to be associated with hypertrophic pyloric stenosis[13]; azithromycin, on the other hand, penetrates sufficiently but, like all macrolides, achieves low CSF levels due to the rapid distribution and accumulation in brain tissue.[14] Evidence regarding antibiotic choice and duration of therapy is limited to case reports or small case series.[6] [7] Spontaneous remission has been reported even without Ureplasma-specific antibiotic administration.[11]
Regarding tracheal colonization with Uu, routines for both diagnosis and therapy have already been established in most neonatal intensive care unit. As a general practice, macrolides are used as an oral formulation. For eradication with azithromycin, differences between centers exist regarding the administered dosage.[15] Consideration should be given to standard monitoring of the success of eradication therapy when Uu is detected in the TS or OPS, as persistent colonization is a potential source of CNS infection. Lastly, it remains unclear in this case whether it is a case of inadequate eradication or reinfection.
To date, it is unknown how Ureaplasma spp. infiltrate the central nervous system, but a disrupted blood-brain barrier appears to be associated with infection.[11] In this context, barrier disruption may be primarily caused by infection with Ureaplasma spp,[8] but it may also occur as a consequence of inflammatory processes following events such as intracerebral hemorrhage, thus facilitating the translocation of bacteria.[16]
Increased permeability of the blood-brain barrier could explain the efficacy of clarithromycin in our case, although in the literature it has been described as having little or no CSF penetration.[17] However, attempting to quantify drug levels in CSF with TDM did not yield measurable levels in our case. This may be due to the rapid distribution of macrolides from fluid into tissue. In addition, no established and standardized TDM protocols are available for clarithromycin which would specify the ideal sampling time relative to drug administration as well as storage and transport conditions. Finally, studies correlating detected CSF drug levels to clinical outcomes are lacking. Overall, the benefit of TDM for clarithromycin in CSF is not yet determined.
Conclusion
Ureaplasma urealyticum (Uu) is a rare causative agent of ventriculitis in preterm infants. Unlike fulminant infections caused by gram-positive or gram-negative pathogens, Uu infections are usually subclinical or even asymptomatic. Therefore, CSF changes indicative or compatible with infection and not improving under empirical antimicrobial therapy should prompt a targeted investigation for Ureaplasma, especially in infants with previously diagnosed colonization with Ureaplasma in TS. In the case described here, prolonged therapy with clarithromycin led to therapeutic success. Consequent eradication of Ureaplasma in the TS or OPS with subsequent monitoring of success could contribute to reducing the risk of central nervous infection.
Conflict of Interest
None declared.
-
References
- 1 Murtha AP, Edwards JM. The role of mycoplasma and Ureaplasma in adverse pregnancy outcomes. Obstet Gynecol Clin North Am 2014; 41 (04) 615-627
- 2 Stol K, Jans J, Ott de Bruin L, Unger W, van Rossum A. Perinatal infections with Ureaplasma. Pediatr Infect Dis J 2021; 40 (5S): S26-S30
- 3 Sprong KE, Mabenge M, Wright CA, Govender S. Ureaplasma species and preterm birth: current perspectives. Crit Rev Microbiol 2020; 46 (02) 169-181
- 4 Glaser K, Wohlleben M, Speer CP. An 8-month history of meningitis in an extremely low birth weight infant? Long-lasting infection with Ureaplasma parvum. Z Geburtshilfe Neonatol 2015; 219 (01) 52-56
- 5 Xing N, Zhao Z, Li Q, Dong Y, Li J, Zhang S. Ureaplasma parvum meningitis following atypical choroid plexus papilloma resection in an adult patient: a case report and literature review. BMC Infect Dis 2021; 21 (01) 1276
- 6 Zhan C, Chen L, Hu L. Neonatal Ureaplasma parvum meningitis complicated with subdural hematoma: a case report and literature review. BMC Infect Dis 2021; 21 (01) 268
- 7 Duan J, Zhang C, Wang J. et al. Diagnosis of Ureaplasma parvum meningitis by mNGS in an extremely low birth weight infant with multi-system lesions. Indian J Med Microbiol 2022; 40 (03) 455-458
- 8 Silwedel C, Hütten MC, Speer CP. et al. Ureaplasma-driven neonatal neuroinflammation: novel insights from an ovine model. Cell Mol Neurobiol 2023; 43 (02) 785-795
- 9 Parasuraman JM, Albur M, Fellows G, Heep A. Monitoring intraventricular vancomycin for ventriculostomy access device infection in preterm infants. Childs Nerv Syst 2018; 34 (03) 473-479
- 10 de Vries LS, Groenendaal F, Liem KD. et al; ELVIS study group. Treatment thresholds for intervention in posthaemorrhagic ventricular dilation: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed 2019; 104 (01) F70-F75
- 11 Clifford V, Tebruegge M, Everest N, Curtis N. Ureaplasma: pathogen or passenger in neonatal meningitis?. Pediatr Infect Dis J 2010; 29 (01) 60-64
- 12 Beeton ML, Spiller OB. Antibiotic resistance among Ureaplasma spp. isolates: cause for concern?. J Antimicrob Chemother 2017; 72 (02) 330-337
- 13 Almaramhy HH, Al-Zalabani AH. The association of prenatal and postnatal macrolide exposure with subsequent development of infantile hypertrophic pyloric stenosis: a systematic review and meta-analysis. Ital J Pediatr 2019; 45 (01) 20
- 14 Jaruratanasirikul S, Hortiwakul R, Tantisarasart T, Phuenpathom N, Tussanasunthornwong S. Distribution of azithromycin into brain tissue, cerebrospinal fluid, and aqueous humor of the eye. Antimicrob Agents Chemother 1996; 40 (03) 825-826
- 15 Chang E, Ballard KE, Johnson PN, Nandyal R, Miller JL. Azithromycin for eradication of Ureaplasma and prevention of bronchopulmonary dysplasia in preterm neonates in the neonatal intensive care unit. J Pediatr Pharmacol Ther 2023; 28 (01) 10-19
- 16 Del Pozo A, Villa M, Vargas C. et al. Intraventricular hemorrhage induces inflammatory brain damage with blood-brain barrier dysfunction in immature rats. Pediatr Res 2023; 93 (01) 78-88
- 17 Rodvold KA. Clinical pharmacokinetics of clarithromycin. Clin Pharmacokinet 1999; 37 (05) 385-398
Address for correspondence
Publication History
Received: 09 January 2024
Accepted: 10 June 2024
Article published online:
03 July 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Murtha AP, Edwards JM. The role of mycoplasma and Ureaplasma in adverse pregnancy outcomes. Obstet Gynecol Clin North Am 2014; 41 (04) 615-627
- 2 Stol K, Jans J, Ott de Bruin L, Unger W, van Rossum A. Perinatal infections with Ureaplasma. Pediatr Infect Dis J 2021; 40 (5S): S26-S30
- 3 Sprong KE, Mabenge M, Wright CA, Govender S. Ureaplasma species and preterm birth: current perspectives. Crit Rev Microbiol 2020; 46 (02) 169-181
- 4 Glaser K, Wohlleben M, Speer CP. An 8-month history of meningitis in an extremely low birth weight infant? Long-lasting infection with Ureaplasma parvum. Z Geburtshilfe Neonatol 2015; 219 (01) 52-56
- 5 Xing N, Zhao Z, Li Q, Dong Y, Li J, Zhang S. Ureaplasma parvum meningitis following atypical choroid plexus papilloma resection in an adult patient: a case report and literature review. BMC Infect Dis 2021; 21 (01) 1276
- 6 Zhan C, Chen L, Hu L. Neonatal Ureaplasma parvum meningitis complicated with subdural hematoma: a case report and literature review. BMC Infect Dis 2021; 21 (01) 268
- 7 Duan J, Zhang C, Wang J. et al. Diagnosis of Ureaplasma parvum meningitis by mNGS in an extremely low birth weight infant with multi-system lesions. Indian J Med Microbiol 2022; 40 (03) 455-458
- 8 Silwedel C, Hütten MC, Speer CP. et al. Ureaplasma-driven neonatal neuroinflammation: novel insights from an ovine model. Cell Mol Neurobiol 2023; 43 (02) 785-795
- 9 Parasuraman JM, Albur M, Fellows G, Heep A. Monitoring intraventricular vancomycin for ventriculostomy access device infection in preterm infants. Childs Nerv Syst 2018; 34 (03) 473-479
- 10 de Vries LS, Groenendaal F, Liem KD. et al; ELVIS study group. Treatment thresholds for intervention in posthaemorrhagic ventricular dilation: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed 2019; 104 (01) F70-F75
- 11 Clifford V, Tebruegge M, Everest N, Curtis N. Ureaplasma: pathogen or passenger in neonatal meningitis?. Pediatr Infect Dis J 2010; 29 (01) 60-64
- 12 Beeton ML, Spiller OB. Antibiotic resistance among Ureaplasma spp. isolates: cause for concern?. J Antimicrob Chemother 2017; 72 (02) 330-337
- 13 Almaramhy HH, Al-Zalabani AH. The association of prenatal and postnatal macrolide exposure with subsequent development of infantile hypertrophic pyloric stenosis: a systematic review and meta-analysis. Ital J Pediatr 2019; 45 (01) 20
- 14 Jaruratanasirikul S, Hortiwakul R, Tantisarasart T, Phuenpathom N, Tussanasunthornwong S. Distribution of azithromycin into brain tissue, cerebrospinal fluid, and aqueous humor of the eye. Antimicrob Agents Chemother 1996; 40 (03) 825-826
- 15 Chang E, Ballard KE, Johnson PN, Nandyal R, Miller JL. Azithromycin for eradication of Ureaplasma and prevention of bronchopulmonary dysplasia in preterm neonates in the neonatal intensive care unit. J Pediatr Pharmacol Ther 2023; 28 (01) 10-19
- 16 Del Pozo A, Villa M, Vargas C. et al. Intraventricular hemorrhage induces inflammatory brain damage with blood-brain barrier dysfunction in immature rats. Pediatr Res 2023; 93 (01) 78-88
- 17 Rodvold KA. Clinical pharmacokinetics of clarithromycin. Clin Pharmacokinet 1999; 37 (05) 385-398