

Subscribe to RSS
DOI: 10.1055/s-0042-1757792
Cerebrospinal Fluid Drainage for Prevention of Spinal Cord Ischemia in Thoracic Endovascular Aortic Surgery—Pros and Cons
Authors
Funding None.

Abstract
Thoracic endovascular aortic repair (TEVAR) carries a risk of spinal cord ischemia (SCI) which exerts a devastating impact on patient's quality of life and life expectancy. Although routine prophylactic cerebrospinal fluid (CSF) drainage is not unequivocally supported by current data, several studies have demonstrated favorable outcomes. Patients at high risk for SCI following TEVAR likely will benefit from prophylactic CSF drains. However, the intervention is not risk free, and thorough risk/benefit analysis should be individualized to each patient.
Introduction
Thoracic endovascular aortic repair (TEVAR) is a minimally invasive procedure increasingly used in the treatment of thoracic aortic pathologies such as aneurysm, dissection, stenosis, and traumatic injury. The procedure was first reported by Volodos et al in 1987[1] and Dake et al[2] in 1994 for the repair of descending thoracic aortic aneurysms (TAAs) in patients at high surgical risk for conventional open repair. At the time of the inception of TEVAR, the risk of paraplegia for an open repair of thoracoabdominal aortic aneurysm was 16%.[3] TEVAR has been shown to reduce the risk of morbidity and mortality compared with conventional open surgical repair.[4] Patients with complex thoracic aortic pathologies who were previously deemed nonsurgical candidates for open surgical repair due to high surgical risk are now able to receive definitive treatment with endovascular stents. Despite TEVAR's favorable outcomes and steady advances in open surgical techniques, both endovascular and open surgical repairs still carry the potential risk of spinal cord ischemia (SCI) with subsequent paraplegia, a catastrophic complication.
Spinal Cord Ischemia Effects on Life Expectancy
SCI exerts a devastating impact on patients in terms of quality of life and life expectancy. A retrospective review of 607 TEVAR patients revealed mean postoperative survival of 37.2 ± 4.5 months in patients who developed SCI, compared with 71.6 ± 3.9 months (p < 0.0006) for those who did not develop SCI. Patients with SCI who manifested functional improvement showed much-improved survival of 53.9 ± 5.9 months compared with 9.6 ± 3.6 months for those with a permanent neurological deficit (p < 0.0001).[5]
To determine the impact of SCI on functional outcome and patient survival, Conrad et al performed a retrospective analysis on 576 patients undergoing open thoracoabdominal aneurysm repair, open descending thoracic aortic repair, and TEVAR. SCI was stratified by the degree of deficit and a scale was developed and graded as follows: grade I: flaccid paralysis; grade II: <50% function; and grade III: >50% function. A significantly higher 30-day mortality was registered in patients with SCI as compared with those without SCI, 23.4 versus 8%, respectively (p < 0.001); 5-year survival of all SCI patients was less than half that of the non-SCI patients (25 ± 6 vs. 51 ± 3%, p < 0.001). Prognosis correlated closely with the degree of SCI deficit; patients with SCID grades II and III had similar 5-year survival to non-SCID patients (41 ± 10 vs. 51 ± 3%, p = 0.281). However, SCI deficit grade I conferred the worst prognosis, no patient recovered their ability to walk or lived to 5 years. Importantly, 73% of patients with SCI deficit grade II and 100% grade III patients were able to ambulate with or without assistance at their last follow-up visit.[6] Thus, the loss of the ability to walk correlated closely with mortality. It is, therefore, evident that the occurrence of SCI dramatically adversely impacts the overall quality of life and ultimately, life expectancy.
Anatomy of Spinal Cord Blood Supply
The anterior spinal artery (ASA) provides the main blood supply to the spinal cord. The ASA supplies the anterior two-thirds of the spinal cord and is formed by the vertebral arteries, which in turn originate from the subclavian arteries. Before the vertebral arteries join to form the basilar artery, they branch inferiorly forming a single ASA.[7] The posterior one-third of the spinal cord is supplied by the two posterior spinal arteries (PSAs) which originate either from the posterior inferior cerebellar artery (PICA) or from the preatlantal vertebral arteries.[8]
Through its course down the spinal cord, the ASA is augmented by an extensive collateral network. The segmental spinal arteries, intercostal and lumbar, bifurcate into an anterior and posterior radicular artery to feed both the ASAs and PSAs, respectively. The greater anterior radiculomedullary artery, also known as the artery of Adamkiewicz, is the largest segmental medullary artery that branches off the descending aorta and supplies the ASA.[8] Caudally, the hypogastric arteries provide retrograde collateral perfusion to the ASA. This extensive collateral network is crucial for preventing SCI when part of the spinal cord blood supply becomes compromised during an open or endovascular aortic repair.
Spinal Cord Ischemia Risk Thoracic Endovascular Aortic Repair versus Open
A meta-analysis of 14,580 patients compared the complications encountered with TEVAR versus open repairs for descending thoracic aortic disease and found TEVAR to be associated with a lower incidence of postoperative paraplegia (3.3 vs. 5.5%, p = 0.007).[4] However, if patients with thoracoabdominal aortic disease were included and the extent of aortic coverage was comparable, the actual risk for SCI was similar between TEVAR and open repairs. Other studies have shown that the risk of SCI with TEVAR can reach 10.3%.[9] The risk of SCI following TEVAR varies and depends primarily on the extent of coverage of the segmental arteries ([Fig. 1]) and the vigor of the paraspinal collateral network ([Fig. 2]). Several risk factors predispose TEVAR patients to SCI. These include severe calcification or extensive coverage of the descending thoracic aorta (>15 cm), coverage of the left subclavian artery without revascularization, coverage of the celiac artery, or occlusion of the hypogastric plexus.


Debate
Patients at high risk for SCI following TEVAR should receive special attention to optimize perfusion and oxygen delivery to the spinal cord. Some of the considerations for SCI monitoring and prevention include cerebrospinal fluid (CSF) drainage, blood pressure augmentation, neurophysiological monitoring, pharmacological adjuncts, and mild hypothermia. The current guidelines for patients with acute SCI recommend maintaining mean arterial pressure (MAP) above 85 to 90 mm Hg for 7 days following the injury.[10] This is based on the assumption that spinal cord perfusion pressure (SCPP) is equal to the MAP minus the CSF pressure or central vascular pressure, whichever is higher. Although this concept is extrapolated from the traumatic brain injury literature, with no direct supportive evidence, there is evidence supporting the concept that improving hemodynamics can enhance neurological outcomes.[11] [12] In addition to blood pressure augmentation, SCPP can be optimized with CSF drainage by lowering the intrathecal pressure. CSF drains (CSFDs) have been extensively used for open thoracic and thoracoabdominal aortic surgeries, and this following discussion will focus on the ongoing debate whether prophylactic CSFDs should be routinely performed in patients undergoing high-risk TEVARs. Now that the above basic perspective has been explored, the debate is entered.
Pros: For Spinal Cerebrospinal Fluid Drain
Recently, there has been increasing interest and debate regarding the prophylactic use of CSF drainage for the prevention of SCI. Although data supporting the benefit of lumbar CSFDs specifically in TEVAR are of moderate quality with no randomized controlled trials (RCTs), numerous studies have explored the utility of CSFD in open TAA repair.[13] [14] A meta-analysis including three RCTs and five cohort studies (which compared outcomes after open thoracoabdominal aortic aneurysm repair to historical cohorts) showed a significant decrease in postoperative paraplegia with the use of lumbar CSF drainage, with a pooled odds ratio of 0.3 (number needed to treat [NNT] = 9, 95% confidence interval [CI], 0.17–0.54).[15]
Several additional studies have assessed the use of CSFD in patients undergoing TEVAR and supported its role in SCI prophylaxis. A prospective observational trial performed by Hnath et al included 121 patients who underwent TEVAR. Fifty-six patients (46%) had prophylactic CSF drainage (notably this arm contained a higher proportion of patients at high risk for SCI—with more extensive aneurysmal coverage, previous abdominal aortic aneurysm repair, or coverage of the left subclavian artery), while the other 65 patients (54%) did not receive prophylactic drainage. Results showed that none of the patients with prophylactic CSFD developed SCI, while five patients (8%) in the control arm developed SCI within the first 24 hours of the procedure (p = 0.05).[14] A more recently published study, which interrogated the database of the Vascular Quality Initiative, identified 4,287 patients who underwent TEVAR for various descending aortic pathologies. In the 1,292 propensity-matched pairs of patients, prophylactic placement of CSFD reduced the risk of SCI (1.5 vs 2.5%) but did not change the number of days spent in the ICU or the 30-day mortality rates. Additionally, this study identified that placement of a CSFD as a rescue maneuver did not offer the same degree of spinal cord protection as preoperative elective placement.[16]
A 2016 meta-analysis included a total of 10 studies of both open and endovascular repairs of thoracoabdominal aortic aneurysm comparing 319 patients who received CSFD to 784 controls who did not. The study showed that CSFD decreased SCI by nearly half (relative risk of 0.42, 95% CI, 0.25–0.70; p = 0.0009), with an absolute risk reduction of 7% and the NNT to reach a benefit of 14.[13] In another study, Bobadilla et al observed 94 patients who underwent TEVAR with a mean length of aortic coverage of 16 cm. Their SCI protection protocol was routine CSF drainage (CSF pressure maintained < 10 mm Hg), endorphin receptor blockade (naloxone infusion), moderate intraoperative hypothermia (<35°C), and maintenance of MAP >90 mm Hg. Only one patient developed SCI postoperatively, who later recovered and was able to ambulate without assistance.[17]
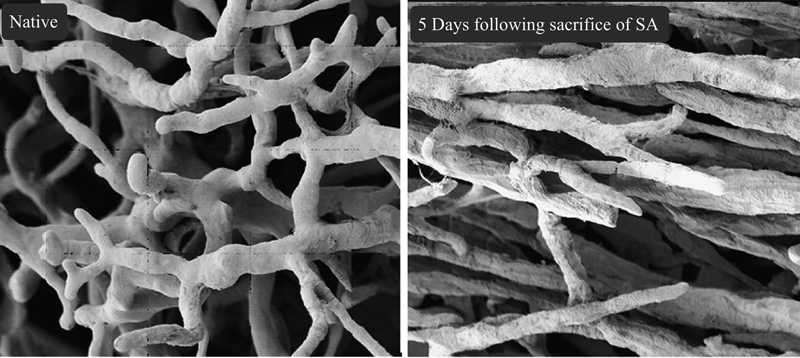
Furthermore, early experimental studies performed on animal models have demonstrated that CSF drainage reduces CSF pressure and mitigates the degree of SCI, improving neurological outcomes.[18] [19] One such experiment, performed on 10 pigs, enhanced our understanding of the impact of sacrificing segmental arteries on the SCPP intraoperatively and in the immediate postoperative period.[20] Pigs have a spinal cord collateral blood supply similar to humans.[21] [22] This experiment showed that at baseline the collateral spinal network pressure is 77% of the MAP. After clamping of segmental arteries, the collateral network pressure drops to 22 ± 6 mm Hg, reaching a nadir at 5 hours after the insult ([Fig. 3]). Another experiment done on 10 Yorkshire pigs showed that 24 hours following extensive segmental artery sacrifice, the collateral network begins to recover by a process of angiogenesis and the pressure starts to increase, reaching approximately baseline levels at 5 days after the insult ([Fig. 4]).[23] The study findings depicting an early collateral network deficiency, with subsequent recovery, suggest that early CSF drainage may be beneficial. In an endovascular procedure, the first few hours in the intensive care unit seem to be the most critical period when SCI can occur. Therefore, prophylactic CSF drainage along with blood pressure augmentation serves as a bridge until recovery of the collateral spinal network.

American College of Cardiology Foundation and the American Heart Association Guidelines
In 2010, the American College of Cardiology Foundation and the American Heart Association (ACCF/AHA) assigned a class I recommendation for the use of CSFD as a protective strategy for the spinal cord in open and endovascular thoracic aortic repair, with level B evidence.[24] A class I recommendation indicates that the procedure is strongly recommended, beneficial, and should be performed. However, as the recommendation only pertained to those patients at high risk for SCI, risk stratification of patients undergoing TEVAR can be performed before the use of prophylactic CSF drainage. Risk factors associated with the development of SCI in patients undergoing TEVAR have been well characterized in previous studies[25] [26] [27] and include extensive aortic coverage (more than nine segments) by long aortic stent-grafts or multiple stent-grafts, sacrificing a greater number of segmental and intercostal arteries, coverage of the distal thoracic aorta (Th8–Th12), previous abdominal aortic aneurysm repair,[28] coverage of the left subclavian artery compromising collateral supply from the vertebral artery,[29] incomplete circle of Willis, chronic renal insufficiency, advanced atherosclerosis,[27] emergency operation, advanced age, and perioperative hypotension. Based on a retrospective evaluation of 7,900 patients undergoing various types of TEVAR procedures, with data obtained from the Society for Vascular Surgery/Vascular Quality Improvement Database, Mousa et al developed a preoperative risk stratification scale for SCI ([Table 1]). Each risk factor is assigned several points, and patients are deemed to be at low, moderate, or high risk for SCI based on the total number of points accumulated.[30]
Abbreviations: ASA, American Society of Anesthesiologists; eGFR, estimated glomerular filtration rate.
Notes: Categories of low, medium, or high risk: low risk = raw score 0 to 4; medium risk = raw score 4.5 to 6.5; high risk = raw score ≥ 7.0. Reproduced with permission from Mousa et al.[30]
Level B evidence indicates moderate-quality evidence from one or more RCTs. Three RCTs have been published to date outlining the utility of prophylactic CSF drainage in open thoracoabdominal aortic aneurysm repair[31] [32] [33]; however, no RCTs have yet been published on the endovascular approach.
Three articles have been taken into account in the class I recommendation for the use of CSF drainage as a protective strategy for the spinal cord in TEVAR for patients at high risk for SCI. The first study included 145 patients undergoing open thoracoabdominal aortic aneurysm repair and showed that CSFDs resulted in 80% reduction in the risk of postoperative neurological injury from SCI (2.6 vs. 13%, p = 0.03).[31] Although the study showed a significant reduction in neurological injury related to SCI, it only included open thoracoabdominal aortic aneurysm repair.
A meta-analysis performed by the Cochrane group, also considered for the class I recommendation, included three RCTs on open repairs and showed a significant reduction of SCI with the use of CSFD (odds ratio [OR] = 0.48; 95% CI, 0.25–0.92). However, one of the RCTs included in the meta-analysis always utilized intrathecal papaverine in combination with CSF drainage. If this study is excluded from the meta-analysis, the benefit of lumbar CSF drainage appears to be insignificant (OR = 0.57; 95% CI, 0.28–1.17). The authors' conclusion was that data supporting the role of CSFD in thoracic and thoracoabdominal aneurysm surgery for the prevention of neurological injury are limited.[34]
The last study considered for the 2010 class I recommendation guideline was a retrospective cohort investigation analyzing 1,004 patients who underwent thoracic or thoracoabdominal open repairs over a 12-year period. Seven hundred and forty one patients (74%) had distal aortic perfusion (left atrial to femoral artery bypass) in combination with adjunctive CSFD, whereas the other 263 patients (26%) were treated in an earlier time period, with the traditional clamp-and-sew technique without either distal aortic perfusion or CSFD. The study compared these two groups and reported the SCI risk to be 2.4% in the CSFD adjunct group and 6.8% in the nonadjunct group (p < 0.0009). Furthermore, the benefit was more evident in patients at high risk for SCI (patients with aneurysm distal to the left subclavian artery to below the renal arteries), with SCI occurring in 11 out of 167 (6.6%) in the adjunct group versus 11 out of 38 (29%) in the nonadjunct group.[35] However, no endovascular repairs were included in the study and the benefit may be attributed to the combination of both techniques, distal aortic perfusion and CSF drainage.
Based on this substantial but not ideal evidence, proponents strongly support the use of prophylactic CSFD in high-risk patients undergoing both open and endovascular thoracic aortic procedures.
Cons: Against Spinal Cerebrospinal Fluid Drain
It can be argued that results from open surgery may not translate to the endovascular approach as several distinct differences exist. For example, in open surgery, the historical clamp and sew technique ([Fig. 5]) requires the use of an aortic clamp causing a higher MAP proximal to the clamp, with severe hypoperfusion distal to the aortic clamp. With the clamp and sew technique, there is no time for reimplantation of intercostal arteries, thus permanently depriving the spinal cord of collateral blood supply.

Standard left atrial-femoral bypass ([Fig. 6]) revolutionized open aortic repair by offering distal perfusion, which improves blood pressure below the clamp and allows time for segmental artery reimplantation, resulting in improved spinal cord perfusion. Similarly, in endovascular repair ([Fig. 7]), the graft body allows for continuous blood flow throughout the procedure, resulting in much better hemodynamic stability and sustained lower body perfusion. Cardiovascular stability and the absence of aortic cross-clamping in the endovascular technique likely underlie the improved SCI outcomes, despite the inherent permanent sacrifice of segmental arteries. Experimental studies on sheep have shown that cross-clamping the aorta produces a much greater risk for SCI compared with covering the thoracic aorta with stent-grafts.[36]


Moreover, also arguing against routine CSFD, some studies have shown that preoperative lumbar drainage is not associated with a reduced risk for SCI in TEVAR.[37] [38] A recent systematic review by Wong et al identified 46 studies comprising a total of 4,936 patients, aiming to determine the appropriate role of CSFD in TEVAR. The overall incidence of SCI was reported to be 3.89%, and the pooled rate of SCI for patients who received prophylactic CSFD was 3.2% compared with 3.47% in patients who did not receive prophylactic CSFD. Furthermore, in 24 included studies, prophylactic CSFD was used selectively (for patients at high risk for SCI) and the pooled rate of SCI was 5.6%. The study concluded that the role of prophylactic CSFD in TEVAR is difficult to establish.[38]
In a single-center study, which included 381 patients undergoing TEVAR over a period of 10-years, CSFD was utilized selectively based on SCI risk. Twenty-one percent (81/381) of the patients had preoperative CSFDs placed, of whom 14.8% (12/81) developed SCI; 6 of these were transient, whereas 6 resulted in permanent neurologic injury. In patients who did not receive a preoperative CSFD, SCI occurred in 4.3% (13/300) of the patients. In nine of these patients, SCI resolved with blood pressure augmentation. Three patients required late CSFD placement as SCI did not resolve with blood pressure augmentation alone, but they achieved complete resolution of symptoms. Only 1 of the 13 patients suffered permanent paraplegia. Moreover, in 32% (26/81) of the patients, preoperative CSFDs were never utilized as the CSF pressure never exceeded 12 mm Hg and none of these patients manifested signs of SCI. Drain-related complications occurred in 11% (9/81) of the patients, with no permanent injury registered. The study concluded that the utility of preoperative lumbar drains for the prevention of SCI during TEVAR procedures remains questionable.[37]
Cerebrospinal Fluid Drainage Complications and Safety Measures
As with any procedure, CSF drainage has its own complications, which vary in severity. These complications may be related to drain placement or removal, to CSF drainage per se, and to the indwelling spinal catheter. Some experts feel that prophylactic CSFD should be reserved for high-risk patients due to the significant risks associated with the procedure and that a thorough risk-benefit analysis should be performed before placing the CSFD. A recent retrospective single-center study evaluated the utility of CSFDs in preventing SCI and the frequency of drain-related complications. Consistent with previous literature, this study identified that the group that had a prophylactic CSF drainage had a lower incidence of SCI (1.2 vs. 2.9%), but the 30-day mortality was similar in both groups. However, the study also identified a 6% risk of CSFD-related complications, none of which were permanent.[39] Another very recent study that assessed the safety of perioperative CSFD placement came to similar conclusions.[40] A large meta-analysis performed to define a more accurate risk-benefit ratio analyzed 34 studies from 1990 to 2017 and included 4,714 patients who had CSFD placed for open or endovascular repairs of thoracic or thoracoabdominal aortic aneurysms. The study identified the overall CSFD-related complication rate at 6.5%, with severe complications occurring in 2.5% of the cases and a pooled CSFD-related mortality rate of 0.9%.[41] Severe complications included subarachnoid or intracranial hemorrhage (ICH), epidural hematoma, meningitis, and drainage or catheter-related neurological deficit. Therefore, the placement of a CSFD is not without risk and should be heavily weighed against the benefit.
A retrospective review performed by Wynn et al studied complications of CSFD performed in 724 patients. A total of 10% of the patients developed bloody CSF, of whom half had an ICH diagnosed on computed tomography (CT) of the brain. The general interpretation is that dropping CSF pressure in the spinal canal can lead to the caudal anatomic displacement of the brain, stretching fragile veins and leading to bloody CSF. Of those patients with ICH, six (15%) were symptomatic and three (7.5%) died. These authors further reported that a higher volume of CSF drainage correlated with the likelihood of intracerebral bleeding and, therefore, suggested that the amount of CSF drainage should be restricted to no more than 10 to 20 mL per hour along with a CSF pressure target of 8 to 10 mm Hg.[42] As identified by this study, mortality related to CSFD is highest in patients with symptomatic ICH. Patients with bloody CSF, unexplained headache, decreased level of consciousness, or a neurological deficit not related to SCI should undergo a head CT emergently to rule out ICH. The risk of ICH related to CSF drainage can be minimized by intermittently draining 10 to 20 mL per hour and maintaining an ICP between 8 and 10 mm Hg (in the absence of SCI).
Although CSF drainage carries a risk of serious complications, adherence to safety measures can significantly minimize this risk. Authorities point to methods of risk reduction, including fluoroscopy-guided CSFD placement, avoidance of over-drainage of CSF, placement of drains a day prior to surgery, and protocol-based management of CSFDs. Some studies have reported no cases of spinal or epidural hematomas.[43] [44] Less serious CSFD complications have been shown to occur at a rate of 2 to 3.7% and include puncture site bleeding, CSF leak, hypotension, spinal headache, and catheter fracture.[41] Another study performed to evaluate the safety of CSFD in 135 patients who underwent open thoracic aortic surgery using extracorporeal circulation and full anticoagulation did not result in any hemorrhagic complications, with the most frequent complication being catheter fracture at 1.8%,[43] which can be minimized with the proper surgical technique.
Thus, opponents of spinal drainage have meaningful data on which to draw, data that confirms rare but real potential complications and equivocal benefits.
Conclusion
There is tangible, credible evidence to support both sides of the debate—as is seen so often, because medicine, even at the level of complex surgical procedures, remains an art rather than true science.
Even though endovascular repair has a lower risk than open thoracoabdominal aortic aneurysm surgery, SCI with potentially permanent paraplegia remains a possible complication of TEVAR. CSF drainage allows for SCPP optimization during critical periods of hypoperfusion. According to the ACCF/AHA guidelines, CSFD is recommended for patients at high risk for SCI undergoing TEVAR procedures. Although there are no RCTs to validate the utility of preoperative CSFD specifically in TEVAR procedures, several recent studies have demonstrated favorable outcomes.[13] [14] [17] [45] [46] Nevertheless, routine prophylactic CSF drainage is not unequivocally supported by current data. In conclusion, the significant economic burden associated with morbidity and mortality of SCI, the tragic consequences of rescue drainage failure, combined with the low risks for CSF drainage complications, in our view justify the use of prophylactic CSFDs in high-risk patients undergoing open surgical repair or TEVAR.[47] However, the intervention is not risk-free, and a thorough risk/benefit analysis should be individualized to each patient.
Conflict of Interest
J.A.E. is the Principal at CoolSpine and consultant for Tissium.
Acknowledgments
None.
-
References
- 1 Volodos' NL, Karpovich IP, Shekhanin VE, Troian VI, Iakovenko LF. [A case of distant transfemoral endoprosthesis of the thoracic artery using a self-fixing synthetic prosthesis in traumatic aneurysm]. Grudn Khir 1988; (06) 84-86
- 2 Dake MD, Miller DC, Semba CP, Mitchell RS, Walker PJ, Liddell RP. Transluminal placement of endovascular stent-grafts for the treatment of descending thoracic aortic aneurysms. N Engl J Med 1994; 331 (26) 1729-1734
- 3 Svensson LG, Crawford ES, Hess KR, Coselli JS, Safi HJ. Experience with 1509 patients undergoing thoracoabdominal aortic operations. J Vasc Surg 1993; 17 (02) 357-368 , discussion 368–370
- 4 Harky A, Kai Chan JS, Ming Wong CH, Bashir M. Open versus endovascular repair of descending thoracic aortic aneurysm disease: a systematic review and meta-analysis. Ann Vasc Surg 2019; 54: 304-315.e5
- 5 DeSart K, Scali ST, Feezor RJ. et al. Fate of patients with spinal cord ischemia complicating thoracic endovascular aortic repair. J Vasc Surg 2013; 58 (03) 635-42.e2
- 6 Conrad MF, Ye JY, Chung TK, Davison JK, Cambria RP. Spinal cord complications after thoracic aortic surgery: long-term survival and functional status varies with deficit severity. J Vasc Surg 2008; 48 (01) 47-53
- 7 Ali F, Reddy V, Dublin AB. Anatomy, Back, Anterior Spinal Artery. Treasure Island, FL: StatPearls; 2021
- 8 Gofur EM, Singh P. Anatomy, Back, Vertebral Canal Blood Supply. Treasure Island, FL: StatPearls; 2021
- 9 Uchida N. How to prevent spinal cord injury during endovascular repair of thoracic aortic disease. Gen Thorac Cardiovasc Surg 2014; 62 (07) 391-397
- 10 Walters BC, Hadley MN, Hurlbert RJ. et al; American Association of Neurological Surgeons, Congress of Neurological Surgeons. Guidelines for the management of acute cervical spine and spinal cord injuries: 2013 update. Neurosurgery 2013; 60 (CN_suppl_1): 82-91
- 11 Hawryluk G, Whetstone W, Saigal R. et al. Mean arterial blood pressure correlates with neurological recovery after human spinal cord injury: analysis of high frequency physiologic data. J Neurotrauma 2015; 32 (24) 1958-1967
- 12 Menacho ST, Floyd C. Current practices and goals for mean arterial pressure and spinal cord perfusion pressure in acute traumatic spinal cord injury: defining the gaps in knowledge. J Spinal Cord Med 2021; 44 (03) 350-356
- 13 Khan NR, Smalley Z, Nesvick CL, Lee SL, Michael II LM. The use of lumbar drains in preventing spinal cord injury following thoracoabdominal aortic aneurysm repair: an updated systematic review and meta-analysis. J Neurosurg Spine 2016; 25 (03) 383-393
- 14 Hnath JC, Mehta M, Taggert JB. et al. Strategies to improve spinal cord ischemia in endovascular thoracic aortic repair: Outcomes of a prospective cerebrospinal fluid drainage protocol. J Vasc Surg 2008; 48 (04) 836-840
- 15 Cinà CS, Abouzahr L, Arena GO, Laganà A, Devereaux PJ, Farrokhyar F. Cerebrospinal fluid drainage to prevent paraplegia during thoracic and thoracoabdominal aortic aneurysm surgery: a systematic review and meta-analysis. J Vasc Surg 2004; 40 (01) 36-44
- 16 Suarez-Pierre A, Zhou X, Gonzalez JE. et al. Association of preoperative spinal drain placement with spinal cord ischemia among patients undergoing thoracic and thoracoabdominal endovascular aortic repair. J Vasc Surg 2019; 70 (02) 393-403
- 17 Bobadilla JL, Wynn M, Tefera G, Acher CW. Low incidence of paraplegia after thoracic endovascular aneurysm repair with proactive spinal cord protective protocols. J Vasc Surg 2013; 57 (06) 1537-1542
- 18 Bower TC, Murray MJ, Gloviczki P, Yaksh TL, Hollier LH, Pairolero PC. Effects of thoracic aortic occlusion and cerebrospinal fluid drainage on regional spinal cord blood flow in dogs: correlation with neurologic outcome. J Vasc Surg 1989; 9 (01) 135-144
- 19 Dasmahapatra HK, Coles JG, Wilson GJ. et al. Relationship between cerebrospinal fluid dynamics and reversible spinal cord ischemia during experimental thoracic aortic occlusion. J Thorac Cardiovasc Surg 1988; 95 (05) 920-923
- 20 Etz CD, Homann TM, Plestis KA. et al. Spinal cord perfusion after extensive segmental artery sacrifice: can paraplegia be prevented?. Eur J Cardiothorac Surg 2007; 31 (04) 643-648
- 21 Strauch JT, Lauten A, Spielvogel D. et al. Mild hypothermia protects the spinal cord from ischemic injury in a chronic porcine model. Eur J Cardiothorac Surg 2004; 25 (05) 708-715
- 22 Strauch JT, Spielvogel D, Lauten A. et al. Importance of extrasegmental vessels for spinal cord blood supply in a chronic porcine model. Eur J Cardiothorac Surg 2003; 24 (05) 817-824
- 23 Etz CD, Kari FA, Mueller CS, Brenner RM, Lin HM, Griepp RB. The collateral network concept: remodeling of the arterial collateral network after experimental segmental artery sacrifice. J Thorac Cardiovasc Surg 2011; 141 (04) 1029-1036
- 24 Hiratzka LF, Bakris GL, Beckman JA. et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, Society for Vascular Medicine. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. J Am Coll Cardiol 2010; 55 (14) e27-e129
- 25 Bisdas T, Panuccio G, Sugimoto M, Torsello G, Austermann M. Risk factors for spinal cord ischemia after endovascular repair of thoracoabdominal aortic aneurysms. J Vasc Surg 2015; 61 (06) 1408-1416
- 26 Hiraoka T, Komiya T, Tsuneyoshi H, Shimamoto T. Risk factors for spinal cord ischaemia after thoracic endovascular aortic repair. Interact Cardiovasc Thorac Surg 2018; 27 (01) 54-59
- 27 Ullery BW, Cheung AT, Fairman RM. et al. Risk factors, outcomes, and clinical manifestations of spinal cord ischemia following thoracic endovascular aortic repair. J Vasc Surg 2011; 54 (03) 677-684
- 28 Schlösser FJ, Verhagen HJ, Lin PH. et al. TEVAR following prior abdominal aortic aneurysm surgery: increased risk of neurological deficit. J Vasc Surg 2009; 49 (02) 308-314 , discussion 314
- 29 Matsumura JS, Lee WA, Mitchell RS. et al; Society for Vascular Surgery. The Society for Vascular Surgery Practice Guidelines: management of the left subclavian artery with thoracic endovascular aortic repair. J Vasc Surg 2009; 50 (05) 1155-1158
- 30 Mousa AY, Morcos R, Broce M, Bates MC, AbuRahma AF. New preoperative spinal cord ischemia risk stratification model for patients undergoing thoracic endovascular aortic repair. Vasc Endovascular Surg 2020; 54 (06) 487-496
- 31 Coselli JS, LeMaire SA, Köksoy C, Schmittling ZC, Curling PE. Cerebrospinal fluid drainage reduces paraplegia after thoracoabdominal aortic aneurysm repair: results of a randomized clinical trial. J Vasc Surg 2002; 35 (04) 631-639
- 32 Svensson LG, Hess KR, D'Agostino RS. et al. Reduction of neurologic injury after high-risk thoracoabdominal aortic operation. Ann Thorac Surg 1998; 66 (01) 132-138
- 33 Crawford ES, Svensson LG, Hess KR. et al. A prospective randomized study of cerebrospinal fluid drainage to prevent paraplegia after high-risk surgery on the thoracoabdominal aorta. J Vasc Surg 1991; 13 (01) 36-45 , discussion 45–46
- 34 Khan SN, Stansby G. Cerebrospinal fluid drainage for thoracic and thoracoabdominal aortic aneurysm surgery. Cochrane Database Syst Rev 2012; 10 (10) CD003635
- 35 Safi HJ, Miller III CC, Huynh TT. et al. Distal aortic perfusion and cerebrospinal fluid drainage for thoracoabdominal and descending thoracic aortic repair: ten years of organ protection. Ann Surg 2003; 238 (03) 372-380 , discussion 380–381
- 36 Böckler D, Kotelis D, Kohlhof P. et al. Spinal cord ischemia after endovascular repair of the descending thoracic aorta in a sheep model. Eur J Vasc Endovasc Surg 2007; 34 (04) 461-469
- 37 Hanna JM, Andersen ND, Aziz H, Shah AA, McCann RL, Hughes GC. Results with selective preoperative lumbar drain placement for thoracic endovascular aortic repair. Ann Thorac Surg 2013; 95 (06) 1968-1974 , discussion 1974–1975
- 38 Wong CS, Healy D, Canning C, Coffey JC, Boyle JR, Walsh SR. A systematic review of spinal cord injury and cerebrospinal fluid drainage after thoracic aortic endografting. J Vasc Surg 2012; 56 (05) 1438-1447
- 39 Chaudhary O, Sharkey A, Schermerhorn M. et al. Protocolized based management of cerebrospinal fluid drains in thoracic endovascular aortic aneurysm repair procedures. Ann Vasc Surg 2021; 72: 409-418
- 40 Abdelbaky M, Papanikolaou D, Zafar MA. et al. Safety of perioperative cerebrospinal fluid drain as a protective strategy during descending and thoracoabdominal open aortic repair. JTCVS Tech 2021; 6: 1-8
- 41 Rong LQ, Kamel MK, Rahouma M, White RS, Lichtman AD, Pror KO. Cerebrospinal fluid drain-related complications in patients undergoing open and endovascular repairs of thoracic and thoracoabdominal aortic pathologies: a systematic review and meta-analysis. J Vasc Surg 2018; 68 (02) 652
- 42 Wynn MM, Sebranek J, Marks E, Engelbert T, Acher CW. Complications of spinal fluid drainage in thoracic and thoracoabdominal aortic aneurysm surgery in 724 patients treated from 1987 to 2013. J Cardiothorac Vasc Anesth 2015; 29 (02) 342-350
- 43 Cheung AT, Pochettino A, Guvakov DV, Weiss SJ, Shanmugan S, Bavaria JE. Safety of lumbar drains in thoracic aortic operations performed with extracorporeal circulation. Ann Thorac Surg 2003; 76 (04) 1190-1196 , discussion 1196–1197
- 44 Youngblood SC, Tolpin DA, LeMaire SA, Coselli JS, Lee V-V, Cooper Jr JR. Complications of cerebrospinal fluid drainage after thoracic aortic surgery: a review of 504 patients over 5 years. J Thorac Cardiovasc Surg 2013; 146 (01) 166-171
- 45 Weigang E, Hartert M, Siegenthaler MP. et al. Perioperative management to improve neurologic outcome in thoracic or thoracoabdominal aortic stent-grafting. Ann Thorac Surg 2006; 82 (05) 1679-1687
- 46 Cheung AT, Pochettino A, McGarvey ML. et al. Strategies to manage paraplegia risk after endovascular stent repair of descending thoracic aortic aneurysms. Ann Thorac Surg 2005; 80 (04) 1280-1288 , discussion 1288–1289
- 47 Arora H, Ullery BW, Kumar PA, Cheung AT. Pro: patients at risk for spinal cord ischemia after thoracic endovascular aortic repairs should receive prophylactic cerebrospinal fluid drainage. J Cardiothorac Vasc Anesth 2015; 29 (05) 1376-1380
Address for correspondence
Publication History
Received: 07 September 2021
Accepted: 14 April 2022
Article published online:
20 December 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Volodos' NL, Karpovich IP, Shekhanin VE, Troian VI, Iakovenko LF. [A case of distant transfemoral endoprosthesis of the thoracic artery using a self-fixing synthetic prosthesis in traumatic aneurysm]. Grudn Khir 1988; (06) 84-86
- 2 Dake MD, Miller DC, Semba CP, Mitchell RS, Walker PJ, Liddell RP. Transluminal placement of endovascular stent-grafts for the treatment of descending thoracic aortic aneurysms. N Engl J Med 1994; 331 (26) 1729-1734
- 3 Svensson LG, Crawford ES, Hess KR, Coselli JS, Safi HJ. Experience with 1509 patients undergoing thoracoabdominal aortic operations. J Vasc Surg 1993; 17 (02) 357-368 , discussion 368–370
- 4 Harky A, Kai Chan JS, Ming Wong CH, Bashir M. Open versus endovascular repair of descending thoracic aortic aneurysm disease: a systematic review and meta-analysis. Ann Vasc Surg 2019; 54: 304-315.e5
- 5 DeSart K, Scali ST, Feezor RJ. et al. Fate of patients with spinal cord ischemia complicating thoracic endovascular aortic repair. J Vasc Surg 2013; 58 (03) 635-42.e2
- 6 Conrad MF, Ye JY, Chung TK, Davison JK, Cambria RP. Spinal cord complications after thoracic aortic surgery: long-term survival and functional status varies with deficit severity. J Vasc Surg 2008; 48 (01) 47-53
- 7 Ali F, Reddy V, Dublin AB. Anatomy, Back, Anterior Spinal Artery. Treasure Island, FL: StatPearls; 2021
- 8 Gofur EM, Singh P. Anatomy, Back, Vertebral Canal Blood Supply. Treasure Island, FL: StatPearls; 2021
- 9 Uchida N. How to prevent spinal cord injury during endovascular repair of thoracic aortic disease. Gen Thorac Cardiovasc Surg 2014; 62 (07) 391-397
- 10 Walters BC, Hadley MN, Hurlbert RJ. et al; American Association of Neurological Surgeons, Congress of Neurological Surgeons. Guidelines for the management of acute cervical spine and spinal cord injuries: 2013 update. Neurosurgery 2013; 60 (CN_suppl_1): 82-91
- 11 Hawryluk G, Whetstone W, Saigal R. et al. Mean arterial blood pressure correlates with neurological recovery after human spinal cord injury: analysis of high frequency physiologic data. J Neurotrauma 2015; 32 (24) 1958-1967
- 12 Menacho ST, Floyd C. Current practices and goals for mean arterial pressure and spinal cord perfusion pressure in acute traumatic spinal cord injury: defining the gaps in knowledge. J Spinal Cord Med 2021; 44 (03) 350-356
- 13 Khan NR, Smalley Z, Nesvick CL, Lee SL, Michael II LM. The use of lumbar drains in preventing spinal cord injury following thoracoabdominal aortic aneurysm repair: an updated systematic review and meta-analysis. J Neurosurg Spine 2016; 25 (03) 383-393
- 14 Hnath JC, Mehta M, Taggert JB. et al. Strategies to improve spinal cord ischemia in endovascular thoracic aortic repair: Outcomes of a prospective cerebrospinal fluid drainage protocol. J Vasc Surg 2008; 48 (04) 836-840
- 15 Cinà CS, Abouzahr L, Arena GO, Laganà A, Devereaux PJ, Farrokhyar F. Cerebrospinal fluid drainage to prevent paraplegia during thoracic and thoracoabdominal aortic aneurysm surgery: a systematic review and meta-analysis. J Vasc Surg 2004; 40 (01) 36-44
- 16 Suarez-Pierre A, Zhou X, Gonzalez JE. et al. Association of preoperative spinal drain placement with spinal cord ischemia among patients undergoing thoracic and thoracoabdominal endovascular aortic repair. J Vasc Surg 2019; 70 (02) 393-403
- 17 Bobadilla JL, Wynn M, Tefera G, Acher CW. Low incidence of paraplegia after thoracic endovascular aneurysm repair with proactive spinal cord protective protocols. J Vasc Surg 2013; 57 (06) 1537-1542
- 18 Bower TC, Murray MJ, Gloviczki P, Yaksh TL, Hollier LH, Pairolero PC. Effects of thoracic aortic occlusion and cerebrospinal fluid drainage on regional spinal cord blood flow in dogs: correlation with neurologic outcome. J Vasc Surg 1989; 9 (01) 135-144
- 19 Dasmahapatra HK, Coles JG, Wilson GJ. et al. Relationship between cerebrospinal fluid dynamics and reversible spinal cord ischemia during experimental thoracic aortic occlusion. J Thorac Cardiovasc Surg 1988; 95 (05) 920-923
- 20 Etz CD, Homann TM, Plestis KA. et al. Spinal cord perfusion after extensive segmental artery sacrifice: can paraplegia be prevented?. Eur J Cardiothorac Surg 2007; 31 (04) 643-648
- 21 Strauch JT, Lauten A, Spielvogel D. et al. Mild hypothermia protects the spinal cord from ischemic injury in a chronic porcine model. Eur J Cardiothorac Surg 2004; 25 (05) 708-715
- 22 Strauch JT, Spielvogel D, Lauten A. et al. Importance of extrasegmental vessels for spinal cord blood supply in a chronic porcine model. Eur J Cardiothorac Surg 2003; 24 (05) 817-824
- 23 Etz CD, Kari FA, Mueller CS, Brenner RM, Lin HM, Griepp RB. The collateral network concept: remodeling of the arterial collateral network after experimental segmental artery sacrifice. J Thorac Cardiovasc Surg 2011; 141 (04) 1029-1036
- 24 Hiratzka LF, Bakris GL, Beckman JA. et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, Society for Vascular Medicine. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. J Am Coll Cardiol 2010; 55 (14) e27-e129
- 25 Bisdas T, Panuccio G, Sugimoto M, Torsello G, Austermann M. Risk factors for spinal cord ischemia after endovascular repair of thoracoabdominal aortic aneurysms. J Vasc Surg 2015; 61 (06) 1408-1416
- 26 Hiraoka T, Komiya T, Tsuneyoshi H, Shimamoto T. Risk factors for spinal cord ischaemia after thoracic endovascular aortic repair. Interact Cardiovasc Thorac Surg 2018; 27 (01) 54-59
- 27 Ullery BW, Cheung AT, Fairman RM. et al. Risk factors, outcomes, and clinical manifestations of spinal cord ischemia following thoracic endovascular aortic repair. J Vasc Surg 2011; 54 (03) 677-684
- 28 Schlösser FJ, Verhagen HJ, Lin PH. et al. TEVAR following prior abdominal aortic aneurysm surgery: increased risk of neurological deficit. J Vasc Surg 2009; 49 (02) 308-314 , discussion 314
- 29 Matsumura JS, Lee WA, Mitchell RS. et al; Society for Vascular Surgery. The Society for Vascular Surgery Practice Guidelines: management of the left subclavian artery with thoracic endovascular aortic repair. J Vasc Surg 2009; 50 (05) 1155-1158
- 30 Mousa AY, Morcos R, Broce M, Bates MC, AbuRahma AF. New preoperative spinal cord ischemia risk stratification model for patients undergoing thoracic endovascular aortic repair. Vasc Endovascular Surg 2020; 54 (06) 487-496
- 31 Coselli JS, LeMaire SA, Köksoy C, Schmittling ZC, Curling PE. Cerebrospinal fluid drainage reduces paraplegia after thoracoabdominal aortic aneurysm repair: results of a randomized clinical trial. J Vasc Surg 2002; 35 (04) 631-639
- 32 Svensson LG, Hess KR, D'Agostino RS. et al. Reduction of neurologic injury after high-risk thoracoabdominal aortic operation. Ann Thorac Surg 1998; 66 (01) 132-138
- 33 Crawford ES, Svensson LG, Hess KR. et al. A prospective randomized study of cerebrospinal fluid drainage to prevent paraplegia after high-risk surgery on the thoracoabdominal aorta. J Vasc Surg 1991; 13 (01) 36-45 , discussion 45–46
- 34 Khan SN, Stansby G. Cerebrospinal fluid drainage for thoracic and thoracoabdominal aortic aneurysm surgery. Cochrane Database Syst Rev 2012; 10 (10) CD003635
- 35 Safi HJ, Miller III CC, Huynh TT. et al. Distal aortic perfusion and cerebrospinal fluid drainage for thoracoabdominal and descending thoracic aortic repair: ten years of organ protection. Ann Surg 2003; 238 (03) 372-380 , discussion 380–381
- 36 Böckler D, Kotelis D, Kohlhof P. et al. Spinal cord ischemia after endovascular repair of the descending thoracic aorta in a sheep model. Eur J Vasc Endovasc Surg 2007; 34 (04) 461-469
- 37 Hanna JM, Andersen ND, Aziz H, Shah AA, McCann RL, Hughes GC. Results with selective preoperative lumbar drain placement for thoracic endovascular aortic repair. Ann Thorac Surg 2013; 95 (06) 1968-1974 , discussion 1974–1975
- 38 Wong CS, Healy D, Canning C, Coffey JC, Boyle JR, Walsh SR. A systematic review of spinal cord injury and cerebrospinal fluid drainage after thoracic aortic endografting. J Vasc Surg 2012; 56 (05) 1438-1447
- 39 Chaudhary O, Sharkey A, Schermerhorn M. et al. Protocolized based management of cerebrospinal fluid drains in thoracic endovascular aortic aneurysm repair procedures. Ann Vasc Surg 2021; 72: 409-418
- 40 Abdelbaky M, Papanikolaou D, Zafar MA. et al. Safety of perioperative cerebrospinal fluid drain as a protective strategy during descending and thoracoabdominal open aortic repair. JTCVS Tech 2021; 6: 1-8
- 41 Rong LQ, Kamel MK, Rahouma M, White RS, Lichtman AD, Pror KO. Cerebrospinal fluid drain-related complications in patients undergoing open and endovascular repairs of thoracic and thoracoabdominal aortic pathologies: a systematic review and meta-analysis. J Vasc Surg 2018; 68 (02) 652
- 42 Wynn MM, Sebranek J, Marks E, Engelbert T, Acher CW. Complications of spinal fluid drainage in thoracic and thoracoabdominal aortic aneurysm surgery in 724 patients treated from 1987 to 2013. J Cardiothorac Vasc Anesth 2015; 29 (02) 342-350
- 43 Cheung AT, Pochettino A, Guvakov DV, Weiss SJ, Shanmugan S, Bavaria JE. Safety of lumbar drains in thoracic aortic operations performed with extracorporeal circulation. Ann Thorac Surg 2003; 76 (04) 1190-1196 , discussion 1196–1197
- 44 Youngblood SC, Tolpin DA, LeMaire SA, Coselli JS, Lee V-V, Cooper Jr JR. Complications of cerebrospinal fluid drainage after thoracic aortic surgery: a review of 504 patients over 5 years. J Thorac Cardiovasc Surg 2013; 146 (01) 166-171
- 45 Weigang E, Hartert M, Siegenthaler MP. et al. Perioperative management to improve neurologic outcome in thoracic or thoracoabdominal aortic stent-grafting. Ann Thorac Surg 2006; 82 (05) 1679-1687
- 46 Cheung AT, Pochettino A, McGarvey ML. et al. Strategies to manage paraplegia risk after endovascular stent repair of descending thoracic aortic aneurysms. Ann Thorac Surg 2005; 80 (04) 1280-1288 , discussion 1288–1289
- 47 Arora H, Ullery BW, Kumar PA, Cheung AT. Pro: patients at risk for spinal cord ischemia after thoracic endovascular aortic repairs should receive prophylactic cerebrospinal fluid drainage. J Cardiothorac Vasc Anesth 2015; 29 (05) 1376-1380