

RSS-Feed abonnieren
DOI: 10.1055/s-0043-124872
Comparative Efficacy and Safety of Antipsychotic Drugs for Tic Disorders: A Systematic Review and Bayesian Network Meta-Analysis
Authors
Correspondence
Publikationsverlauf
received 02. September 2017
revised 04. Dezember 2017
accepted 10. Dezember 2017
Publikationsdatum:
05. März 2018 (online)

Abstract
Objective The purpose of this study was to evaluate the efficacy and safety of antipsychotic drugs for tic disorders (TDs) in a network meta-analysis.
Methods PubMed, Embase, Cochrane Library, and 4 Chinese databases were searched. Randomized controlled trials (RCTs) evaluating the efficacy of antipsychotic drugs for TDs were included.
Results Sixty RCTs were included. In terms of tic symptom score, compared with placebo, haloperidol, risperidone, aripiprazole, quetiapine, olanzapine, and ziprasidone can significantly improve tic symptom score (standardized mean differences [SMD] ranged from −12.32 to −3.20). Quetiapine was superior to haloperidol, pimozide, risperidone, tiapride, aripiprazole, and penfluridol for improving tic symptom score (SMD ranged from −28.24 to −7.59). Compared with tiapride, aripiprazole could significantly improve tic symptom score (SMD=−4.27). Compared with all other drugs, penfluridol was not effective. Atypical antipsychotics were generally well tolerated.
Conclusions Atypical antipsychotics (risperidone and aripiprazole) appear to be the most robust evidence-based options for the treatment of TDs. Quetiapine may be a promising therapy. Ziprasidone and olanzapine are also effective, but the evidence is lacking. Further high-quality directly comparing different pharmacological treatment studies are justified.
Introduction
Tic disorders (TDs) are common, childhood-onset, neuropsychiatric disorders with variable severity and prognosis, which are characterized by sudden, repetitive, nonrhythmic motor movement or vocalization [1]. TDs are classified into transient tic disorder (TTD), chronic tic disorder (CTD), and Tourette syndrome (TS) by duration and severity [2]. Symptoms of common comorbidities of TDs (i. e., attention-deficit hyperactivity disorder, obsessive-compulsive disorder, pervasive developmental disorder, and other mood disorders) often coexist [3]. Tics and co-occurring conditions have been associated with functional impairment and diminished quality of life, for instance by affecting subjective discomfort (i. e., pain or injury), sleep quality, and emotional status (i. e., anxiety or depression), and can cause sustained social problems (i. e., social isolation or bullying) especially in severe cases [4] [5] [6] [7]. Knight’s study presented that the prevalence of TS is 0.77%. TTD is the most common TD, with a prevalence of 2.99%, and CTD has a prevalence of 1.61% [8].
Motor/vocal tics and comorbid symptoms are often managed by pharmacotherapy. Antipsychotic drugs are commonly used in the treatment of TDs, including typical antipsychotic drugs (i. e., haloperidol, pimozide) and atypical antipsychotic drugs (i. e., risperidone, aripiprazole, quetiapine) [6] [9] [10]. A number of randomized controlled trials (RCTs) and systematic reviews evaluating the efficacy of antipsychotic drugs for TDs have been published [11] [12] [13] [14]. In our previous overview including 22 systematic reviews for treating TDs, we found some antipsychotics were efficacious in the reduction of tic severity; however, RCTs directly comparing different pharmacological treatment options for TDs are scarce [15].
Bayesian network meta-analysis is known as mixed treatment comparison, and it could combine direct and indirect evidence from multiple treatment comparisons to estimate the interrelations across all treatments, which allows the simultaneous comparison of multiple antipsychotic drugs within a single analysis while preserving randomization [16]. Multiple genes interacting with environmental factors could lead to the onset of symptoms, and multiple genes and chromosomal regions have been implicated in TS etiology, with SLITRK1 being the most prominent example [17]. If we screen out some antipsychotic treatments with better efficacy through indirect comparison, it could provide reference for the precise treatment for TDs from gene perspective.
Therefore, we aimed to provide a comprehensive and hierarchical evidence of the efficacy and safety of antipsychotic drugs in the treatment of TDs.
Methods
Inclusion and exclusion criteria
Types of studies
Only RCTs, including crossover and cluster randomized trials, evaluating the efficacy and safety of antipsychotic drugs for the treatment of TDs were included. We planned to use only data from the first period of any included crossover trials. Trials were excluded if (1) the same study was published in different languages and if (2) they compared different doses of drugs—that is, the treatment group used high (or low) doses and the control group used low (or high) doses.
Types of participants
We focused on the patients with clinical diagnoses of TDs who met the following diagnosis criteria: (1) the Diagnostic and Statistical Manual of Mental Disorders-III (DSM-III), DSM-IV, or DSM-IV-Text Revision [18] [19] [20]; (2) the International Classification of Diseases-10 (ICD-10) [21]; and (3) the Chinese Classification and Diagnostic Criteria of Mental Disorders (CCMD) [22].
Types of interventions and controls
The interventions are all antipsychotic drugs, including typical antipsychotic drugs (i. e., haloperidol, tiapride, pimozide, penfluridol, fluphenazine) and atypical antipsychotic drugs (risperidone, olanzapine, aripiprazole, quetiapine, ziprasidone, paliperidone, sulpiride, tetrabenazine). The controls are also all antipsychotic drugs.
Types of outcome measurements
The primary outcome was the efficacy at post-treatment, as measured by mean change scores in tic severity symptoms from baseline to post-treatment. When an included study used more than 1 scale, the Yale Global Tic Severity Scale (YGTSS) was used as the primary measure, as it is the more commonly-used measure of tic severity symptoms [23], followed by the Clinical Global Impression (CGI) Scale [19], the Tourette Syndrome Global Scale (TSGS) [19], the Tourette Syndrome Severity Scale (TSSS), or other scales [24]. We used these scales in this order through published research and expert opinion in our hospital.
The secondary outcomes were the response and the reported adverse events (AEs). The response was defined as a reduction of 50% or more in scores from baseline to post-treatment on the tic severity symptoms.
Search strategy
The following databases were searched from their respective inceptions up to January 2017 by 2 reviewers (Yang and Hao): PubMed, EMBASE, the Cochrane Library, Cochrane Controlled Trials databases (CENTRAL), the Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI,), the Chinese Science and Technique Journals Database (VIP), and the Wanfang Database (http://www.wanfangdata.com/). We also searched the additional studies in the reference lists of all identified publications, including relevant meta-analyses and systematic reviews. The following search terms were used: “Tourette syndrome,” “tic disorders,” “Tourette disorders,” “haloperidol,” “tiapride,” “pimozide,” “penfluridol,” “risperidone,” “olanzapine,” “aripiprazole,” “quetiapine,” “ziprasidone,” “paliperidone,” “sulpiride,” “fluphenazine,” “tetrabenazine,” “antipsychotics,” “typical antipsychotics,” and “atypical antipsychotics.”
Selection of studies and data extraction
Two reviewers (Yang and Hao) independently screened the titles and abstracts of every record. Full articles were obtained when either information provided in the title or abstracts conformed to the selection criteria outlined previously or could not be ascertained because of limited information. To include studies, data were independently extracted by each reviewer and entered into a standardized form. The data extraction form included the following contents: (1) general characteristics of studies, (2) the general characteristics of patients, (3) the diagnostic criteria, (4) sample size, (5) interventions and comparisons, (6) outcome measurements, and (7) AEs. Discrepancies were resolved by consensus.
Quality assessment
Two reviewers (Yang and Hao) independently evaluated the methodological quality of identified studies using the “risk of bias tool” under the domains of 6 aspects, including (1) sequence generation, (2) allocation concealment, (3) blinding, (4) incomplete outcome data, (5) selective outcome, and (6) other biases. The methodological criteria referred to the Cochrane Handbook for Systematic Reviews of Interventions version 5.3 [25].
Statistical methods
First, we performed traditional meta-analysis for studies that directly compared different treatment arms. Results for dichotomous outcomes are expressed as risk ratios (RR) with 95% confidence intervals (CIs). Results for continuous outcomes are expressed as the standardized mean difference (SMD). We evaluated heterogeneity among the included studies using the I² test. Regardless of the size of heterogeneity, the random effects model was used for statistical analysis. We conducted the meta-analysis using STATA 12.0 (Stata Corporation, College Station, Texas, USA). Publication bias was examined with the funnel plot method and the Egger’s regression asymmetry test [26].
Then we performed Bayesian network meta-analyses to compare different antipsychotic drugs with a random-effects model within a Bayesian framework [27]. The pooled estimates of SMD with 95% CIs were calculated for continuous outcomes, and odds ratios (ORs) with 95% CIs for categorical outcomes. The pooled estimates were obtained using the Markov chain Monte Carlo method. Three Markov chains were run simultaneously with different arbitrarily chosen initial values [27]. To ensure convergence, trace plots were assessed [28]. A run-in period of 50,000 iterations was adequate to achieve convergence, and a further 100,000 samples were taken. Inconsistency refers to differences between direct and various indirect effect estimates for the same comparison. To assess inconsistency, we estimated the inconsistency factors in closed loop based on the method described by Chaimani et al. [29]. Probability values were summarized and reported as surface under the cumulative ranking curve (SUCRA) and rankograms. A higher SUCRA value suggests better results for respective treatment method. Moreover, network meta-regression analyses were used to investigate whether potential heterogeneity could be explained by differences in publication year and sample sizes. We will select better model for the network meta-analysis based on deviance information criterion. Results from intention-to-treat (ITT) analysis or modified ITT were preferred over results from completer analyses.
Network meta-analyses were performed using the WinBUGS software package (MRC Biostatistics Unit, Cambridge, UK) with random effects models for multi-arm trials. The other analyses were performed and presented by the Stata 12.0 software packages (Stata Corporation, College Station, Texas, USA).
The first sensitivity analysis was performed on a network excluding trials with small sample sizes (n<20 patients), and the second sensitivity analysis was performed by omitting trials with long-term treatment period (treatment period>24 weeks).
Results
Results of the literature search
The literature search process identified a total of 6312 potentially relevant articles. After removing duplicates, screening titles and abstracts, and reading full texts, 60 RCTs met the inclusion criteria ([Fig. 1]).

The characteristics of the included studies (Table S1)
We included 60 studies involving 4077 participants. The sample size of included RCTs ranged from 4 to 180 (median 61). The location of the first author had the following distribution: China (47/60, 78.3%), United States (7/60, 11.7%), Canada (2/60, 3.3%), South Korea (1/60, 1.7%), Iran (1/60, 1.7%), Italy (1/60, 1.7%), and South Africa (1/60, 1.7%). Only 4 trials were multicenter RCTs. Fifty-one studies were positive drug controls, and 9 studies used a placebo as a control. This study included 11 different types of antipsychotic agents: haloperidol (n=44 RCTs), risperidone (n=23 RCTs), aripiprazole (n=15 RCTs), tiapride (n=14 RCTs), pimozide (n=8 RCTs), quetiapine (n=4 RCTs), olanzapine (n=3 RCTs), ziprasidone (n=2 RCTs), paliperidone (n=1 RCT), penfluridol (n=1 RCT), and sulpiride (n=1 RCT). The period of treatment ranged from 3 weeks to 20 months.
Characteristics of participants (Table S1)
The age of participants ranged from 2 to 65 years. Two categories of disorders were examined: TS (43/60, 71.7%) and TDs (17/60, 28.3%). The diagnostic criteria used were as follows: CCMD (22/60, 36.7%), DSM-IV (17/60, 28.3%), ICD-10 (5/60, 8.3%), DSM-III (4/60, 6.7%), DSM-III-R (3/60, 5%), DSM-IV-TR (2/60, 3.3%), both DSM-IV and CCMD-3 (1/60, 1.7%), and both DSM-IV-TR and CCMD-3(1/60, 1.7%). The diagnostic criteria were not mentioned in 5 studies (5/60, 8.3%).
Primary outcome measurements
The majority of the included RCTs (37/60, 61.7%) used the YGTSS as the primary outcome measurement, and other outcome measurements used in the included studies were the response rate (36/60, 60%), the CGI Scale (4/60, 6.7%), the TSGS (3/60, 5%), the TSSS (2/60, 3.3%), and tic counts (1/60, 1.7%). Ninety-five percent (57/60) of included studies reported on AEs of treatment, of which 42 studies reported specific AEs.
Quality assessment
Twenty-five percent (15/60) of studies used an adequate method of random sequence generation. Ten percent (6/60) of studies implemented adequate allocation concealment, and 25% (15/60) used the methods of blinding. Eight percent (5/60) of studies reported loss to follow-up, and none of the studies used an ITT analysis for incomplete outcome data. Only 5% (3/60) of studies had registration for a protocol. Comparability of baseline in 4 of the studies was unclear. In other trials, there were no significant differences in the comparability of baseline between the treatment group and the control group.
Results of pairwise meta-analyses
Table S2 presents the results of the pairwise meta-analyses. Compared with haloperidol, risperidone, aripiprazole, quetiapine, tiapride, pimozide, olanzapine, paliperidone, and ziprasidone could improve tic symptoms score, but there were no significantly difference between them. Haloperidol and risperidone could significantly improve tic symptoms scores compared with placebo, and pimozide also could improve tic symptoms scores, but there were no significantly difference between them. Aripiprazole was superior to tiapride in the improvement of tic symptoms, and there was significantly difference between them.
In terms of response rate, quetiapine was superior to haloperidol in the improvement of tic symptoms, and there were significantly difference between them. Compared with haloperidol, risperidone, tiapride, aripiprazole, olanzapine, ziprasidone, paliperidone, and pimozide could improve tic symptoms, but there were no significantly difference between them. Compared with tiapride, aripiprazole and risperidone could improve the tic symptoms, but there was no significantly difference between them. Compared with risperidone, aripiprazole could improve the tic symptoms, but there were no significantly difference between them (Table S3).
Results of network meta-analysis
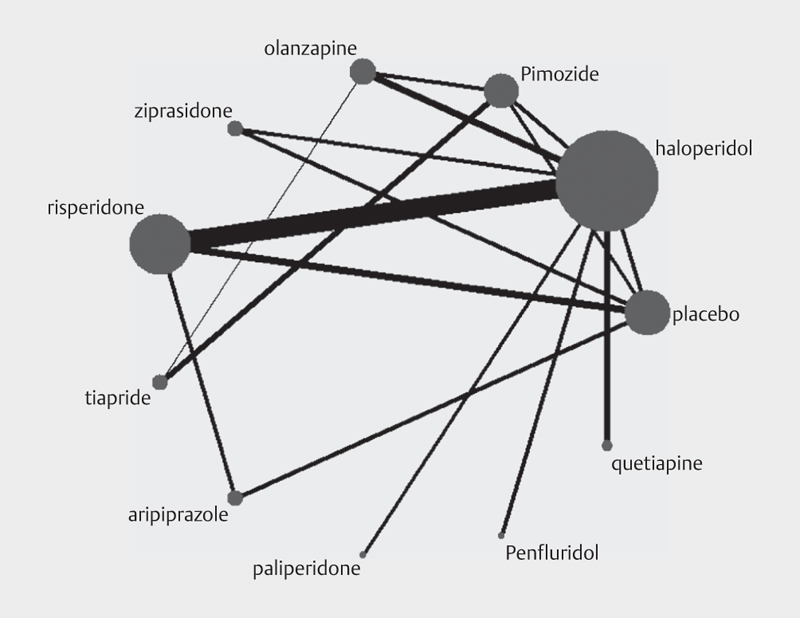
In regard to the primary outcome, we included 39 RCTs involving 2417 participants for network meta-analysis. There were 11 comparisons of primary outcome in the network plot of different types of antipsychotic agents ([Fig. 2]). In the network plot of eligible comparisons for outcomes, the connecting line represented that there was a direct comparison between 2 kinds of interventions. The thickness of the line represents the number of included studies, and the dot size represents the total sample size of interventions. The pooled effect estimates for primary efficacy from the network meta-analysis are provided ([Fig. 4]). Compared with placebo, haloperidol (SMD=−3.20, 95% CI [−6.52, −0.14]), olanzapine (SMD=−6.11, 95% CI [−11.86, 0.55]), ziprasidone (SMD=−5.57, 95% CI [−11.15, −0.048]), risperidone (SMD=−3.47, 95% CI [−6.87, −0.37]), aripiprazole (SMD=−4.74, 95% CI [−8.67, −1.06]), and quetiapine (SMD=−12.32, 95% CI [−19.09, −5.63]) could significantly improve tic symptom score, and there were significant differences between the treatment group and the placebo control group. Quetiapine was superior to haloperidol (SMD=−9.13, 95% CI [−15.06, −3.21]), pimozide (SMD=−10.38, 95% CI [−17.64, −3.11]), risperidone (SMD=−8.87, 95% CI [−15.15, −2.56]), tiapride (SMD=−11.86, 95% CI [−18.65, −5.02]), aripiprazole (SMD=−7.59, 95% CI [−14.07, −1.00]), and penfluridol (SMD=−28.24, 95% CI [−40.17, −28.26]) for improving tic symptom score, and the difference was statistically significant. Compared with tiapride, aripiprazole could significantly improve tic symptom score (SMD=−4.27, 95% CI [−8.01, −0.58]). There were no significant differences between other drugs.

In regard to the secondary efficacy outcomes for response rates, we included 33 RCTs involving 1791 participants for network meta-analysis. There were 9 comparisons of the secondary efficacy in the network plot of different types of antipsychotic agents ([Fig. 3]). The pooled effect estimates for primary efficacy from the network meta-analysis are provided ([Fig. 4]). The results were consistent with those of the primary outcome for efficacy, except that there were no significant difference comparing quetiapine with pimozide, ziprasidone, risperidone, tiapride, and aripiprazole.

In regard to the primary outcome, the results in closed loop showed that the direct estimate of the summary effect was consistent with the indirect estimate in all loops except 1 (i. e., haloperidol-tiapridal-aripiprazole), since all their 95% CIs included 0 (Fig. S1).
In regard to the secondary efficacy outcomes for response rates, their 95% CIs included 1 in all closed loop, so the direct estimate of the summary effect was consistent with the indirect estimate (Fig. S2).
Table S1 presents the results of the overall SUCRA-based probabilities for all antipsychotic drugs in terms of efficacy and response rate. The few significant findings in the network meta-analysis restrict the interpretation of hierarchical evidence based on SUCRA (Figs. S3 and S4).
Adverse events
Ninety-five percent (57/60) of the studies reported AEs. Of them, 42 studies reported specific AEs. The AEs of ziprasidone and penfluridol were not reported in included RCTs. For other antipsychotic drugs, the most common AEs of haloperidol were drowsiness, extrapyramidal reactions, and dry mouth. The most common AEs of tiapride were dizziness, nausea, and dry mouth. The most common AEs of aripiprazole were drowsiness and nausea/vomiting. The most common AEs of risperidone were drowsiness and increased appetite. The most common AEs of pimozide were acinesia and akathisia. The most common AEs of quetiapine was drowsiness. The most common AEs of olanzapine was dizziness, drowsiness, and dry mouth. The most common AEs of pailperidone were headache and nausea. The common AEs of different drugs are shown in Table S4.
Sensitivity analysis (Figs. S5 and S6) and meta-regression
In regard to the primary outcome, after excluding trials with mall sample sizes (n<20 patients), no material change of the pooled estimated effects in sensitivity analysis was found. The minor changes of estimated effects between interventions were mainly as follows: haloperidol versus placebo, olanzapine versus placebo, risperidone versus placebo, and quetiapine versus aripiprazole.
After omitting trials with long-term treatment period (treatment period>24 weeks), only 1 changed estimated effects was found. The minor changes were as follows: ziprasidone versus pimozide. In regard to the response rate, after excluding trials with mall sample sizes (n<20 patients), no material change of the pooled estimated effects in sensitivity analysis was found. The minor changes were mainly as follows: aripiprazole versus haloperidol and aripiprazole versus pimozide. Because there was no study focused on more than 24 weeks in the evaluation of response rate, we could not conduct a sensitivity analysis after omitting trials with a long-term treatment period.
In the meta-regression analysis to assess potential biases in publication year, there was no statistical significance for this variable.
Publication bias
In regard to the primary outcome, according to the funnel plot asymmetry (Fig. S7) and Egger’s test (t=1.66, p=0.132), we found there is no publication bias for risperidone and haloperidol in improving tic symptom scores outcomes. However in regard to the response rate, according to the funnel plot asymmetry (Fig. S8) and Egger’s test (t=−3.34, p=0.007), publication bias may exist.
Discussion
Statement of main findings
This systematic review and network meta-analysis identified 60 RCTs, providing a comprehensive picture of the efficacy and safety of 11 different types of antipsychotic agents for TDs. In terms of tic symptom score, the existing evidence indicated that haloperidol, risperidone, aripiprazole, quetiapine, olanzapine, and ziprasidone were significantly more effective than placebo in the improvement of tic symptom. Quetiapine was superior to haloperidol, pimozide, risperidone, tiapride, aripiprazole, and penfluridol for improving tic symptom score. Although current evidence showed quetiapine was effective, the number of included RCTs that evaluated the efficacy of quetiapine was very limited, and it has never been studied in a placebo controlled trial. Seventy percent of included RCTs reported specific AEs. Overall, tolerability of atypical antipsychotic drug was better than the typical antipsychotics. Because of the limitations of the number of included studies, the results of the overall SUCRA-based probabilities still need to be treated with caution.
In order to compare the consistency between direct and indirect comparisons for antipsychotic drugs in the treatment of TDs, we estimated the inconsistency factors in closed loop, and the results showed good consistence, except the direct estimate in 1 closed loop (i. e., haloperidol-tiapride-aripiprazole) was not consistent with the indirect estimate, the reasons may be as follows. (1) Tiapride was not approved and seldom used in the United States and the included RCTs of tiapride were all published in Chinese. (2) Fourteen RCTs evaluate the efficacy of tiapride; however, only 5 studies reported outcomes tic symptom score. The lack of RCTs may lead to the inconsistence. We also conducted sensitivity analysis to test the stability of the results, and no material change of the pooled estimated effects was found, but some minor changes were still existing. The potential reasons may be as follows: (1) small sample research may not be representative and low power; (2) results from long-term treatment may be different from that in short-term period treatment, so the sample size and treatment period may have influence on the results of this study.
Quality of the evidence
The main problems of included RCTs in our study are as follows. (1) Most studies were often labeled as “random” without providing details on random sequence generation. (2) The successful implementation of adequately concealed randomization sequences and blinding was not reported in majority of the included RCTs. (3) The majority of included RCTs were conducted in single center and the sample size was relatively small, with few multicenter studies. (4) RCTs focused on the evaluation of short-term efficacy and had no discussion of long-term efficacy. Therefore, the results of the study need to be treated with caution. Further studies should overcome these drawbacks.
Implications for clinical practice
Our study presented that typical antipsychotics (haloperidol, pimozide) were effective; however, these drugs have a poor tolerability profile (i. e., extrapyramidal and metabolic side effects), so they have been replaced stepwise by atypical antipsychotics [86]. The most thoroughly studied atypical antipsychotic to date are risperidone and aripiprazole, which appear to be the most robust evidence-based options for the treatment of TDs, while quetiapine is also a promising therapy. Ziprasidone and olanzapine also could improve tic symptoms, but the evidence is lacking. Among them, ziprasidone can be used for TS patients with baseline obesity or who have other risk factors for metabolic syndrome/diabetes [87]. Olanzapine may be used for the treatment of both tics and some symptoms of psychiatric comorbidities, but the current data supporting such efficacy are very scant. Moreover, the significant weight gain and excessive sedation that are commonly reported as AEs with olanzapine may limit widespread enthusiasm for treating tics with this medication [87]. The evidence of paliperidone and sulpiride was limited with rare clinical application.
Implications for future study
-
The quality of the included RCTs is not high. It is recommended to carry out high-quality, multicenter, large-sample RCTs to compare directly different pharmacological treatment. Several promising interventions should be given priority, including quetiapine, ziprasidone, and olanzapine.
-
RCTs need to be registered in the international clinical trial registry platform to increase the transparency of clinical trials and avoid selective reporting.
-
Future RCTs should be carried out with international cooperation to evaluate the efficacy and safety of different antipsychotic agents with more accurate dose for TDs in different ethnic groups and try to identify novel targets for improved therapies by the gradual availability of large-scale TS cohorts and novel methodologies for the study of both common and rare genetic variants.
-
Future studies should pay more attention to long-term outcome measurements, especially outcomes reported by patients or their caregivers.
-
In this network meta-analysis, there is a lack of evidence of direct comparison between some antipsychotic drugs. The efficacy of 3 interventions (i. e., paliperidone, penfluridol, and sulpiride) was evaluated in only 1 RCT. Future RCTs with direct comparison are needed in the future.
Limitations of the study
First, most of the included studies were conducted in a single center with a small sample. Therefore, the efficacy of antipsychotic agents needs to be tested in other ethnicities. Second, the outcome measurements varied across different studies, which made it difficult to compare the efficacy among different studies. Third, there was a lack of long-term evaluation of outcomes in the included studies. Fourth, monitoring the quality of implications and reporting of trials was difficult because of the lack of clinical trial registration, and publication bias may exist. Fifth, we could not combine data from different dose arm. It is difficult to separate different dose arm, because every study gave the appropriate dose for patients according to the weight.
Conclusion
Atypical antipsychotics (risperidone and aripiprazole) appear to be the most robust evidence-based options for the treatment of TDs. Quetiapine may be a promising therapy. Ziprasidone and olanzapine are also effective, but the evidence is lacking. Further high-quality directly comparing different pharmacological treatment studies are justified.
Contributions
Chunsong Yang and Zilong Hao contributed equally to this study.
Chunsong Yang: designed the review, collected data, developed the search strategy, undertook searches, appraised the quality of papers, selected trials for inclusion, extracted data from papers. Data management: carried out analysis and interpretation of the data and wrote the review.
Zilong Hao: collected data, undertook searches, appraised the quality of papers; selected trials for inclusion, extracted data from papers. Data management: checked the data and wrote the review.
Ling-Li Zhang: designed the review, collected data, undertook searches, appraised the quality of papers; selected trials for inclusion, extracted data from papers. Data management: checked the data and commented on drafts for previous version.
Cai-Rong Zhu: designed the review, selected trials for inclusion, extracted data from papers. Data management: checked the data and commented on drafts for previous version.
Ping Zhu: collected data, undertook searches, appraised the quality of papers; selected trials for inclusion, extracted data from papers.
Qin Guo: collected data, undertook searches, appraised the quality of papers; selected trials for inclusion, extracted data from papers.
Funding
This study was funded by the Natural Science Foundation of China, an evidence-based establishment of evaluation index system for pediatric rational drug use in China (No. 81373381), and the Program for Yangtze River Scholars and Innovative Research Team in University (No. IRT0935). The sponsor had no role in the study design, writing of the manuscript, or decision to submit this or future manuscripts for publication.
Conflict of Interest
No author declares any conflict of interest.
Acknowledgments
We thank the Group of People with Highest Risk of Drug Exposure of International Network for the Rational Use of Drugs, China, for providing support to coordinate circulation of the manuscript to all co-authors and collect comments from all co-authors.
* Chunsong Yang and Zilong Hao contributed equally to this study.
Supplementary Material
- Supporting Information for this article is available online at http:// doi.org/10.1055/s-0043-124872
- Supplementary Material (PDF)
-
References
- 1 Plessen KJ. Tic disorders and Tourette’s syndrome. Eur Child Adolesc Psychiatry 2013; 22 (Suppl. 01) S55-S60
- 2 Cavanna AE, Termine C. Tourette syndrome. Adv Exp Med Biol. 2012; 724: 375-383
- 3 Jimenez-Shahed J. Tourette syndrome. Neurol Clin. 2009; 27: 737-755
- 4 Conelea CA, Woods DW, Zinner SH. et al. The impact of Tourette syndrome in adults: Results from the Tourette syndrome impact survey. Community Ment Health J. 2013; 49: 110-120
- 5 Jalenques I, Galland F, Malet L. et al. Quality of life in adults with Gilles de la Tourette syndrome. BMC Psychiatry 2012; 12: 109
- 6 Roessner V, Plessen KJ, Rothenberger A. et al. European clinical guidelines for Tourette syndrome and other tic disorders. Part II: pharmacological treatment. Eur Child Adolesc Psychiatry 2011; 20: 173-196
- 7 Evans J, Seri S, Cavanna AE. The effects of Gilles de la Tourette syndrome and other chronic tic disorders on quality of life across the lifespan: a systematic review. Eur Child Adolesc Psychiatry 2016; 25: 939-948
- 8 Knight T, Steeves T, Day L. et al. Prevalence of tic disorders: A systematic review and meta-analysis. Pediatr Neurol. 2012; 47: 77-90
- 9 Murphy TK, Lewin AB, Storch EA. et al. Practice parameter for the assessment and treatment of children and adolescents with tic disorders. J Am Acad Child Adolesc. Psychiatry. 2013; 52: 1341-1359
- 10 Pringsheim T, Doja A, Gorman D. et al. Canadian guidelines for the evidence-based treatment of tic disorders: Pharmacotherapy. Can J Psychiatry. 2012; 57: 133-143
- 11 Gilbert DL, Batterson JR, Sethuraman G. et al. Tic reduction with risperidone versus pimozide in a randomized, double-blind, crossover trial. J Am Acad Child Adolesc Psychiatry. 2004; 43: 206-214
- 12 Yoo HK, Joung YS, Lee JS. et al. A multicenter, randomized, double-blind, placebo-controlled study of aripiprazole in children and adolescents with Tourette's disorder. J Clin Psychiatry. 2013; 74: e772-e780
- 13 Ghanizadeh A, Haghighi A. Aripiprazole versus risperidone for treating children and adolescents with tic disorder: A randomized double blind clinical trial. Child Psychiatry Hum Dev. 2014; 45: 596-603
- 14 Bruggeman R, van der Linden C, Buitelaar JK. et al. Risperidone versus pimozide in Tourette’s disorder: A comparative double-blind parallel-group study. J Clin Psychiatry. 2001; 62: 50-56
- 15 Yang C, Hao Z, Zhu C. et al. Interventions for tic disorders: An overview of systematic reviews and meta analyses. Neurosci Biobehav Rev. 2016; 63: 239-255
- 16 Li T, Puhan MA, Vedula SS. et al. Network meta-analysis highly attractive but more methodological research is needed. BMC Med 2011; 9: 79
- 17 Paschou P. The genetic basis of Gilles de la Tourette Syndrome. Neurosci Biobehav Rev. 2013; 37: 1026-1039
- 18 Yan WW. A review of diagnostic and statistical manual of mental disorder-III. Foreign Med Sci 1981; 2: 5-9
- 19 Pringsheim T, Marras C. Pimozide for tics in Tourette’s syndrome. Cochrane Database Syst Rev. 2009; 15: 1-15
- 20 Leckman JF, Towbin KE, Ort SI. Clinical assessment of tic disorder severity. In: Cohen DJ. ed. Tourette’s Syndrome and Tic Disorders. New York: John Wiley & Sons; 1988: 55-78
- 21 World Health Organization. The ICD-10 Classification of Mental and Behavioral Disorders Diagnostic Criteria for Research. Geneva: WHO; 1993
- 22 The Branch of Psychiatry of Chinese Medical Association. Chinese Classification and Diagnostic Criteria of Mental Disorders-3 (CCMD-3). Shandong: Science and Technology Press of Shandong Province; 2001
- 23 Leckman JF, Riddle MA, Hardin MT. et al. The Yale Global Tic Severity Scale: initial testing of a clinician-rated scale of tic severity. J Am Acad Child Adolesc Psychiatry. 1989; 28: 566-573
- 24 Leckman JF, Towbin KE, Ort SI. Clinical assessment of tic disorder severity. In: Cohen DJ. ed. Tourette’s Syndrome and Tic Disorders. New York: John Wiley & Sons; 1988: 55-78
- 25 Higgins JPT, Green S.eds. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration; 2011; Available at www.cochrane-handbook.org
- 26 Egger M. Davey Smith G. et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315: 629-634
- 27 Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med. 2004; 23: 3105-3124
- 28 Brooks SP, Gelman A. Alternative methods for monitoring convergence of iterative simulations. J Comput Graph Stat 1998; 7: 434-445
- 29 Bucher HC, Guyatt GH, Griffith LE. et al. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol 1997; 50: 683-691
- 30 Shapiro E, Shapiro AK, Fulop G. et al. Controlled study of haloperidol, pimozide and placebo for the treatment of Gilles de la Tourette’s syndrome. Arch Gen Psychiatry 1989; 46: 722-730
- 31 Sallee FR, Dougherty D, Sethuraman G. et al. Prolactin monitoring of haloperidol and pimozide treatment in children with Tourette’s syndrome. Biol Psychiatry 1996; 40: 1044-1050
- 32 Sallee FR, Nesbitt L, Jackson C. et al Relative efficacy of haloperidol and pimozide in children and adolescents with Tourette's disorder. Am J Psychiatry. 1997; 154: 1057-1062
- 33 Ross MS, Moldofsky H. A comparison of pimozide and haloperidol in the treatment of Gilles de la Tourette's syndrome. Am J Psychiatry. 1978; 135: 585-587
- 34 Shapiro AK, Shapiro E. Controlled study of pimozide vs. placebo in Tourette’s syndrome. J Am Acad Child Psychiatry 1984; 23: 161-173
- 35 Onofrj M, Paci C, D’Andreamatteo G. et al. Olanzapine in severe Gilles de la Tourette syndrome: A 52-week double-blind cross-over study vs. low-dose pimozide. J Neurol 2000; 247: 443-436
- 36 Sallee FR, Kurlan R, Goetz CG. et al Ziprasidone treatment of children and adolescents with Tourette's syndrome: a pilot study. J Am Acad Child Adolesc Psychiatry. 2000; 39: 292-299
- 37 Scahill L, Leckman JF, Schultz RT. et al. A placebo-controlled trial of risperidone in Tourette syndrome. Neurology 2003; 60: 1130-1135
- 38 Dion Y, Annable L, Sandor P. et al. Risperidone in the treatment of Tourette syndrome: A double-blind, placebo-controlled trial. J Clin Psychopharmacol. 2002; 22: 31-39
- 39 Duan BW, Li MZ. The efficacy of haloperidol and tiapride for the treatment of Tourette syndrome. Chinese Community Doctors 2008; 13: 25
- 40 Lu ZX, Shi L, Li ZJ. A control study of paliperidone versus haloperidol in the treatment of tic disorders in children. China & Foreign Medical Treatment 2015; 10: 7-9
- 41 Zhang Y. Penfluridol (hidden treatment drug) vs. haloperidol for Tourette syndrome. China Pharmacy 2007; 18: 1803-1804
- 42 Huang WJ. A control study of olanzapine and haloperidol in the treatment for tic disorders in children. Medical Journal of Chinese People’s Health 2012; 24: 2863-2893
- 43 Ji WD, Li Y, Li N. et al. Olanzapine for treatment of Tourette syndrome: a double-blind randomized controlled trial. Chinese Journal of Clinical Rehabilitation 2005; 9: 66-68
- 44 Xiong H, Xu J, Peng Z. et al. A control study of ziprasidone and haloperidol in the treatment for Tourette syndrome. Journal of Clinical and Experimental Medicine 2010; 9: 1267-1274
- 45 Wang HL, Gao CH, Yang WB. et al. A control study of risperidone and haloperidol in the treatment for Tourette syndrome. Chinese Journal of Modern Drug Application 2009; 3: 106-107
- 46 Zhang Y, Xu P, Yang Y. A comparative study of risperidone oral solution and haloperidol in the treatment of Tourette’s syndrome. Journal of Psychiatry 2010; 23: 171-173
- 47 Zhang H, Huang HZ, Lin GD. A randomized controlled study of risperidone and aripiprazole in treatment of children with tic disorder. Clinical Focus 2015; 12: 1393-1396
- 48 Zheng SQ, Li RJ, Ding YF. Clinical control study of risperidone and haloperidol in the treatment for Tourette syndrome. Nervous Diseases and Mental Health 2006; 6: 279-281
- 49 Wu ZM, Ren CB. Clinical Observation of risperidone and haloperidol in the treatment of Tourette Syndrome in children. Journal of Psychiatry 2008; 21: 452-453
- 50 Lv CB. Clinical Research of the efficacy of risperidone and haloperidol in the treatment of Tourette Syndrome. Chinese Community Doctors 2011; 13: 37-38
- 51 Zhu QX. The comparison of the effect of risperidone and tiapride in the treatment of children with Tourette’s Syndrome. Jilin Medical Journal 2012; 33: 6502-6503
- 52 Tan QE, Wu BR, Wang HH. et al. A control study of risperidone in the treatment for Tourette syndrome. J Clin Psychol Med 2004; 14: 42-43
- 53 Yao HX, Bao HH, Ou YH. et al. Controlled study of risperidone in treatment of Tourette syndrome. J Clin Psychol Med 2005; 15: 42-43
- 54 Cui YH, Zheng Y. A control observation of refractory Tourette syndrome treated with risperidone. J Clin Psychol Med 2007; 17: 371-373
- 55 Li N, Lei XF, Du JJ. Effect of risperidone for Tourette Syndrome in children. Journal of Applied Clinical Pediatrics 2010; 25: 1604-1605
- 56 Yan Q, Ma PL. Analysis of the clinical data in treatment of Tourette syndrome with risperidone. J Clin Psychosom Dis 2015; 21: 136-137
- 57 Li YD, Luo YN, Wu HS. et al. A comparison of treatment of tic disorder with risperidone and haloperidol. Chin J Rehabil Theory Practice 2006; 12: 844-845
- 58 Huang HZ, Lin JS, Li YH. et al. Clinical study of risperidone and haloperidol in treating Tourette Syndrome. Hebei Medicine Journal 2006; 12: 547-549
- 59 Xu GH. A comparison of treatment of tic disorder with risperidone. Strait Pharmaceutical Journal 2005; 17: 154-154
- 60 Guo JH, Guo SQ. Risperidone oral solution vs. haloperidol in the treatment of childhood tic disorder. Evaluation and Analysis of Drug-Use in Hospitals of China 2011; 11: 459-460
- 61 Zhou KY, Wen FQ, Chen T. et al. A comparative study on risperidone and haloperidol in the treatment of Tourette syndrome. Chinese Journal of Practical Pediatrics 2004; 19: 488-490
- 62 Zhang SC. Clinical research of the effect of risperidone in the treatment for Tourette syndrome with 39 cases. Modern Medicine & Health 2010; 26: 2932-2933
- 63 Yang ZJ. The therapeutic efficacy and safety of tiapride and haloperidol in treatment of Tourette syndrome. Journal of Clinical Pediatrics 2012; 30: 1051-1053
- 64 Zheng QF, Zhao DY, Zhang GY. et al. The observation of the effect of tiapride in the treatment of children with Tourette’s syndrome. Hebei Medical Journal 2012; 34: 2666
- 65 Diao LW. The efficacy of tiapride and haloperidol in the treatment of Tourette syndrome. Applied Journal of General Practice 2008; 6: 196
- 66 Li FM. The therapeutic efficacy and safety of tiapride in treatment of Tourette syndrome. Jilin Medical Journal 2013; 34: 465
- 67 Wang Y, Chen GH. Clinical observation of the treatment of Tourette Syndrome with tiapride and haloperidol. Chinese Journal of Practical Nervous Diseases 2013; 16: 83-84
- 68 Li HM. Comparison of clinical efficacy and safety between tiapride and haloperidol in treatment of Tourette syndrome. Drugs & Clinic 2013; 28: 919-921
- 69 Zhao ZL, Guo P, Guo H. A comparative study of aripiprazole and haloperidol for the treatment of tic disorders in children. World Health Digest 2011; 8: 111-113
- 70 Liu YY, Chen YH, Chen H. et al. A control study of aripiprazole and tiapride treatment for tic disorders in children. Chinese Journal of Contemporary Pediatrics 2010; 12: 421-424
- 71 Xu XX. The efficacy of aripiprazole in treatment of Tourette syndrome. World Latest Medicine Information 2015; 15: 77-78
- 72 Zhang Y, Su J, Hu ZJ. et al. Comparison of clinical efficacy and safety between aripiprazole and tiapride in treatment of Tourette syndrome. Shandong Medical Journal 2014; 54: 44-46
- 73 Chen ZM, Lei QH. Comparative study of aripiprazole and haloperidol in the treatment of tic disorder. Medical Journal of Chinese People’s Health 2012; 24: 402-453
- 74 Ren ZB, Jin WD, Wang HQ. A comparative study of aripiprazole and haloperidol treatment for tic disorders in children. Chinese Journal of Nervous and Mental Diseases 2012; 38: 222-224
- 75 Guo F, Qin X, Guo SQ. et al. Aripiprazole and haloperidol in the treatment of tic disorder of childhood. China Journal of Health Psychology 2013; 21: 1767-1768
- 76 Wang YH, Chen ZM, Wang XS. A comparative study of the effect of aripiprazole and tiapride treatment for tic disorders in children. Shandong Medical Journal 2013; 53: 58-59
- 77 Gao R, Zhou YD, Huang ZY. et al. A comparative study of aripiprazole and haloperidol treatment for tic disorders in children. Sichuan Mental Health 2013; 26: 300-302
- 78 Zheng QM, Li YD, Deng LH. et al. A comparative study of aripiprazole orally disintegrating tablets and Haloperidol treatment for tic disorders. Jilin Medical Journal 2015; 36: 2995-2997
- 79 Sun Y, Wang HP, Duan LF. The clinical efficacy and safety of aripiprazole in the treatment of tic disorder. China Medicine and Pharmacy 2014; 4: 64-65+113
- 80 Zhou W, Zhang YM, Zhou CX. A control analysis of aripiprazole and haloperidol treatment for tic disorders in children. Medical Information 2015; 28: 230-231
- 81 Liang YZ, Zheng Y, Zhang SJ. et al. A control study of quetiapine treatment for Tourette syndrome in children. Journal of Clinical Psychiatry 2006; 16: 292
- 82 Zhang Y, Li XY, Wang Y. A comparative study of quetiapine in the treatment of tic disorder in children. Journal of Psychiatry 2008; 21: 21-23
- 83 Sui GH. A comparative study of quetiapine and haloperidol in the treatment of tic disorder in children. Jilin Medical Journal 2015; 36: 707-708
- 84 Yanlin Yang. A control study of quetiapine and haloperidol in the treatment of tic disorder in children. Journal of Clinical Psychosomatic Diseases 2011; 17: 494-496
- 85 Zhang G. Clinical analysis of sulpiride treatment for Tourette syndrome in children. For all Health 2013; 7: 146-147
- 86 Cavanna AE, Seri S. Tourette’s syndrome. BMJ 2013; 20: 1-6
- 87 Budman CL. The role of atypical antipsychotics for treatment of Tourette's syndrome: An overview. Drugs 2014; 74: 1177-1193
Correspondence
-
References
- 1 Plessen KJ. Tic disorders and Tourette’s syndrome. Eur Child Adolesc Psychiatry 2013; 22 (Suppl. 01) S55-S60
- 2 Cavanna AE, Termine C. Tourette syndrome. Adv Exp Med Biol. 2012; 724: 375-383
- 3 Jimenez-Shahed J. Tourette syndrome. Neurol Clin. 2009; 27: 737-755
- 4 Conelea CA, Woods DW, Zinner SH. et al. The impact of Tourette syndrome in adults: Results from the Tourette syndrome impact survey. Community Ment Health J. 2013; 49: 110-120
- 5 Jalenques I, Galland F, Malet L. et al. Quality of life in adults with Gilles de la Tourette syndrome. BMC Psychiatry 2012; 12: 109
- 6 Roessner V, Plessen KJ, Rothenberger A. et al. European clinical guidelines for Tourette syndrome and other tic disorders. Part II: pharmacological treatment. Eur Child Adolesc Psychiatry 2011; 20: 173-196
- 7 Evans J, Seri S, Cavanna AE. The effects of Gilles de la Tourette syndrome and other chronic tic disorders on quality of life across the lifespan: a systematic review. Eur Child Adolesc Psychiatry 2016; 25: 939-948
- 8 Knight T, Steeves T, Day L. et al. Prevalence of tic disorders: A systematic review and meta-analysis. Pediatr Neurol. 2012; 47: 77-90
- 9 Murphy TK, Lewin AB, Storch EA. et al. Practice parameter for the assessment and treatment of children and adolescents with tic disorders. J Am Acad Child Adolesc. Psychiatry. 2013; 52: 1341-1359
- 10 Pringsheim T, Doja A, Gorman D. et al. Canadian guidelines for the evidence-based treatment of tic disorders: Pharmacotherapy. Can J Psychiatry. 2012; 57: 133-143
- 11 Gilbert DL, Batterson JR, Sethuraman G. et al. Tic reduction with risperidone versus pimozide in a randomized, double-blind, crossover trial. J Am Acad Child Adolesc Psychiatry. 2004; 43: 206-214
- 12 Yoo HK, Joung YS, Lee JS. et al. A multicenter, randomized, double-blind, placebo-controlled study of aripiprazole in children and adolescents with Tourette's disorder. J Clin Psychiatry. 2013; 74: e772-e780
- 13 Ghanizadeh A, Haghighi A. Aripiprazole versus risperidone for treating children and adolescents with tic disorder: A randomized double blind clinical trial. Child Psychiatry Hum Dev. 2014; 45: 596-603
- 14 Bruggeman R, van der Linden C, Buitelaar JK. et al. Risperidone versus pimozide in Tourette’s disorder: A comparative double-blind parallel-group study. J Clin Psychiatry. 2001; 62: 50-56
- 15 Yang C, Hao Z, Zhu C. et al. Interventions for tic disorders: An overview of systematic reviews and meta analyses. Neurosci Biobehav Rev. 2016; 63: 239-255
- 16 Li T, Puhan MA, Vedula SS. et al. Network meta-analysis highly attractive but more methodological research is needed. BMC Med 2011; 9: 79
- 17 Paschou P. The genetic basis of Gilles de la Tourette Syndrome. Neurosci Biobehav Rev. 2013; 37: 1026-1039
- 18 Yan WW. A review of diagnostic and statistical manual of mental disorder-III. Foreign Med Sci 1981; 2: 5-9
- 19 Pringsheim T, Marras C. Pimozide for tics in Tourette’s syndrome. Cochrane Database Syst Rev. 2009; 15: 1-15
- 20 Leckman JF, Towbin KE, Ort SI. Clinical assessment of tic disorder severity. In: Cohen DJ. ed. Tourette’s Syndrome and Tic Disorders. New York: John Wiley & Sons; 1988: 55-78
- 21 World Health Organization. The ICD-10 Classification of Mental and Behavioral Disorders Diagnostic Criteria for Research. Geneva: WHO; 1993
- 22 The Branch of Psychiatry of Chinese Medical Association. Chinese Classification and Diagnostic Criteria of Mental Disorders-3 (CCMD-3). Shandong: Science and Technology Press of Shandong Province; 2001
- 23 Leckman JF, Riddle MA, Hardin MT. et al. The Yale Global Tic Severity Scale: initial testing of a clinician-rated scale of tic severity. J Am Acad Child Adolesc Psychiatry. 1989; 28: 566-573
- 24 Leckman JF, Towbin KE, Ort SI. Clinical assessment of tic disorder severity. In: Cohen DJ. ed. Tourette’s Syndrome and Tic Disorders. New York: John Wiley & Sons; 1988: 55-78
- 25 Higgins JPT, Green S.eds. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration; 2011; Available at www.cochrane-handbook.org
- 26 Egger M. Davey Smith G. et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315: 629-634
- 27 Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med. 2004; 23: 3105-3124
- 28 Brooks SP, Gelman A. Alternative methods for monitoring convergence of iterative simulations. J Comput Graph Stat 1998; 7: 434-445
- 29 Bucher HC, Guyatt GH, Griffith LE. et al. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol 1997; 50: 683-691
- 30 Shapiro E, Shapiro AK, Fulop G. et al. Controlled study of haloperidol, pimozide and placebo for the treatment of Gilles de la Tourette’s syndrome. Arch Gen Psychiatry 1989; 46: 722-730
- 31 Sallee FR, Dougherty D, Sethuraman G. et al. Prolactin monitoring of haloperidol and pimozide treatment in children with Tourette’s syndrome. Biol Psychiatry 1996; 40: 1044-1050
- 32 Sallee FR, Nesbitt L, Jackson C. et al Relative efficacy of haloperidol and pimozide in children and adolescents with Tourette's disorder. Am J Psychiatry. 1997; 154: 1057-1062
- 33 Ross MS, Moldofsky H. A comparison of pimozide and haloperidol in the treatment of Gilles de la Tourette's syndrome. Am J Psychiatry. 1978; 135: 585-587
- 34 Shapiro AK, Shapiro E. Controlled study of pimozide vs. placebo in Tourette’s syndrome. J Am Acad Child Psychiatry 1984; 23: 161-173
- 35 Onofrj M, Paci C, D’Andreamatteo G. et al. Olanzapine in severe Gilles de la Tourette syndrome: A 52-week double-blind cross-over study vs. low-dose pimozide. J Neurol 2000; 247: 443-436
- 36 Sallee FR, Kurlan R, Goetz CG. et al Ziprasidone treatment of children and adolescents with Tourette's syndrome: a pilot study. J Am Acad Child Adolesc Psychiatry. 2000; 39: 292-299
- 37 Scahill L, Leckman JF, Schultz RT. et al. A placebo-controlled trial of risperidone in Tourette syndrome. Neurology 2003; 60: 1130-1135
- 38 Dion Y, Annable L, Sandor P. et al. Risperidone in the treatment of Tourette syndrome: A double-blind, placebo-controlled trial. J Clin Psychopharmacol. 2002; 22: 31-39
- 39 Duan BW, Li MZ. The efficacy of haloperidol and tiapride for the treatment of Tourette syndrome. Chinese Community Doctors 2008; 13: 25
- 40 Lu ZX, Shi L, Li ZJ. A control study of paliperidone versus haloperidol in the treatment of tic disorders in children. China & Foreign Medical Treatment 2015; 10: 7-9
- 41 Zhang Y. Penfluridol (hidden treatment drug) vs. haloperidol for Tourette syndrome. China Pharmacy 2007; 18: 1803-1804
- 42 Huang WJ. A control study of olanzapine and haloperidol in the treatment for tic disorders in children. Medical Journal of Chinese People’s Health 2012; 24: 2863-2893
- 43 Ji WD, Li Y, Li N. et al. Olanzapine for treatment of Tourette syndrome: a double-blind randomized controlled trial. Chinese Journal of Clinical Rehabilitation 2005; 9: 66-68
- 44 Xiong H, Xu J, Peng Z. et al. A control study of ziprasidone and haloperidol in the treatment for Tourette syndrome. Journal of Clinical and Experimental Medicine 2010; 9: 1267-1274
- 45 Wang HL, Gao CH, Yang WB. et al. A control study of risperidone and haloperidol in the treatment for Tourette syndrome. Chinese Journal of Modern Drug Application 2009; 3: 106-107
- 46 Zhang Y, Xu P, Yang Y. A comparative study of risperidone oral solution and haloperidol in the treatment of Tourette’s syndrome. Journal of Psychiatry 2010; 23: 171-173
- 47 Zhang H, Huang HZ, Lin GD. A randomized controlled study of risperidone and aripiprazole in treatment of children with tic disorder. Clinical Focus 2015; 12: 1393-1396
- 48 Zheng SQ, Li RJ, Ding YF. Clinical control study of risperidone and haloperidol in the treatment for Tourette syndrome. Nervous Diseases and Mental Health 2006; 6: 279-281
- 49 Wu ZM, Ren CB. Clinical Observation of risperidone and haloperidol in the treatment of Tourette Syndrome in children. Journal of Psychiatry 2008; 21: 452-453
- 50 Lv CB. Clinical Research of the efficacy of risperidone and haloperidol in the treatment of Tourette Syndrome. Chinese Community Doctors 2011; 13: 37-38
- 51 Zhu QX. The comparison of the effect of risperidone and tiapride in the treatment of children with Tourette’s Syndrome. Jilin Medical Journal 2012; 33: 6502-6503
- 52 Tan QE, Wu BR, Wang HH. et al. A control study of risperidone in the treatment for Tourette syndrome. J Clin Psychol Med 2004; 14: 42-43
- 53 Yao HX, Bao HH, Ou YH. et al. Controlled study of risperidone in treatment of Tourette syndrome. J Clin Psychol Med 2005; 15: 42-43
- 54 Cui YH, Zheng Y. A control observation of refractory Tourette syndrome treated with risperidone. J Clin Psychol Med 2007; 17: 371-373
- 55 Li N, Lei XF, Du JJ. Effect of risperidone for Tourette Syndrome in children. Journal of Applied Clinical Pediatrics 2010; 25: 1604-1605
- 56 Yan Q, Ma PL. Analysis of the clinical data in treatment of Tourette syndrome with risperidone. J Clin Psychosom Dis 2015; 21: 136-137
- 57 Li YD, Luo YN, Wu HS. et al. A comparison of treatment of tic disorder with risperidone and haloperidol. Chin J Rehabil Theory Practice 2006; 12: 844-845
- 58 Huang HZ, Lin JS, Li YH. et al. Clinical study of risperidone and haloperidol in treating Tourette Syndrome. Hebei Medicine Journal 2006; 12: 547-549
- 59 Xu GH. A comparison of treatment of tic disorder with risperidone. Strait Pharmaceutical Journal 2005; 17: 154-154
- 60 Guo JH, Guo SQ. Risperidone oral solution vs. haloperidol in the treatment of childhood tic disorder. Evaluation and Analysis of Drug-Use in Hospitals of China 2011; 11: 459-460
- 61 Zhou KY, Wen FQ, Chen T. et al. A comparative study on risperidone and haloperidol in the treatment of Tourette syndrome. Chinese Journal of Practical Pediatrics 2004; 19: 488-490
- 62 Zhang SC. Clinical research of the effect of risperidone in the treatment for Tourette syndrome with 39 cases. Modern Medicine & Health 2010; 26: 2932-2933
- 63 Yang ZJ. The therapeutic efficacy and safety of tiapride and haloperidol in treatment of Tourette syndrome. Journal of Clinical Pediatrics 2012; 30: 1051-1053
- 64 Zheng QF, Zhao DY, Zhang GY. et al. The observation of the effect of tiapride in the treatment of children with Tourette’s syndrome. Hebei Medical Journal 2012; 34: 2666
- 65 Diao LW. The efficacy of tiapride and haloperidol in the treatment of Tourette syndrome. Applied Journal of General Practice 2008; 6: 196
- 66 Li FM. The therapeutic efficacy and safety of tiapride in treatment of Tourette syndrome. Jilin Medical Journal 2013; 34: 465
- 67 Wang Y, Chen GH. Clinical observation of the treatment of Tourette Syndrome with tiapride and haloperidol. Chinese Journal of Practical Nervous Diseases 2013; 16: 83-84
- 68 Li HM. Comparison of clinical efficacy and safety between tiapride and haloperidol in treatment of Tourette syndrome. Drugs & Clinic 2013; 28: 919-921
- 69 Zhao ZL, Guo P, Guo H. A comparative study of aripiprazole and haloperidol for the treatment of tic disorders in children. World Health Digest 2011; 8: 111-113
- 70 Liu YY, Chen YH, Chen H. et al. A control study of aripiprazole and tiapride treatment for tic disorders in children. Chinese Journal of Contemporary Pediatrics 2010; 12: 421-424
- 71 Xu XX. The efficacy of aripiprazole in treatment of Tourette syndrome. World Latest Medicine Information 2015; 15: 77-78
- 72 Zhang Y, Su J, Hu ZJ. et al. Comparison of clinical efficacy and safety between aripiprazole and tiapride in treatment of Tourette syndrome. Shandong Medical Journal 2014; 54: 44-46
- 73 Chen ZM, Lei QH. Comparative study of aripiprazole and haloperidol in the treatment of tic disorder. Medical Journal of Chinese People’s Health 2012; 24: 402-453
- 74 Ren ZB, Jin WD, Wang HQ. A comparative study of aripiprazole and haloperidol treatment for tic disorders in children. Chinese Journal of Nervous and Mental Diseases 2012; 38: 222-224
- 75 Guo F, Qin X, Guo SQ. et al. Aripiprazole and haloperidol in the treatment of tic disorder of childhood. China Journal of Health Psychology 2013; 21: 1767-1768
- 76 Wang YH, Chen ZM, Wang XS. A comparative study of the effect of aripiprazole and tiapride treatment for tic disorders in children. Shandong Medical Journal 2013; 53: 58-59
- 77 Gao R, Zhou YD, Huang ZY. et al. A comparative study of aripiprazole and haloperidol treatment for tic disorders in children. Sichuan Mental Health 2013; 26: 300-302
- 78 Zheng QM, Li YD, Deng LH. et al. A comparative study of aripiprazole orally disintegrating tablets and Haloperidol treatment for tic disorders. Jilin Medical Journal 2015; 36: 2995-2997
- 79 Sun Y, Wang HP, Duan LF. The clinical efficacy and safety of aripiprazole in the treatment of tic disorder. China Medicine and Pharmacy 2014; 4: 64-65+113
- 80 Zhou W, Zhang YM, Zhou CX. A control analysis of aripiprazole and haloperidol treatment for tic disorders in children. Medical Information 2015; 28: 230-231
- 81 Liang YZ, Zheng Y, Zhang SJ. et al. A control study of quetiapine treatment for Tourette syndrome in children. Journal of Clinical Psychiatry 2006; 16: 292
- 82 Zhang Y, Li XY, Wang Y. A comparative study of quetiapine in the treatment of tic disorder in children. Journal of Psychiatry 2008; 21: 21-23
- 83 Sui GH. A comparative study of quetiapine and haloperidol in the treatment of tic disorder in children. Jilin Medical Journal 2015; 36: 707-708
- 84 Yanlin Yang. A control study of quetiapine and haloperidol in the treatment of tic disorder in children. Journal of Clinical Psychosomatic Diseases 2011; 17: 494-496
- 85 Zhang G. Clinical analysis of sulpiride treatment for Tourette syndrome in children. For all Health 2013; 7: 146-147
- 86 Cavanna AE, Seri S. Tourette’s syndrome. BMJ 2013; 20: 1-6
- 87 Budman CL. The role of atypical antipsychotics for treatment of Tourette's syndrome: An overview. Drugs 2014; 74: 1177-1193