

Subscribe to RSS
DOI: 10.1055/s-0040-1708849
Peritoneovaginal Fistula and Appendicitis-Related Pelvic Abscess in Pregnancy
Authors
Address for correspondence
Publication History
21 November 2019
05 December 2019
Publication Date:
15 April 2020 (online)

Abstract
Appendicitis in pregnancy is the most common nonobstetric surgical emergency. Pregnancy causes changes in anatomy, which could lead to uncertainty regarding the diagnosis of appendicitis. This case report describes a case of appendicitis presenting with peritoneovaginal fistula in a pregnant woman in the second trimester, with interesting finding of isolated appendiceal endometriosis on pathology. The importance of complete physical examination, including speculum examination, is emphasized in the pregnant patient presenting with acute-onset abdominal pain. Imaging criteria for diagnosis of appendicitis should be adjusted to account for the gravid uterus, which may cause appendiceal abscess to appear in a variety of locations, such as posterior to the cervix, as in this case.
Keywords
peritoneovaginal fistula - acute appendicitis during pregnancy - appendiceal endometriosis - appendiceal abscessAppendicitis in pregnancy is the most common nonobstetric surgical emergency. Isolated appendiceal endometriosis in the absence of other sites of endometriosis is also uncommon. Here, we describe a case of acute appendicitis in the second trimester of pregnancy leading to a pelvic abscess and peritoneovaginal fistula with incidental pathological finding of isolated appendiceal endometriosis. The patient had an emergent appendectomy with a prolonged antibiotic course. She continued her pregnancy with no additional complications and delivered at 401/7 weeks of gestation. The infant was healthy, with no malformations, and currently exhibits no neurological or behavioral sequelae at discharge home from the hospital. We discuss the prevalence and management considerations inherent to this complex clinical scenario including clinical acuity, time from presentation to surgical management, and the importance of multidisciplinary approach to managing the patient.
Case Report
A 36-year-old Hispanic gravida 3 para 0 at 17 weeks' gestation with no significant medical history presented with lower abdominal pain for 2 days. She was seen 1 day prior to presentation for similar mild complaints and was discharged home with a diagnosis of intestinal gas. On presentation, her pain was persistent, severe, exacerbated by movement, without resolution by medical management. She had a significant loss of appetite but denied nausea or emesis. On physical examination, she was tachycardic (120 beats per minute) with involuntary guarding in the suprapubic region. Sterile speculum examination revealed a normal closed cervix with spontaneous rupture of yellow purulent fluid expulsed from the posterior vaginal fornix. This posterior vaginal wall defect could not be fully visualized. The patient expressed significant relief upon rupture, but further examination could not be tolerated. Her white blood cell count was elevated at 18.7, with a neutrophilic shift of 94%. Transvaginal ultrasound revealed a 5 cm × 2 cm complex collection in the posterior cul-de-sac, immediately posterior to the cervix, with no Doppler flow consistent with the appearance of a multiloculated abscess ([Fig. 1]). Appendicitis was not at the top of the differential diagnosis due to how inferiorly situated the abscess was; it was thought to be too distant from the appendix to represent an appendicitis or appendiceal abscess. Pelvic magnetic resonance imaging revealed a right ovarian torsion versus abscess formation due to appendicitis. While antibiotic treatment with ceftriaxone and metronidazole was given, the general surgery team was consulted. Twenty-four hours after her presentation, the patient met criteria for sepsis, and she continued to decompensate with worsening hypotension and pain. A multidisciplinary meeting was held between the obstetrics/gynecology team, maternal–fetal medicine, medical intensive care unit, and the general surgery team regarding best management practice at this juncture. Vancomycin was added to the antibiotic regimen, and the patient was brought to the operating room for diagnostic laparoscopy jointly by the general surgery and obstetrics/gynecology teams.

Examination under anesthesia revealed a 1 × 1 cm defect in the posterior fornix of the vagina with continued expression of purulent, yellow fluid. The appendix was adherent to the uterus with noted abscess and was subsequently removed. The right fallopian tube and ovary were difficult to visualize due to the acute inflammatory process and adhesions in the right lower quadrant. No additional abnormalities were appreciated. A right lower quadrant Penrose drain was placed. Fetal status was reassuring before and after the procedure.
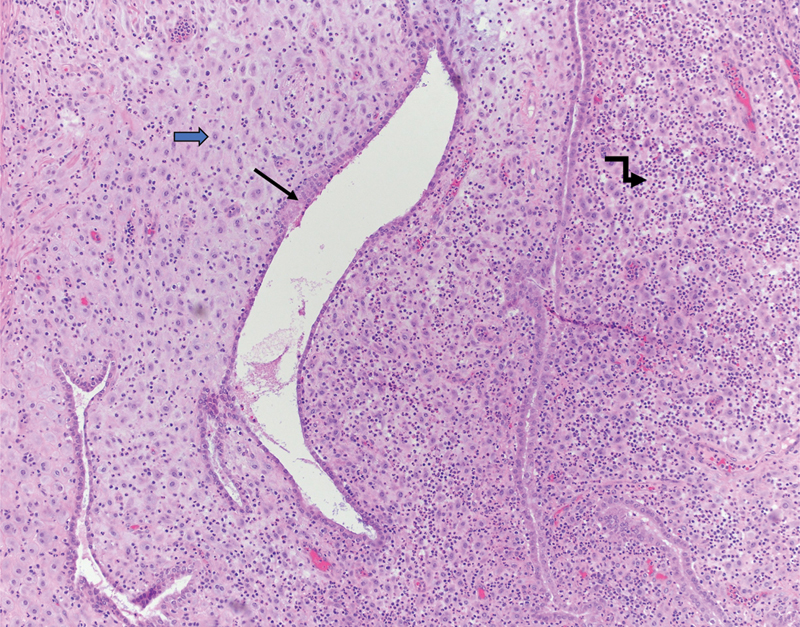
Postoperatively, the patient continued on piperacillin–tazobactam 3.375 g every 8 hours until postoperative day 5. She was slowly advanced to regular diet on postoperative day 5 with Penrose drain removal on that day. The fetal status remained reassuring during her hospital recovery. She was discharged in stable condition on postoperative day 5 with oral cefpodoxime 200 mg orally twice a day for 7 days. She was recovering appropriately at her office follow-up visit. In this case, the final diagnosis was a pelvic abscess due to acute, nonperforated appendicitis, resulting in peritoneovaginal fistula in the setting of second trimester pregnancy with endometriosis and decidualization found on pathological examination of the appendix ([Figs. 2] and [3]). The patient went on to have an uncomplicated normal spontaneous vaginal delivery at 401/7 weeks without complication.

Discussion
To our knowledge, this is the only case of a patient in the second trimester presenting with acute appendicitis leading to peritoneovaginal fistula later found to have isolated appendiceal endometriosis. There are three important points to be gleaned from this complex case, and each will be examined in turn: acute appendicitis in the pregnant patient, appendiceal endometriosis, and peritoneovaginal fistula as a consequence of appendicitis.
The incidence of nonobstetric surgical procedures in pregnant women is 0.75%.[1] It has been established that acute appendicitis is the most common surgical emergency in the pregnant patient.[2] Incidence of appendicitis is similar in the pregnant and nonpregnant population at 1/1,400 to 1/1,500.[3] In a Canadian study including more than 7,000 cases of appendicitis in pregnancy, Abbasi et al found that pregnant women with appendicitis were more likely to be black or Hispanic, similar to our patient.[3] Furthermore, they found that maternal morbidity due to appendicitis in pregnancy increases with the development of peritonitis, which our patient also exhibited. The same study found that 20% of pregnant patients with eventually diagnosed appendicitis had peritonitis, and the authors cite the difficulty in diagnosing an acute abdominal process in a pregnant patient (due to factors such as anatomical changes with the appendix moving more cephalad as early as the first trimester) as the cause of a higher rate of development of peritonitis in this population. Pregnant patients with appendicitis are also at significantly higher risk of fetal loss with concurrent peritoneal abscess formation.[4] Although our patient did not experience fetal loss, she remained at increased risk due to her peritoneal abscess.
Echoed throughout numerous studies is the point that maternal morbidity and mortality from appendicitis during pregnancy is significantly reduced by prompt surgical intervention,[3] with one study citing an increase in rupture rate by 5% after 36 hours of untreated symptoms.[5] In our case, it took ∼24 hours for the patient to be taken to the operating room for diagnostic laparoscopy. Pregnant women requiring emergent surgery are as entitled to timely intervention as the nonpregnant patient; however, uncertainty regarding the patient's diagnosis made it more challenging due to her pregnant status and contributed to the delay in surgical intervention. Based on guidelines from the American College of Obstetrics and Gynecology, a pregnant woman should never be denied surgery that has been deemed necessary, nor should that surgery be delayed regardless of trimester.[6] Regarding acute illness in the setting of pregnancy, a multidisciplinary approach is helpful and should include intensivist, obstetrician, maternal–fetal medicine specialist, among other experts as applicable, including anesthesiologists, and neonatologists (as applicable considering gestational age of fetus).[4] [7]
The prevalence of endometriosis in general varies widely, ranging from 1.5 to 15% of women.[8] It is defined as the pathological proliferation of functional endometrial tissue in extrauterine sites. When endometriosis affects the bowel, it is usually limited to superficial serosal spread.[9] Appendiceal endometriosis is a rare diagnosis. A recent review[10] cites a 2.6% prevalence for appendiceal endometriosis, but most instances in this review involved other endometriotic implants as well, which was not the case in our patient, who appeared to have isolated appendiceal endometriosis and no previous history of pelvic pain. Another study by Gustofson et al estimated that appendiceal endometriosis affects 0.4% of the general population.[11] Thus, appendiceal endometriosis may have a prevalence ranging from 0.5 to 2.6%. The rate of appendiceal endometriosis presenting as acute appendicitis during pregnancy is cited at 8/10,000 at the most.[12] Survey of the literature only revealed three case reports with a patient who had acute appendicitis during the second trimester of gestation that was later found to have evidence of appendiceal endometriosis, as in the case of our patient.[13] [14] [15] Complications of appendicitis such as perforation, peritonitis, and abscess development are more likely to occur in the case of acute appendicitis in the setting of appendiceal endometriosis. This is due to inflammatory response induced by decidua within the endometriotic appendix.[16]
Peritoneovaginal fistula is a rare complication of acute appendicitis, with only two other cases published.[10] [17] [18] [19] A case report by Yeh et al described a case of a 3-year-old girl presenting with abdominal pain and nausea, found to have appendicitis, treated with antibiotics but readmitted to the hospital with purulent fluid draining from the vagina. Similar to our patient, this child experienced significant relief of pain once the fluid began to drain from the vagina. Although this also represents a case of peritoneovaginal fistula in the setting of appendicitis, this case represents a pediatric patient rather than a pregnant adult patient such as ours. Chung-Yen et al published a case report of a woman with peritoneovaginal fistula resulting from ruptured appendicitis who also presented with vaginal discharge. There are no cases published involving peritoneovaginal fistula due to acute appendicitis in the setting of pregnancy. Although our patient did not present with vaginal discharge, it was immediately obvious upon speculum examination that there was an intraperitoneal process connecting to the vagina. Prompt physical examination, including a speculum examination, may lead to more timely identification of correct diagnosis in pregnant patients presenting with significant abdominal pain. Inflammation of the appendix, likely compounded by inflammatory reaction by decidua within this endometriotic appendix may have contributed to this rare fistulization.
Conclusion
This case report described a patient in the second trimester of pregnancy presenting with signs and symptoms concerning for acute intra-abdominal process, ultimately found to have appendicitis. The appendicitis was complicated by peritoneovaginal fistula, which is an uncommon occurrence, previously reported only outside of pregnancy. Further, the appendix was found to have endometriosis, which is also a rare phenomenon. This case highlights the value of timely and complete physical examination. It also demonstrates the importance of maintaining a high index of suspicion for appendicitis, even when abscess fluid collects in the posterior cul-de-sac, seemingly distant from and unrelated to the appendix. Furthermore, this case underscores the benefit of interdisciplinary collaboration in the case of complex presentation of appendicitis, further complicated by the gravid state.
Conflict of Interest
None.
-
References
- 1 Mazze RI, Källén B. Reproductive outcome after anesthesia and operation during pregnancy: a registry study of 5405 cases. Am J Obstet Gynecol 1989; 161 (05) 1178-1185
- 2 Tamir IL, Bongard FS, Klein SR. Acute appendicitis in the pregnant patient. Am J Surg 1990; 160 (06) 571-575 , discussion 575–576
- 3 Abbasi N, Patenaude V, Abenhaim HA. Management and outcomes of acute appendicitis in pregnancy-population-based study of over 7000 cases. BJOG 2014; 121 (12) 1509-1514
- 4 McGory ML, Zingmond DS, Tillou A, Hiatt JR, Ko CY, Cryer HM. Negative appendectomy in pregnant women is associated with a substantial risk of fetal loss. J Am Coll Surg 2007; 205 (04) 534-540
- 5 ACOG Committee Opinion Number 775: non obstetric surgery during pregnancy. Obstet Gynecol 2019; 133 (04) e285-e286
- 6 Bickell NA, Aufses Jr AH, Rojas M, Bodian C. How time affects the risk of rupture in appendicitis. J Am Coll Surg 2006; 202 (03) 401-406
- 7 Guntupalli KK, Hall N, Karnad DR, Bandi V, Belfort M. Critical illness in pregnancy: part I: an approach to a pregnant patient in the ICU and common obstetric disorders. Chest 2015; 148 (04) 1093-1104
- 8 Ballard KD, Seaman HE, de Vries CS, Wright JT. Can symptomatology help in the diagnosis of endometriosis? Findings from a national case-control study--Part 1. BJOG 2008; 115 (11) 1382-1391
- 9 Shen AY, Stanes A. Isolated appendiceal endometriosis. J Obstet Gynaecol Can 2016; 38 (10) 979-981
- 10 Mabrouk M, Raimondo D, Mastronardi M. , et al. Endometriosis of the appendix: when to predict and how to manage-a multivariate analysis of 1935 endometriosis cases. J Minim Invasive Gynecol 2020; 27 (01) 100-106
- 11 Gustofson RL, Kim N, Liu S, Stratton P. Endometriosis and the appendix: a case series and comprehensive review of the literature. Fertil Steril 2006; 86 (02) 298-303
- 12 Lebastchi AH, Prieto PA, Chen C, Lui FY. Appendiceal endometriosis in a pregnant woman presenting with acute perforated appendicitis. J Surg Case Rep 2013; 2013 (12) rjt104
- 13 Nakatani Y, Hara M, Misugi K, Korehisa H. Appendiceal endometriosis in pregnancy. Report of a case with perforation and review of the literature. Acta Pathol Jpn 1987; 37 (10) 1685-1690
- 14 Giorgakis E, Karydakis V, Farghaly A. Perforated endometrial appendicitis in pregnancy. Hippokratia 2012; 16 (02) 181-183
- 15 Murphy SJ, Kaur A, Wullschleger ME. Endometrial decidualization: a rare cause of acute appendicitis during pregnancy. J Surg Case Rep 2016; 2016 (04) rjw053
- 16 Perez CM, Minimo C, Margolin G, Orris J. Appendiceal endometriosis presenting as acute appendicitis during pregnancy. Int J Gynaecol Obstet 2007; 98 (02) 164-167
- 17 Yeh D, Moyles K, Ekwenna O, Thompson WR, Neville HL, Sola JE. Spontaneous vaginal drainage of a pelvic abscess: an unusual presentation of perforated appendicitis. Pediatr Emerg Care 2009; 25 (12) 856-858
- 18 Sander S, Eliçevik M, Unal M, Vural O. An unusual presentation of appendicitis: vaginal discharge. J Pediatr Surg 2001; 36 (10) 1579-1580
- 19 Chung-Yen Chen C-FF, Chuang H-Y, Katakwar A, Chang PC. Peritoneovaginal fistula alleviated ruptured appendicitis-related pelvic abscess. E Da Med J 2017; 4 (02) 24-27
Address for correspondence
-
References
- 1 Mazze RI, Källén B. Reproductive outcome after anesthesia and operation during pregnancy: a registry study of 5405 cases. Am J Obstet Gynecol 1989; 161 (05) 1178-1185
- 2 Tamir IL, Bongard FS, Klein SR. Acute appendicitis in the pregnant patient. Am J Surg 1990; 160 (06) 571-575 , discussion 575–576
- 3 Abbasi N, Patenaude V, Abenhaim HA. Management and outcomes of acute appendicitis in pregnancy-population-based study of over 7000 cases. BJOG 2014; 121 (12) 1509-1514
- 4 McGory ML, Zingmond DS, Tillou A, Hiatt JR, Ko CY, Cryer HM. Negative appendectomy in pregnant women is associated with a substantial risk of fetal loss. J Am Coll Surg 2007; 205 (04) 534-540
- 5 ACOG Committee Opinion Number 775: non obstetric surgery during pregnancy. Obstet Gynecol 2019; 133 (04) e285-e286
- 6 Bickell NA, Aufses Jr AH, Rojas M, Bodian C. How time affects the risk of rupture in appendicitis. J Am Coll Surg 2006; 202 (03) 401-406
- 7 Guntupalli KK, Hall N, Karnad DR, Bandi V, Belfort M. Critical illness in pregnancy: part I: an approach to a pregnant patient in the ICU and common obstetric disorders. Chest 2015; 148 (04) 1093-1104
- 8 Ballard KD, Seaman HE, de Vries CS, Wright JT. Can symptomatology help in the diagnosis of endometriosis? Findings from a national case-control study--Part 1. BJOG 2008; 115 (11) 1382-1391
- 9 Shen AY, Stanes A. Isolated appendiceal endometriosis. J Obstet Gynaecol Can 2016; 38 (10) 979-981
- 10 Mabrouk M, Raimondo D, Mastronardi M. , et al. Endometriosis of the appendix: when to predict and how to manage-a multivariate analysis of 1935 endometriosis cases. J Minim Invasive Gynecol 2020; 27 (01) 100-106
- 11 Gustofson RL, Kim N, Liu S, Stratton P. Endometriosis and the appendix: a case series and comprehensive review of the literature. Fertil Steril 2006; 86 (02) 298-303
- 12 Lebastchi AH, Prieto PA, Chen C, Lui FY. Appendiceal endometriosis in a pregnant woman presenting with acute perforated appendicitis. J Surg Case Rep 2013; 2013 (12) rjt104
- 13 Nakatani Y, Hara M, Misugi K, Korehisa H. Appendiceal endometriosis in pregnancy. Report of a case with perforation and review of the literature. Acta Pathol Jpn 1987; 37 (10) 1685-1690
- 14 Giorgakis E, Karydakis V, Farghaly A. Perforated endometrial appendicitis in pregnancy. Hippokratia 2012; 16 (02) 181-183
- 15 Murphy SJ, Kaur A, Wullschleger ME. Endometrial decidualization: a rare cause of acute appendicitis during pregnancy. J Surg Case Rep 2016; 2016 (04) rjw053
- 16 Perez CM, Minimo C, Margolin G, Orris J. Appendiceal endometriosis presenting as acute appendicitis during pregnancy. Int J Gynaecol Obstet 2007; 98 (02) 164-167
- 17 Yeh D, Moyles K, Ekwenna O, Thompson WR, Neville HL, Sola JE. Spontaneous vaginal drainage of a pelvic abscess: an unusual presentation of perforated appendicitis. Pediatr Emerg Care 2009; 25 (12) 856-858
- 18 Sander S, Eliçevik M, Unal M, Vural O. An unusual presentation of appendicitis: vaginal discharge. J Pediatr Surg 2001; 36 (10) 1579-1580
- 19 Chung-Yen Chen C-FF, Chuang H-Y, Katakwar A, Chang PC. Peritoneovaginal fistula alleviated ruptured appendicitis-related pelvic abscess. E Da Med J 2017; 4 (02) 24-27