

Subscribe to RSS
DOI: 10.1055/s-0034-1384802
Milestones in Surgery: 60 Years of Open Heart Surgery
Authors
Address for correspondence
Publication History
28 March 2014
23 May 2014
Publication Date:
01 August 2014 (online)
Abstract
Long periods of experimental research signify the struggle for the goal to substitute the functions of heart and lungs by a machine. In 1931, John Heysham Gibbon, a young surgeon in Boston began animal experiments concentrating on this task. After almost 20 years he succeeded, in May 1953, he performed the first successful open heart operation using a heart–lung machine in the world in Philadelphia. Almost simultaneously, a team of surgeons around Clarence Walton Lillehei in Minneapolis had the same intentions, yet using a different approach. They applied the method of cross-circulation where a parent of the sick child served as “temporary placenta” like a biological oxygenator. Their first successful operation occurred in March 1954. All over the world, many scientists worked intensely on that subject, but did not succeed. However, these two great personalities, persistent and ingenious, reached the same scientific target with very different methods. Thus, both created the foundation for modern cardiac surgery, which is now performed daily all over the world.
Introduction
Part of this material was presented as a lecture at the 43rd Annual Meeting of the German Society for Thoracic and Cardiovascular Surgery, Freiburg, Germany, February 10, 2014.
This article looks back into the history of cardiac surgery, more precisely the history of open heart operations.
Just about a hundred years ago, surgical treatment of congenital cardiac anomalies or valvular heart disease was regarded as “pure fantasy.” The well-known Berlin vascular surgeon Ernst Jeger writes in his book on: “Surgery of Blood Vessels and the Heart” published by A. Hirschwald, Berlin, 1913[1]: “It is indeed absolutely non-scientific to express certain hopes in the development of that field. On the other hand it is also quite non-scientific to deny any future for surgery of the heart.”
This view appears surprising today because physiologists had already tried to substitute the functions of the heart and lungs by a machine since 1885. Those experimental researchers were talking about a “respiratory apparatus” or an oxygenator.[2] The idea that such a device might someday be useful for mankind developed some decades later. In February 1931, a young resident, John Heysham Gibbon at the Boston Massachusetts General Hospital, was watching over a patient with massive pulmonary embolism after cholecystectomy.[3] [4] During the long night, envisioning totally helpless the fight of this patient for survival, in Gibbon's mind a visionary dream was forming: the blood becoming darker and darker, the veins extending more and more, he created the idea to extract some of the used dark blood, extract its CO2, replacing it with oxygen and to reinfuse the freshly oxygenated blood into the patient. By bypassing the thrombotic obstruction, the work of the heart and lungs would be reduced and transmitted outside of the body.
This revolutionary idea persisted in Gibbon's thoughts and he began to extend his experimental work in that direction. Together with his coworker and later wife Mary Hokinson, called Maly, he built an oxygenator: venous blood was flowing tangentially in a rotating metallic cylinder, the thin blood film was exposed to oxygen. On the bottom of the cylinder, the oxygenated blood was collected in a glass container which was surrounded by circulating warm water serving as a heat exchanger. A variety of pumps were available at that time. Gibbon and his team tested their apparatus on cats. They caught them on the streets using tuna as a bait so they did not have to buy them. The cats were connected to their machine, their venous blood drawn and reinfused after oxygenation. To simulate cardiopulmonary arrest, the pulmonary artery was occluded. After several experiments success occurred on May 10, 1935: using their machine they were able to sustain cardiopulmonary function for 39 minutes. This was indeed a remarkable achievement, Gibbon and his Maly were dancing with jubilation in their laboratory.[3] [5] [6] They continued their research program with intensity and enthusiasm refining their technique, the experiments becoming better and better. Four years later, 1939, they reported their results at the Meeting of the American Association for Thoracic Surgery: four cats had survived in healthy condition after 20 minutes of substitution of heart–lung function using their extracorporeal device. Gibbon stated in his presentation, “It is conceivable that a diseased mitral valve might be exposed to surgical approach under direct vision and that the fields of cardiac and thoracic surgery might be broadened.” If one considers the unbelievable possibilities for the future, Gibbon appeared quite modest. The president of the society commented: “This reminds me of the fantastic tales of Jules Verne, who anticipated impossible accomplishments which perhaps one day will become reality.”[6] [7] [8]
Six years later, after the war, research in that field continued in many laboratories in the world, in particular, in Sweden, England, and the United States. They all worked on the construction of a circulatory machine following the principles of experiments Gibbon had initiated.[9]
An exceptional example of this outstanding fight for progress is represented by the experimental work of Clarence Dennis and Richard Varco in Minneapolis. They also modified Gibbon's heart–lung machine. After 6 years of intensive work in the dog laboratory, they decided in 1951 to operate on a patient. There were 16 physicians at the time of operation, four of which were assigned to the heart–lung machine. They operated on three very sick girls, but none survived. The causes of death were two diagnostic errors and in one case a pump technician suffering from the flu forgot to put in the safety mechanism against air embolism! In all three cases, however, the pump had supported the circulatory function without problems up to 40 minutes. Despite this, Dennis gave up, despaired, and disappointed by the professional errors at the fatal operations.[5] [6] [8]
But with the beginning of 1951, these heroic achievements determined an important signpost for the future of open heart surgery. Worldwide several other trials of intracardiac operations using a heart–lung machine occurred but they all failed. There was a common scenario for all: good results in animal experiments, but bad results in sick human hearts. The logical conclusion was conceivable that a sick myocardium will not tolerate such an invasive therapy. Immediately a “sick human heart theory” evolved that eventually particular substances would have to be elaborated to ensure clinical success. The future of cardiac surgery was very much in doubt.[5] [8] [10] Just a few, like John Gibbon, did not give up. Meanwhile, since 1946, he had advanced to Director of Surgical Research at the Jefferson Medical College in Philadelphia. He resumed work at his heart–lung machine with the professional aid of five engineers of the Internal Business Machine Corporation (IBM). Using some generous financial support they constructed “Model I” in 1949 and “Model II” in 1951. In his final model, he used a screen oxygenator. After years of steady and tedious experimental work—yet 88% of his animals survived—John Gibbon dared to operate on a 15-year-old girl diagnosed with atrial septal defect (ASD) at the end of 1952. The heart–lung machine worked perfectly, but the child died because the ASD could not be identified. An autopsy revealed a large patent Ductus Botalli. Several months passed until the team performed a second operation in an 18-year-old girl with ASD on May 6, 1953. The machine worked perfectly for 45 minutes overall, with a total bypass time of 26 minutes, and the operation was successful ([Fig. 1]).[11]
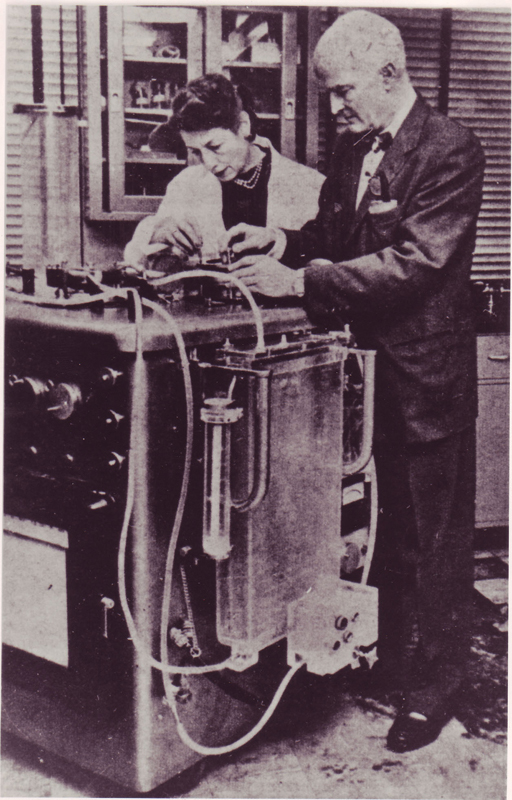
This was the first successful open heart operation on a patient with the aid of total cardiopulmonary bypass in the world. A milestone in surgery, the effect on the new capabilities to deal with up to now incurable cardiac anomalies was enormous. The echo of national and international professional organizations was one of full esteem, admiration, and appreciation. Gibbon, however, could not repeat his success. Frustrated after two additional fatal procedures, he announced a moratorium of 1 year for his machine. As a matter of fact, he never again performed an operation with his device. The risk of technical failures and possible dangers for the patient were, in his mind, unsurmountably high, and he abandoned his task. Gibbon was a dedicated and meticulous pioneer of cardiac surgery. His ingenious ideas and work, beginning 1931, represent the origin of a historic breakthrough in medical history. In 1974, he was proposed for the Nobel Prize, but he had succumbed before, on February 5, 1973, during a tennis match due to myocardial infarction, just a few months before the 20th anniversary of the epoch-making operation with his heart–lung machine.[6] [8]
In Minneapolis, in 1951, a young scientist had watched with eager interest the first operations with a pump by Dennis and Varco from a ladder: Clarence Walton Lillehei. Since Dennis had moved to New York, Lillehei was supposed to succeed with his projects. He, however, regarded the heart–lung machine as too complicated. Apart from his laboratory in the attics of Millard Hall, two colleagues, Morley Cohen and Herbert E. Warden, were experimenting on an alternative route: they used dog's lungs as oxygenators. In their experiments, they connected the donor's circulation to the circulation of a second animal, thus the donor animal served as heart and lungs for the “patient.” Even though the lungs as biological tissue undoubtedly do not damage the blood in comparison to a machine, the procedure turned out to be liable to dangers: for instance, smallest changes of resistance in the system would produce pulmonary edema with fatal results.[2] [10] [12] Nevertheless, Lillehei and his team continued their experiments and had increasing success. Just for exercise, they produced a ventricular septal defect (VSD) in a dog and occluded it using their techniques. To recognize possible neurological damages, Lillehei bought golden retrievers, who, as hunting dogs, showed a specific and constant pattern of behavior. After some successful experiments, the dogs remained hounds. Thus, the procedure of cross-circulation was born. The value of this method for cardiac surgery was evaluated during long and often hot-headed discussions about pro and cons of this method. Somehow the idea prevailed to employ a healthy individual as a donor for correction of a sick patient quasi as a temporary placenta.[10] [12] Lillehei was looking for a candidate for his first operation using cross-circulation ([Fig. 2]).

Meanwhile in Minneapolis, the first special heart hospital of the world was put into effect, the Variety Club Heart Hospital. This hospital was a charity of a Minnesota business man: a four-storey building on the shore of the Mississippi river, with a separate ward for children and adults, a floor for research, and an outpatient department. The designers of the building considered the significance of a certain psychology for sick patients, for instance, the importance of colors: besides white, there were brown, red, and greens. In winter, the lobby was warmed by a fireplace.[10]
In this hospital, Gregory Glidden, 8 months old, was treated because of cardiac failure due to his VSD diagnosed by cardiac catheterization. The actual medical opinion at that time was that there existed no treatment for this patient. Lillehei and his team, Varco, Cohen, and Warden, decided to operate on Gregory. They used their preoperative time to study the anatomy of the human heart not only in the local pathology department but also 90 miles south at the Mayo Clinic in Rochester. There was the home of the most famous cardiac pathologist of the world, Jesse E. Edwards. He had collected an enormous number of specimens of human hearts, stored in wooden pickle barrels filled with formalin. They spent days with Edwards to think over the potential technique to close VSDs, using Edwards' 50 specimens. It was frightening that each of the VSDs was different. Would they be able to identify the VSD in Gregory's heart? Would the stitches tear through the sick myocardial muscle? And, in particular, where was the course of the conduction system? A total atrio-ventricular block (a-v block) at that time represented a lethal complication. Loaded with such thoughts, the team returned to Minneapolis at the day before the operation. Finally, all doubts were ended after visiting a bar on their way home, the owner a former patient of Lillehei. The procedure with cross-circulation was planned for the next day, March 26, 1954. Meanwhile, the father of the 16 months old Gregory would serve as donor. It is indeed mandatory to imagine the actual circumstances at that time ([Fig. 3]).

In the early morning of the day of the operation, Varco had operated on a stomach and Lillehei on an inguinal hernia. The operating room (OR) was just big enough for two tables next to each other, one for the patient and the other for the donor. It had a white-tiled floor, green walls, and windows, in the corner a steam sterilizer. On hot summer days, the windows were opened in the hope of catching a breeze from the nearby Mississippi river. The equipment was state of the art for 1954: for supervision of the patient blood pressure was measured with a cuff around the arm, fingers felt the pulse at the wrist, a glass thermometer registered the patient's temperature. There was an electrocardiogram, but due to electrical interference, it was mostly unreliable. The most important device in this room was the big clock on the wall. Anesthesia was manual work. Respirators were not existent, and the patient was ventilated manually with a black rubber bag. The highly inflammable ether was substituted by the also explosive cyclopropane. To avoid static discharges, special OR shoes were mandatory; female employees were encouraged not to wear silk underwear, since any spark might induce an explosion. As a matter of fact, in 1954, 130 explosions had occurred in American ORs in which 30 people had died.[10]
One day before the operation, the medical director and the head of administration heard about the planned procedure. Immediately, they tried to stop the operation: eventually the life of two patients was in danger. Finally, the strong arguments of the chief of surgery, Owen Wangensteen, succeeded. The pioneers were allowed to go ahead.
It was March 26, 1954, 8 hours 30 minutes in the morning when the team started with Gregory. After thoracotomy and inspection of the situs, the father was prepared as donor using a light narcosis and local anesthesia in the groin. Like in the animal experiments, the surgeons connected the circulation of father and child with tubes and their pump. After opening the right ventricle, the area was not bloodless, but using some suction they could identify the VSD, approximately 12 mm in diameter. Lillehei closed it with single stitches, the ventriculotomy with a continuous silk suture. The cross-circulation time was 19 minutes. The father survived after the operation without problems. The son stayed for 5 hours in the recovery room and was then transferred to his room on the ward. An intensive care unit was not existent. A nurse was attending Gregory day and night, Lillehei or one of the team was present continuously. Gregory's circulatory condition was stable, all organs were functioning, the child was alert, already enjoying food. But suddenly, on the 7th postoperative day, the respiration deteriorated. Immediately, antibiotics were administered and a tracheotomy performed, but the boy died 11 days after the operation due to pneumonia. Despite this, another milestone in cardiac surgery had been established. Lillehei continued with his ideas with emphasis and enthusiasm. As a matter of fact, two additional similar operations in April 1954 were successful.[10] [12]
Now Lillehei went public: he gave a press conference, very probable the first press conference of a surgeon ever, presenting his patients. The echo was breathtaking, the newspapers tumbled over: “miracle, fantastic, impossible surgery, revolutionary!”[10]
Just a little later, Lillehei presented his scientific data to the medical world. The basic consideration was what he called the “azygos factor”: As a result of some earlier animal experiments it was an accepted fact that after occlusion of both venae cavae the flow from the now dilated vena azygos appeared sufficient for organ perfusion.[2] [12] In other words, an organism at rest, here the “donor,” will have sufficient perfusion if the blood flow is one-third of normal with no organ damage observed. Yet, in the recipient, this low flow will induce metabolic acidosis due to some tissue hypoxia. The donor will compensate that with hyperventilation and respiratory alkalosis. In addition, the donor will lack approximately 4 to 20% of his cardiac output depending on the size of the patient. In addition, one has to consider that after opening the beating heart some blood loss is inevitable. At that time, there was no cardiac suction, blood gases, or electrolytes were not measured, no defibrillator or pacemaker existed. Furthermore, there was just a recovery room, artificial respiration was not possible. During the next months, Lillehei continued his work quite intensely. Some spectacular results should be mentioned like the correction of a total atrioventricular canal. On August 31, 1954, he succeeded in correcting a tetralogy of Fallot, at that time considered the Mount Everest of cardiac surgery.
With such news, he electrified the audience at the first Henry Ford Symposium in Detroit in 1955. Conversely, several failures happened, the mortality ranged above 50%. Lillehei always felt full responsibility and insisted to bring the bad news to the parents himself. In the world of cardiac doctors, however, there was quite some uproar, some even called him “murderer.” Helen Taussig, for instance, commented on his success cynically: “Too bad, now he will continue.”[10] [13] [14] [15] [16]
A disgraceful curiosity of that time should also be mentioned here. A 13-year-old boy was admitted with a traumatic VSD after a car accident. He was an African American from Arkansas. It turned out to be impossible to find a donor for that child, not even in jails, where Lillehei had hoped to find volunteers. At that time, in the 1950s, a white donor for a colored child was unthinkable, the mixing of blood was not accepted. Just to save the child Lillehei decided to employ a dog's lung. In Minneapolis, as mentioned, dog lungs were used as oxygenators. For this particular task, he preferred a country dog instead of a city dog in the opinion that the former's lung would be the healthier one. On March 16, 1955, the boy was operated on and survived. It was a remarkable success.[10]
Within 14 months, Lillehei operated on 45 children aged 4 months to 14 years. Fifteen were younger than 1 year old, all operated on with cross-circulation. The diagnoses were VSD, atrioventricular canal, and tetralogy of Fallot. Reasonably, good results were obtained in children in whom the VSD was closed without patch. After some months, Lillehei realized that a patch would permit a more secure closure of the VSD. His first patches were cut from an Ivalon kitchen sponge. Bypass times varied between 6 and 40 minutes; 28 patients, that is, 62%, left the hospital. Today, after 60 years, 20 former patients are alive and in stable condition.[17]
Then a crucial decision was made, actually a further milestone in the history of open heart surgery: in August 1955, Lillehei, with courageous self-criticism, determined to discontinue cross-circulation. He acknowledged the fact that there were always two individuals exposed to danger, even though only one of his donors had suffered damage from air embolism. Lillehei nourished the conviction that further progress could only be achieved using the heart–lung machine. From that day on Lillehei operated with the Travenol Bag, a disposable oxygenator developed by his coworker Richard De Wall.[12] [16]
Another modification of Gibbon's machine was used at the Mayo Clinic by John W. Kirklin, a classmate of Lillehei. This “Mayo–Gibbon machine” had the dimensions of a Wurlitzer organ, being technically highly sophisticated and quite expensive. Kirklin, a diligent thinker and at that time already the pure statistician, had selected eight children for operation with the decision to operate in any case disregarding the results, just to fulfill statistics. Fifty percent survived the operation, Kirklin carried on. At that time, all over the world, only two surgeons were performing open heart operations using a heart–lung machine: Kirklin and Lillehei. Their results were spread worldwide, thus scientists and surgeons were flooding these two “lighthouses” of open heart operations in Minneapolis and Rochester.[2] [9] [10]
Until the end of 1957, Lillehei had operated on 413 patients, the largest series of open heart operations in the world. Some marginal problems could be solved quite promptly, for instance, heart bloc. Lillehei was able to overcome this problem with a temporary pacemaker: Earl Bakken, a former TV mechanic, had developed such a device in his garage. Later on, this became the basis for the Medtronic Company. On August 12, 1960, Lillehei celebrated the 1,000th open heart operation with his team. Since he was not selected as successor of his teacher and promoter, Owen Wangensteen, he moved to the Cornell Medical Center in New York at the end of 1967 ([Fig. 4]).

As bright as Lillehei's reputation as cardiac surgeon appeared, his final professional years were overshadowed by personal problems. For instance, one criticized his unconventional behavior in the OR: there the young residents were allowed to open the thorax, he entered the OR when all the preparations of the heart were finished. At that time, this was absolutely intolerable. During the operation a radio played, this was considered impossible. Organization of his finances was chaotic, cheques from patients were lying for months in some drawer or a cardboard box, and bills were indeterminable. He had operated on some patients for nothing. Considerable tax debts led to an inevitable law suit. Because of his awkward behavior and chaotic management, Lillehei lost his position as chief of the department in April 1970. Due to progressive ophthalmological problems, he terminated his career as a surgeon in December 1973.[10] [12]
I met C. Walton Lillehei in spring 1979 at the meeting of the American Association of Thoracic Surgery (AATS) in Boston. The president of the association, John Kirklin, and the auditorium honored him with an impressive standing ovation, a commemorative demonstration. In a short laudatio Kirklin emphasized the extraordinary achievements of this scientist and surgeon, regretting that fate had denied him a “Lillehei Operation” even though he had performed many operations as a first. Lillehei died a few months before his 81st birthday. The great heart surgeons of our time, John W. Kirklin, Denton A. Cooley, and Norman E. Shumway, granted him the honorary title “father of cardiac surgery.” In 1955, Lillehei and his team had already been honored with the outstanding “Lasker Award,” often called the “American Nobel Prize.”
Looking at the history of cardiac surgery, there is indeed a scientific enlightenment in the first half of the 1950s. The initiative and sparkling ideas originated from the universities and scientific institutions of the United States, in particular, from Philadelphia and Minnesota. In Europe, Sweden, and England started as early as 1954. In Germany, a short time after the Second World War, cardiac surgery suffered a “dull awakening” as Rudolf Nissen stated it. There the first successful open heart operation was performed by Rudolf Zenker on a 30-year-old patient on February 19, 1958, at the University of Marburg, using a modified screen oxygenator by Kay-Gaertner.[9]
In the United States, two surgeons of different temper and character had initiated the onset and breakthrough of open heart surgery: J.H. Gibbon was a diligent and meticulous surgeon, very scrupulous with a high ethical conscience but also modest and reserved. Perhaps he resigned too early? Without doubt Gibbon remains the genius pioneer of cardiac surgery. Conversely, C. Walton Lillehei was the passionate, almost obsessed, surgeon and scientist. Nothing could stop his persistent and heroic experimental spirit and impetus. His fascinating activity was motivation for generations of students and successors.
Certainly, as impressive as the accomplishments of Gibbon and Lillehei were they would not have been possible without colleagues and competitors, without friends, and critics. In Gibbon and Lillehei surgical progress is represented by two great personalities. Their culminating scientific targets were the same, pursued in their very different routes.[18]
Today, open heart surgery has become a routine procedure. All over the world, well-trained surgeons perform open heart operations successfully on thousands of patients. Even very sick patients have a chance for rehabilitation in a high percentage, gaining precious years of a high-quality life. The breakthrough to these achievements originated 60 years ago. The pioneers of modern cardiac surgery, upfront John H. Gibbon and C. Walton Lillehei, deserve that we commemorate their work.
-
References
- 1 Jeger E. Die Chirurgie der Blutgefässe und des Herzens. Berlin: August Hirschwald; 1913
- 2 Rodewald G, History of extracorporeal circulation. In: Hagl S, Klövekorn WP, Mayr N, Sebening F. , eds. Proceedings of the Symposium Thirty Years of Extracorporeal Circulation; April 5–7; 1984: 25-43 ; Munich, Germany: Dtsch Herzzentrum München
- 3 Gibbon Jr JH. The gestation and birth of an idea. Phila Med 1963; 59: 913
- 4 Shumacker Jr HB. John Heysham Gibbon Jr September 29, 1903–February 5, 1973. Biographical Memoirs. Vol 53. Washington DC: National Academy Press; 1982: 213-247
- 5 Hill JD, Gibbon John Jr H. Part I. The development of the first successful heart-lung machine. Ann Thorac Surg 1982; 34 (3) 337-341
- 6 Dobell ARC, Gibbon John Jr H. Part II. Personal reminiscences. Ann Thorac Surg 1982; 34 (3) 342-344
- 7 Gibbon Jr JH. Artificial maintenance of circulation during experimental occlusion of pulmonary artery. Arch Surg 1937; 34: 1105-1131
- 8 Shumacker Jr HB, A Dream of the Heart. The life of John H. Gibbon Jr. , Father of the Heart-Lung Machine. Santa Barbara: Fithian Press; 1999
- 9 Zenker R. Zur Geschichte und Entwicklung der Herzchirurgie. , in: Herz und herznahe Gefäße. Berlin, Heidelberg, New York: Springer-Verlag; 1978. : S. 1-14
- 10 Miller GW. King of Hearts: The True Story of the Maverick Who pioneered Open Heart Surgery. New York: Crown Publishers; 2000
- 11 Gibbon Jr JH. Application of a mechanical heart and lung apparatus to cardiac surgery. Minn Med 1954; 37 (3) 171-185 , passim
- 12 Lillehei CW. A personalized history of extracorporeal circulation. Trans Am Soc Artif Intern Organs 1982; 28: 5-16
- 13 Lillehei CW, Cohen M, Warden HE, Ziegler NR, Varco RL. The results of direct vision closure of ventricular septal defects in eight patients by means of controlled cross circulation. Surg Gynecol Obstet 1955; 101 (4) 446-466
- 14 Lillehei CW, Cohen M, Warden HE, Varco RL. The direct-vision intracardiac correction of congenital anomalies by controlled cross circulation; results in thirty-two patients with ventricular septal defects, tetralogy of Fallot, and atrioventricularis communis defects. Surgery 1955; 38 (1) 11-29
- 15 Lillehei CW, Cohen M, Warden HE , et al. Direct vision intracardiac surgical correction of the tetralogy of Fallot, pentalogy of Fallot, and pulmonary atresia defects; report of first ten cases. Ann Surg 1955; 142 (3) 418-442
- 16 Gott VL, Shumway NE. Cross-circulation: a milestone in cardiac surgery. J Thorac Cardiovasc Surg 2004; 127 (3) 617-618
- 17 Moller JH, Shumway SJ, Gott VL. The first open-heart repairs using extracorporeal circulation by cross-circulation: a 53-year follow-up. Ann Thorac Surg 2009; 88 (3) 1044-1046
- 18 Gott VL. Lillehei, Lewis, and Wangensteen: the right mix for giant achievements in cardiac surgery. Ann Thorac Surg 2005; 79 (6) S2210-S2213
Address for correspondence
-
References
- 1 Jeger E. Die Chirurgie der Blutgefässe und des Herzens. Berlin: August Hirschwald; 1913
- 2 Rodewald G, History of extracorporeal circulation. In: Hagl S, Klövekorn WP, Mayr N, Sebening F. , eds. Proceedings of the Symposium Thirty Years of Extracorporeal Circulation; April 5–7; 1984: 25-43 ; Munich, Germany: Dtsch Herzzentrum München
- 3 Gibbon Jr JH. The gestation and birth of an idea. Phila Med 1963; 59: 913
- 4 Shumacker Jr HB. John Heysham Gibbon Jr September 29, 1903–February 5, 1973. Biographical Memoirs. Vol 53. Washington DC: National Academy Press; 1982: 213-247
- 5 Hill JD, Gibbon John Jr H. Part I. The development of the first successful heart-lung machine. Ann Thorac Surg 1982; 34 (3) 337-341
- 6 Dobell ARC, Gibbon John Jr H. Part II. Personal reminiscences. Ann Thorac Surg 1982; 34 (3) 342-344
- 7 Gibbon Jr JH. Artificial maintenance of circulation during experimental occlusion of pulmonary artery. Arch Surg 1937; 34: 1105-1131
- 8 Shumacker Jr HB, A Dream of the Heart. The life of John H. Gibbon Jr. , Father of the Heart-Lung Machine. Santa Barbara: Fithian Press; 1999
- 9 Zenker R. Zur Geschichte und Entwicklung der Herzchirurgie. , in: Herz und herznahe Gefäße. Berlin, Heidelberg, New York: Springer-Verlag; 1978. : S. 1-14
- 10 Miller GW. King of Hearts: The True Story of the Maverick Who pioneered Open Heart Surgery. New York: Crown Publishers; 2000
- 11 Gibbon Jr JH. Application of a mechanical heart and lung apparatus to cardiac surgery. Minn Med 1954; 37 (3) 171-185 , passim
- 12 Lillehei CW. A personalized history of extracorporeal circulation. Trans Am Soc Artif Intern Organs 1982; 28: 5-16
- 13 Lillehei CW, Cohen M, Warden HE, Ziegler NR, Varco RL. The results of direct vision closure of ventricular septal defects in eight patients by means of controlled cross circulation. Surg Gynecol Obstet 1955; 101 (4) 446-466
- 14 Lillehei CW, Cohen M, Warden HE, Varco RL. The direct-vision intracardiac correction of congenital anomalies by controlled cross circulation; results in thirty-two patients with ventricular septal defects, tetralogy of Fallot, and atrioventricularis communis defects. Surgery 1955; 38 (1) 11-29
- 15 Lillehei CW, Cohen M, Warden HE , et al. Direct vision intracardiac surgical correction of the tetralogy of Fallot, pentalogy of Fallot, and pulmonary atresia defects; report of first ten cases. Ann Surg 1955; 142 (3) 418-442
- 16 Gott VL, Shumway NE. Cross-circulation: a milestone in cardiac surgery. J Thorac Cardiovasc Surg 2004; 127 (3) 617-618
- 17 Moller JH, Shumway SJ, Gott VL. The first open-heart repairs using extracorporeal circulation by cross-circulation: a 53-year follow-up. Ann Thorac Surg 2009; 88 (3) 1044-1046
- 18 Gott VL. Lillehei, Lewis, and Wangensteen: the right mix for giant achievements in cardiac surgery. Ann Thorac Surg 2005; 79 (6) S2210-S2213