

Subscribe to RSS
DOI: 10.1055/s-0029-1244062
© Georg Thieme Verlag KG Stuttgart · New York
Chronic pancreatitis and cholangitis caused by absence of the duodenal papilla
Z.-S. LiMD
Department of Gastroenterology
Changhai Hospital
The Second Military Medical University
168 Changhai Road
Shanghai
China
Fax: +86-21-55620081
Email: zhaoshenli@hotmail.com
Publication History
Publication Date:
07 October 2010 (online)

Anatomic abnormalities associated with the opening of the pancreas and biliary systems into the upper gastrointestinal tract have been increasingly recognized since endoscopic retrograde cholangiopancreatography (ERCP) has come into wide use in clinical practice [1].
A 38-year-old Chinese woman presented with a 4-month history of dull abdominal pain. She had no history of endoscopic intervention (e. g., ERCP or sphincterotomy) or surgery. Physical examination revealed mild abdominal tenderness in the right upper quadrant. Serum levels of triglycerides, calcium, carcinoembryonic antigen, and amylase were normal. Serum carbohydrate antigen 19 – 9 was moderately elevated (202.60 U/mL, reference value: 0 – 37 U/mL). Computed tomography (CT) of the abdomen revealed diffuse pneumatosis of the intrahepatic ([Fig. 1]) and common bile ducts. CT also found dilatation of the pancreatic duct and a high-density shadow in the head of the pancreas ([Fig. 2]). Magnetic resonance cholangiopancreatography showed dilatation of the pancreatic duct and bile duct ([Fig. 3]). ERCP was performed to clear the main pancreatic duct. During the procedure, it became evident that the major duodenal papilla of the patient was absent. Instead, there were two orifices ([Fig. 4]), one on the right for the pancreatic duct and one on the left for the common bile duct. They were subsequently visualized by cholangiopancreatography. The bile duct was irregularly dilated and contrast emptying was delayed ([Fig. 5]). ERCP also revealed a dilated, tortuous main pancreatic duct containing stones ([Fig. 6]).

Fig. 1 Diffuse pneumatosis of the intrahepatic bile ducts.

Fig. 2 CT revealed dilatation of the pancreatic duct and a high-density shadow in the head of pancreas, which could be calcification of the pancreas or stones in the pancreatic duct.

Fig. 3 Magnetic resonance cholangiopancreatography showed dilatation of the pancreatic duct and bile duct.
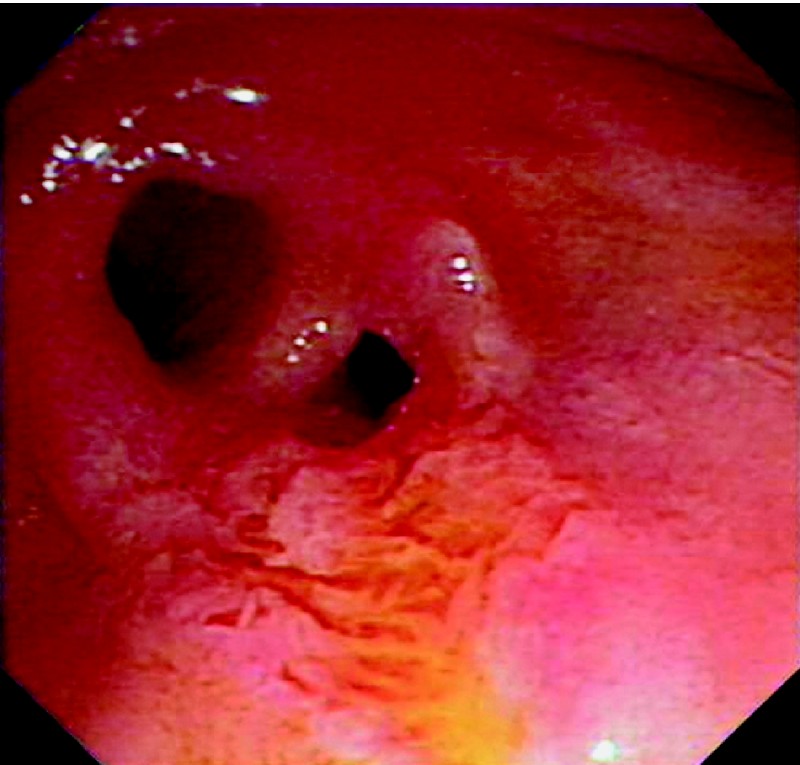
Fig. 4 The major duodenal papilla was absent. Instead, there were two orifices: the one on the right is for the pancreatic duct and the one on the left is for common bile duct.

Fig. 5 Endoscopic retrograde cholangiopancreatography (ERCP) showed the bile duct to be irregularly dilated.

Fig. 6 ERCP revealed a dilated, tortuous main pancreatic duct containing stones.
The etiology of this anomalous opening is unknown. In patients with this defect, duodenal content could easily pass through the biliary tract and pancreatic duct (duodenobiliary reflux). It has been reported that after endoscopic sphincterotomy – which is essentially an artificial opening defect – the occurrence of cholangitis is generally about 3 % [2] [3]. Chronic pancreatitis is a very rare complication after sphincterotomy [4] [5]. Long-term absence of the duodenal papilla can lead to chronic pancreatitis and cholangitis.
Competing interests: None
Endoscopy_UCTN_Code_CCL_1AZ_2AK
Endoscopy_UCTN_Code_CCL_1AZ_2AL
References
- 1 Disibeyaz S, Parlak E, Cicek B. et al . Anomalous opening of the common bile duct into the duodenal bulb: endoscopic treatment. BMC Gastroenterol. 2007; 7 26-36
- 2 Gregg J A, Girolami P D, Carr-Locke D L. Effects of sphincterotomy and endoscopic sphincterotomy on the bacteriologic characteristics of the common bile duct. Am J Surg. 1985; 149 668-671
- 3 Feretis C B, Contou C T, Manouras A J. et al . Long-term consequences of bacterial colonization of the biliary tract after choledochostomy. Surg Gynecol Obstet. 1984; 159 363-266
- 4 Sugiyama M, Atomi Y. Risk factors predictive of late complications after endoscopic sphincterotomy for bile duct stones: long-term (more than 10 years) follow-up study. Am J Gastroenterol. 2002; 97 2763-2767
- 5 Wojtun S, Gil J, Gietka W. et al . Endoscopic sphincterotomy for choledocholithiasis: a prospective single-center study on the short-term and long-term treatment results in 483 patients. Endoscopy. 1997; 29 258-265
1 Dr. Hu LH and Dr. Liao Z contributed equally to this work.
Z.-S. LiMD
Department of Gastroenterology
Changhai Hospital
The Second Military Medical University
168 Changhai Road
Shanghai
China
Fax: +86-21-55620081
Email: zhaoshenli@hotmail.com
References
- 1 Disibeyaz S, Parlak E, Cicek B. et al . Anomalous opening of the common bile duct into the duodenal bulb: endoscopic treatment. BMC Gastroenterol. 2007; 7 26-36
- 2 Gregg J A, Girolami P D, Carr-Locke D L. Effects of sphincterotomy and endoscopic sphincterotomy on the bacteriologic characteristics of the common bile duct. Am J Surg. 1985; 149 668-671
- 3 Feretis C B, Contou C T, Manouras A J. et al . Long-term consequences of bacterial colonization of the biliary tract after choledochostomy. Surg Gynecol Obstet. 1984; 159 363-266
- 4 Sugiyama M, Atomi Y. Risk factors predictive of late complications after endoscopic sphincterotomy for bile duct stones: long-term (more than 10 years) follow-up study. Am J Gastroenterol. 2002; 97 2763-2767
- 5 Wojtun S, Gil J, Gietka W. et al . Endoscopic sphincterotomy for choledocholithiasis: a prospective single-center study on the short-term and long-term treatment results in 483 patients. Endoscopy. 1997; 29 258-265
1 Dr. Hu LH and Dr. Liao Z contributed equally to this work.
Z.-S. LiMD
Department of Gastroenterology
Changhai Hospital
The Second Military Medical University
168 Changhai Road
Shanghai
China
Fax: +86-21-55620081
Email: zhaoshenli@hotmail.com
Fig. 1 Diffuse pneumatosis of the intrahepatic bile ducts.
Fig. 2 CT revealed dilatation of the pancreatic duct and a high-density shadow in the head of pancreas, which could be calcification of the pancreas or stones in the pancreatic duct.
Fig. 3 Magnetic resonance cholangiopancreatography showed dilatation of the pancreatic duct and bile duct.
Fig. 4 The major duodenal papilla was absent. Instead, there were two orifices: the one on the right is for the pancreatic duct and the one on the left is for common bile duct.
Fig. 5 Endoscopic retrograde cholangiopancreatography (ERCP) showed the bile duct to be irregularly dilated.
Fig. 6 ERCP revealed a dilated, tortuous main pancreatic duct containing stones.