
RSS-Feed abonnieren
DOI: 10.1055/s-0034-1391259
Huge hemothorax caused by endoscopic ultrasound-guided fine-needle aspiration of a submucosal tumor of the gastric fornix
Corresponding author
Publikationsverlauf
Publikationsdatum:
17. Februar 2015 (online)

Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) is the most efficacious method for sampling solid lesions adjacent to the gastrointestinal tract. A recent meta-analysis of EUS-FNA complications reported a bleeding rate of 0.13 % [1]. Here, we present a case of hemothorax in a patient receiving anticoagulant therapy for myocardial infarction and atrial fibrillation. The hemothorax developed after the patient underwent EUS-FNA for a gastric submucosal tumor.
A 72-year-old man with an asymptomatic gastric submucosal tumor was admitted for a histologic diagnosis. He had been taking clopidogrel and aspirin regularly for 4 years. A gastric submucosal tumor had been detected 2 years previously and was increasing in size, as seen on computed tomography ([Fig. 1]). The clopidogrel and aspirin were discontinued for 5 days prior to EUS-FNA and on the day of EUS-FNA.

Esophagogastroduodenoscopy revealed a submucosal tumor of the gastric fornix ([Fig. 2]). EUS revealed a well-defined hypoechoic mass with no intervening vessels ([Fig. 3 a]). EUS-FNA was performed with a 19-gauge needle and two needle passes ([Fig. 3 b]).


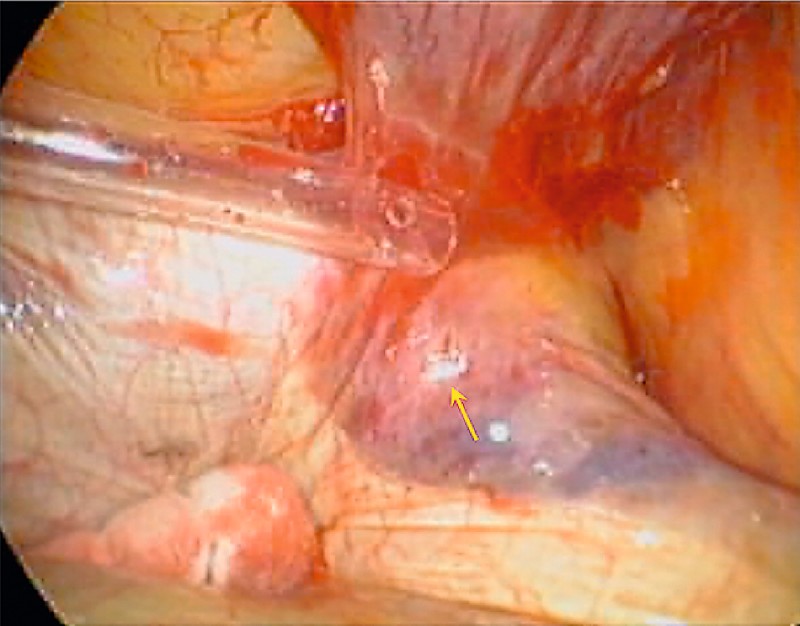
Immediately after the EUS-FNA, no intratumoral or local bleeding was observed at the puncture site. However, 5 hours later, tachypnea and dyspnea developed. Computed tomography of the chest revealed a left hemothorax ([Fig. 4]), and chest tube drainage was carried out immediately. Nonetheless, progressive anemia developed. Video-assisted thoracoscopic surgery was performed, revealing a needle tract penetrating the diaphragm adjacent to the esophagus ([Fig. 5]). Hematomas were observed beyond the diaphragmatic penetration site, suggesting that the bleeding originated from the submucosal tumor. Although the tumor was visualized from the stomach, the needle may have punctured the submucosal tumor through the esophagus wall, not entering the abdominal cavity, and caused bleeding into the thoracic cavity. The patient was discharged on postoperative day 9.

To our knowledge, this is the first report of hemothorax as a complication of EUS-FNA. The possibility of hemothorax should be considered in patients undergoing EUS-FNA of lesions of the gastric fornix.
Endoscopy_UCTN_Code_CCL_1AB_2AC_3AZ
#
Competing interests: None
-
Reference
- 1 Wang KX, Ben QW, Jin ZD et al. Assessment of morbidity and mortality associated with EUS-guided FNA: a systematic review. Gastrointest Endosc 2011; 73: 283-290
Corresponding author
-
Reference
- 1 Wang KX, Ben QW, Jin ZD et al. Assessment of morbidity and mortality associated with EUS-guided FNA: a systematic review. Gastrointest Endosc 2011; 73: 283-290