

Subscribe to RSS
DOI: 10.1055/s-0040-1709651
Structuring Clinical Data for Improving Departmental Functionality
Authors
Funding None.

Abstract
A practical clinical information system used in a hospital's Department of Obstetrics and Gynecology is described, demonstrating its utility to automatically provide required regulatory reports and potential clinical performance improvement, in an easy-to-use way. Its use demonstrates how physician's workflow can be left unimpeded, while centralizing scribe activity to translate textually based documentation to structured data, to improve functionality within its departmental activity. The ability to easily view clinical trends from the collected data continues to demonstrate the value of structured data.
Background and Significance
A need for collecting useful clinical information in the form of structured data has long been recognized in the realm of informatics. Witness the efforts of using pull-downs, radio buttons, and check boxes in electronic health records (EHRs)[1] and using natural language processing (NLP)[2] for this purpose. Yet the workflow of physicians, which often involves writing progress notes and dictating consults and discharge summaries, is often preferred to using screen tools which are provided. To fulfill the requirements of many EHRs, scribes are used to relieve the time pressures from working clinicians. However, some issues are recognized in efficiently translating meaningful clinical information to a scribe,[3] or accurately finding an important clinical phrase that may be used by a physician, through electronically using NLP.
Interestingly, the practice of obstetrics and gynecology uniquely lends itself to digitally recording clinical events, unlike necessarily relying on text to describe those events. For example, there is only a finite set of types of obstetric delivery. Whether an episiotomy is performed at delivery can be indicated with the use of a check box. Even defining a blood pressure measurement can be simply entered as such, without additional prose. However, the use of the EHR systems often requires additional documentation, somewhat superfluous to the documentation of care. This documentation of clinical activity remains as an obligation of providers, but the process can probably be improved upon. Having the clinical data stored for purposes of recognizing trends and applying data for research purposes is most ideal for providers, patients and society alike.[4] [5] [6] Nonetheless, recording obstetrical delivery events requires the use of screen tools which can slow the work of an obstetrician. While many events are systematically recorded in an EHR (often by nurses), only some of that specific clinical information is important to record for purposes of regulatory reporting or performing meaningful research queries.
We developed a system that records events in a structured query language (SQL) perinatal database—having a single individual manually translate the recording of notes and entries in the EHR into this SQL database—referred to as PG works (perinatal and gynecologic clinical data), as the necessary specific data elements are not automatically entered into the EHR.
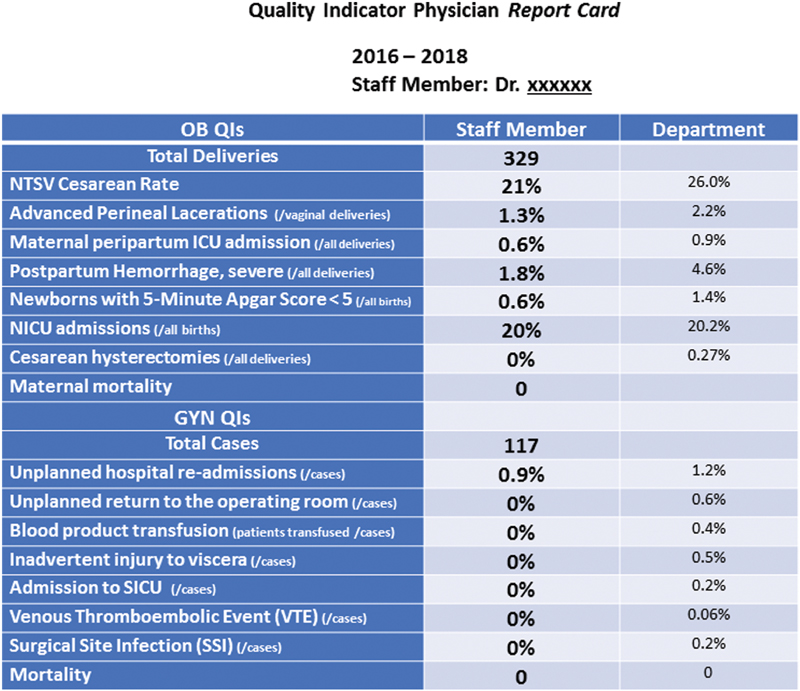
One might even label such an individual as a “central scribe.” In this case, the single individual is one full-time equivalent. The result of this is a queriable perinatal database that can be used for regulatory reporting, on-going professional performance evaluation, performance improvement, and research. The regulatory reporting included identification of the perinatal core measures (PCMs) 1, 2, and 3 (1: elective deliveries <39 weeks; 2: antepartum corticosteroid administration for the treatment for preterm deliveries; 3: and cesarean rate).[7] The OPPE was designed to demonstrate each physician's behavior regarding a variety of quality measures over a specified period of time, creating a specific “report card” ([Fig. 1]). The research activities over the years in our institution have resulted in the publication of several scholarly manuscripts.
The efficiency of this “system” was displayed in many ways and continues to be effectively used in our setting, tracking approximately 2,500 deliveries per year for the past 25 years, using a series of scribes in this way. Different information sources are used to ensure the quality and validity of the data being collected. For example, the perinatal data collected by a separate staff charged with generating birth certificates is continually compared with our own data collection system. We also have the resident staff contribute to that described efficiency for each resident's own gynecologic activity. Naturally, the sensitivity of this private health information requires proper monitoring of this data collection by the Director of Informatics, who also ensures the continued modification of the SQL system according to changes of definitions and usage consensus. This is accomplished with a software design group with whom we partnered.
This report describes this system for the many benefits that are provided to our Department of Obstetrics and Gynecology.
Reporting to the State
The state of Illinois collects perinatal data through its e-Perinet (a state-wide centralized system used to aggregate perinatal data within the state), as well as through the collection of data supporting its generation of birth certificates. All of the data necessary for submission is directly provided (via upload) to this e-Perinet system. Ease of use and the minimization of redundancy result from the use of this system for this purpose. Particular quality measures can be tracked throughout the state for this purpose, encouraging ideal perinatal management from its included medical organizations.
Reporting to the Hospital's Finance Office
PG works collect perinatal events, such as vaginal and operative deliveries, neonatal intensive care unit admissions and surgical operations. As the finance office may often be more concerned with billable events, generated reports can be used to synchronously justify billings beyond the accompanying texts. Financial reconciliation, between provider tasks and the necessary billing actions to which it is assigned, is thus possible. When such actions can occur behind the scenes, physicians are not required to perform these clerical tasks and this becomes a satisfier for physicians.
Reporting to the Accreditation Council on Graduate Medical Education
The ACGME collects resident experience through its resident case log system. Since this relevant information is already digitally collected through this SQL system, the data can be submitted via PG works reports. This further ensures the accuracy of these data—rather than simply relying on the reporting by resident physicians for their individual activity—often requiring the memory of past events, which may not always be easily accomplished.
Reporting to the Hospital System
The hospital system to which our hospital belongs, requires data collection from each hospital resulting in the measurement of the activity of each individual hospitals. Our department can provide relevant perinatal information to easily be directly reported for this purpose. When this can be accomplished in an automatic fashion, the reporting accuracy can be a source for encouraging optimal clinical behavior.
Reporting to the Center for Medicare and Medicaid Services
Since we developed our own quality measures/indicators, we can help our quality department by providing exact numbers for whatever measures are being sought. They, in turn, submit the PCMs to CMS on our behalf. The accuracy of the details that are reported is often difficult to achieve when sampling methodologies are practiced. For example, for PCM-2, determining the number of patients for whom antepartum corticosteroids were administered (per those delivered preterm) is difficult if it only relies upon EHR data entry, without considering the necessary more detailed analyses not typically found in EHR systems.
Reporting for Physician Accreditation, On-Going Professional Performance Evaluation
OPPE reporting is the current standard followed by many hospitals for physician accreditation. Each department member's clinical data, including those quality measures that are routinely collected, are systematically reported to the Department Chairman, so that a properly valid review is performed for each physician ([Fig. 1]). The more that valid performance data can be relied upon for physician evaluation, the greater the credibility such evaluations can have rather than the alternative subjective measures which are so commonly used for this.
Integration of Clinical Data with Microsoft SharePoint
As there is the need for maintaining patient lists from disparate areas in the hospital setting, we used our designed SharePoint site for maintaining a list of neonates who were transferred into our level III nursery. Keeping a record of the telephone conversations, which lead to neonatal transfers, is mandated by the state. Given the need for recording this information by individuals when using their desktops, SharePoint has been a convenient tool to use for this. The maternal and neonatal transfer information is automatically synced with the SQL system, coordinating these efforts. This enabled us to recognize the neonates transferred in (and out), and allow a comparison of outcomes between these groups, enhancing the comprehensive care continuum.
Performance Improvement and Research
Structured clinical data provide the ability to easily identify important variables which may result in positive and/or negative trends in patient outcomes. Possible interventions can then be instituted which can result in clinical improvement. One recent example of this is when examination of the cesarean delivery rate was shown to occur more commonly with induction of labor. While there are many associated variables that play a part in this, the ability to easily examine our own clinical data allowed us to design beneficial appropriate interventions, using this SQL clinical database.[8]
While efforts are often driven to mine clinical data from large databases for this purpose, resultant practice change may more effectively occur when any pertinent findings can be seen in an individual's own practice setting rather than in a described location elsewhere. The ability to illustrate one's own clinical results may be more credible, and therefore may have a greater chance of exerting any practice change which can possibly result in patient care improvement. In this way, there seems to be a benefit to structuring clinical data, to directly display the resultant clinical impact, especially when greater efficiency in patient care practice can result simultaneously.
Conclusion
EHR systems do not always and consistently capture the clinical data elements which are necessary for regulatory or quality reporting. Using this SQL system for digitally recording and organizing the important obstetrical events enabled us to efficiently perform the necessary tasks for our continued function. This system offers an example of the benefits of this technology, which can encourage others to adopt such methods. The purposes of this go well beyond those of EHRs, which are primarily devoted to legally mandated historical medical record-keeping, for producing reimbursement claims data. Proper assessment of the clinical value of any new technology requires an objective comparison to be made. However, a before and after implementation comparison was not performed in this case, as such is practically difficult when an implementation occurs over many years.
Clinical Relevance Statement
As EHRs continue to be used by physicians in the hospital environment, the important clinical information that is entered into the computer needs to be properly used for a variety of regulatory and practice improving ways. Use of a SQL system for containing this information can offer efficient use of every team member's time, in a clinical department setting. This case report illustrates that contention, suggesting that human intervention may often be necessary when collecting clinical information, and that the investment in developing such a system may be worth the effort.
Conflict of Interest
None declared.
Note
All ethical standards have been followed in the creation of this manuscript.
-
References
- 1 Palabindala V, Pamarthy A, Jonnalagadda NR. Adoption of electronic health records and barriers. J Community Hosp Intern Med Perspect 2016; 6 (05) 32643
- 2 Park A, Hartzler AL, Huh J, McDonald DW, Pratt W. Automatically detecting failures in natural language processing tools for online community text. J Med Internet Res 2015; 17 (08) e212
- 3 Pearson E, Frakt A. Medical scribes, productivity and satisfaction. JAMA 2019; 321 (07) 635-636
- 4 Eisenberg M, Hom J, Sharp C. The electronic health record as a healthcare management strategy and implications for obstetrics and gynecologic practice. Curr Opin Obstet Gynecol 2013; 25 (06) 476-481
- 5 Raglan GB, Margolis B, Paulus RA, Schulkin J. Obstetrician/gynecologists' experiences with electronic health record systems: a narrative study. J Reprod Med 2015; 60 (3-4): 95-102
- 6 McCoy MJ, Diamond AM, Strunk AL. ; American Congress of Obstetricians and Gynecologists' Committee on Ambulatory Practice Operations. Special requirements of electronic medical record systems in obstetrics and gynecology. Obstet Gynecol 2010; 116 (01) 140-143
- 7 Available at: https://www.jointcommission.org/perinatal_care/ . Accessed February 20, 2019
- 8 Altman MR, Colorafi K, Daratha KB. The reliability of electronic health data used for obstetrical research. Appl Clin Inform 2018; 9 (01) 156-162
Address for correspondence
-
References
- 1 Palabindala V, Pamarthy A, Jonnalagadda NR. Adoption of electronic health records and barriers. J Community Hosp Intern Med Perspect 2016; 6 (05) 32643
- 2 Park A, Hartzler AL, Huh J, McDonald DW, Pratt W. Automatically detecting failures in natural language processing tools for online community text. J Med Internet Res 2015; 17 (08) e212
- 3 Pearson E, Frakt A. Medical scribes, productivity and satisfaction. JAMA 2019; 321 (07) 635-636
- 4 Eisenberg M, Hom J, Sharp C. The electronic health record as a healthcare management strategy and implications for obstetrics and gynecologic practice. Curr Opin Obstet Gynecol 2013; 25 (06) 476-481
- 5 Raglan GB, Margolis B, Paulus RA, Schulkin J. Obstetrician/gynecologists' experiences with electronic health record systems: a narrative study. J Reprod Med 2015; 60 (3-4): 95-102
- 6 McCoy MJ, Diamond AM, Strunk AL. ; American Congress of Obstetricians and Gynecologists' Committee on Ambulatory Practice Operations. Special requirements of electronic medical record systems in obstetrics and gynecology. Obstet Gynecol 2010; 116 (01) 140-143
- 7 Available at: https://www.jointcommission.org/perinatal_care/ . Accessed February 20, 2019
- 8 Altman MR, Colorafi K, Daratha KB. The reliability of electronic health data used for obstetrical research. Appl Clin Inform 2018; 9 (01) 156-162