

Subscribe to RSS
DOI: 10.1055/a-2620-3297
The Preoperative Planning, Design, and Execution of the Freestyle Propeller Flap: A Detailed Description and the Case Series
Authors
Abstract
Background
Propeller flap reconstruction has been widely utilized in soft tissue reconstruction due to its versatility and aesthetic outcomes. However, technical challenges and the risk of complications persist. This study aims to provide detailed guidelines on the preoperative planning, intraoperative considerations, and execution of propeller flap surgery to reduce complications.
Methods
A retrospective review was conducted on 20 consecutive patients undergoing propeller flap reconstruction between January 2018 and December 2020. Preoperative planning involved computed tomography (CT) angiography and color Doppler ultrasound. Flap designs prioritized perforator proximity (<3 cm from the defect), vessel axiality, and tissue laxity assessed by skin pinch tests. Surgical techniques including pedicle skeletonization, flap elevation, rotation, and inset were meticulously followed.
Results
No total flap loss occurred. Partial flap loss was observed in one case (5%). Two flaps (10%) exhibited venous congestion, which resolved following leech therapy without necrosis. Defects were predominantly located on the trunk (80%), with malignancy as the primary cause (55%). Mean follow-up duration was 432 days.
Conclusions
Careful preoperative planning and adherence to meticulous surgical techniques can significantly reduce complications in propeller flap reconstruction. This structured approach offers a reliable framework, particularly beneficial for surgeons less familiar with propeller flap techniques.
Introduction
Propeller flap reconstructions have been performed in various body areas with adequate perforators for soft tissue reconstruction.[1] [2] [3] [4] The major advantages of the propeller flap include less pedicle dissection during flap elevation, faster operation times, no need for microsurgery, and superior aesthetic results.[5] [6] [7] [8] [9] [10] As long as the surrounding tissue is preserved, the propeller flaps can be considered for covering the soft tissue defect.
Despite their increasing versatility and reliability, performing propeller flap reconstruction without complications is challenging due to various obstacles.[11] [12] [13] [14] One of the most common reasons for failure in a propeller flap is inappropriate indication. Even though the concepts and fundamental principles have been reported, propeller flaps are often attempted in cases that are not ideal.[10] [11] In addition to inappropriate indications, errors and mistakes in the surgical procedures at each step can result in complications such as arterial and venous insufficiency and flap failure.
This article describes the technical details of designing and performing propeller flap reconstructions, including preoperative, intraoperative, and surgical considerations. A retrospective review of propeller flaps has been conducted, and cases of propeller flaps are presented. This article will be beneficial for young surgeons who are not familiar with propeller flaps.
Methods
This retrospective study, approved by the Institutional Review Board (No. 2025-0099), involved 20 consecutive patients who underwent propeller flap reconstruction between January 2018 and December 2020 at a single center. Demographic data, flap information, and reconstructive outcome data were collected. Written informed consent was obtained from all patients for the publication of their clinical photographs.
Step-by-Step Approach of the Propeller Flap
The video provides a step-by-step summary of the propeller flap procedure ([Video 1]).
Video 1A step-by-step approach to propeller flap reconstruction.Preoperative Planning Using Computed Tomography Angiography and Color Doppler Ultrasound
The authors used computed tomography (CT) angiography and color Doppler ultrasound for preoperative evaluation. CT angiography can identify a suitable perforator around the defect. Color Doppler ultrasound, with its real-time imaging, can directly mark the vessels and provide hemodynamic data, including flow velocity, vessel diameter, and the axis of the perforator course.[15] [16] [17] [18] [19] For the propeller flap, the intraflap perforator course (axis) is crucial for designing the flap to maximize circulation. High-frequency color Doppler ultrasound can easily identify and preoperatively mark the perforator axis.[18]
Perforator Identification and Considerations in Flap Design
Using proper retractors, perforators were dissected above the deep fascia and identified directly from the margin of the defect. An additional incision is not usually needed if a handheld Doppler is used to identify the perforators. The authors then chose the perforator with good blood flow, one <3 cm from the defect, and one near the tip of the defect. If the perforator is 1 cm away from the margin, the flap length is increased to twice as long as 2 cm ([Fig. 1]). A perforator closer to the tip than the side is advantageous for effectively covering the defect ([Fig. 2]). For the flap size, a flap margin over 10 cm from the perforator may result in partial necrosis.[20] When determining the axis of the flap, the axis of the perforator course and tissue laxity should be considered. Good axiality of the perforator can provide more blood supply to the area most distant from the perforator, minimizing partial necrosis of the flap. Skin laxity is considered when determining not only the flap direction but also the flap width for primary donor site closure. Skin laxity is evaluated by a skin pinch test ([Fig. 3]). Flap design should comprehensively consider the perforator position, its relation with the tip position, perforator to margin distance, and the axis of the flap.



Considerations in Locating the Perforator in the Propeller Flap
When designing propeller flaps, the question arises of where to position the perforators. Typically, the perforator is placed in the middle and distal part of the flap. However, it is not always necessary to place it in the middle. More importantly, the flap should be designed to fill all defects when rotated. Sometimes, it may be more advantageous to place the perforator on one side to cover the defect, as shown in [Fig. 4].

Flap Elevation and Pedicle Skeletonization
After designing the flap, flap elevation is performed from the flap's margin. About 2 cm of pedicle skeletonization is generally sufficient for rotation. If the pedicle source is directed toward the defect, pedicle skeletonization can effectively elongate the pedicle length. If the origin of the pedicle source is directed away from the defect, pedicle skeletonization has minimal effect on elongating the pedicle length ([Fig. 5]).

Flap Inset and Rotation
After flap elevation, rotation and flap inset are performed. Rotation is done in a direction less than 180 degrees, and the state of the pedicle is evaluated. Flap perfusion should be assessed after rotation, and two things must be checked to determine if perfusion is inadequate. First, evaluate whether excessive tension is on the flap and perform the inset again. Second, after rotating in the opposite direction, reassess perfusion. A hemodynamic study using color duplex ultrasound can help determine the direction of rotation (clockwise or counterclockwise).[21]
Considerations in Arterial and Venous Insufficiency after Flap Inset
After inset, immediate arterial or venous insufficiency can occur. Careful checking of the pedicle vessels is necessary. If pedicle compromise includes kinking, compression, or stretching, the surgeon should identify the reasons for the compromise and reduce the mechanical burdens on the pedicle vein. If venous congestion is limited to the flap margin, leeches can be applied, and partial congestion may resolve after a few days. If venous congestion persists despite efforts to reduce pedicle compromise, delayed flap inset should be considered. Delayed flap inset involves returning the propeller flap to the original donor site and reinserting it after 1 to 2 weeks. This procedure is based on the “delay phenomenon” of the flap.[22]
Results
The mean patient age was 52.8 years, with a mean follow-up period of 432 days. The defect was primarily located on the trunk (80%) and lower extremities (20%). The cause of the defect was malignancy in 55% of patients and pressure sores in 45% ([Table 1]). The mean pedicle distance from the margin was 2.4 cm (range, 1–4 cm). There was no total flap loss. The partial flap loss rate was 5% (n = 1). Two flaps (10%) experienced venous congestion without partial necrosis after leech application ([Table 2]).
Abbreviations: DM, diabetes mellitus; HTN, hypertension.
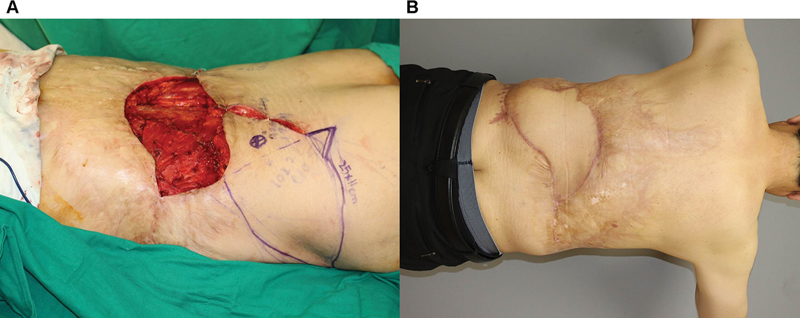
Representative case examples are shown. [Figure 6] shows a 64-year-old male patient with Marjolin's ulceration on his back ([Fig. 6A]). A 25 × 10 cm propeller flap based on the axiality of the perforator and skin laxity was designed and elevated. At 12 months, the patient had a good contour of the flap without complications ([Fig. 6B]). [Figure 7] shows a 44-year-old male patient with myxofibrosarcoma on his left thigh ([Fig. 7A]). A 15 × 7 cm propeller flap based on the axiality of the perforator and skin laxity was designed and elevated. At 1 month, the patient had a good contour of the flap without complications ([Fig. 7B]). [Figure 8] shows a 43-year-old female patient with dermatofibrosarcoma protuberance in her left upper back. A 12 × 11.5 cm defect was created after a wide excision ([Fig. 8A]). An 18 × 6 cm propeller flap based on the axiality of the perforator was designed ([Fig. 8B]). An arterial supercharge was performed to increase blood flow to the distal area ([Fig. 8C]). At 1 year, the patient had a good contour of the flap without complications, even after radiation therapy ([Fig. 8D]). [Figure 9] presents a 56-year-old male patient with chronic osteomyelitis on his left lower leg after below knee amputation ([Fig. 9A]). A 9 × 6 cm propeller flap was designed to cover a 5 × 6 cm defect on the anterior leg ([Fig. 9B–] [9D]). Adequate perfusion of the flap after elevation was confirmed with ICG angiography ([Fig. 9E]).



Discussion
By understanding the anatomical knowledge of the perforasome, propeller flap surgery can theoretically be used in various parts of the body in different ways.[23] [24] [25] To achieve successful reconstruction, surgeons must understand the surgical details to focus on during planning, designing, and postoperative management. However, few articles describe the surgical details of performing the propeller flap.
This article emphasizes the surgical details of performing the propeller flap. Designing and planning the flap before surgery is crucial because the propeller flap features a perforator that is positioned laterally and rotated. If surgeons do not pay attention to each step, complications such as partial necrosis, venous congestion, and incomplete coverage of the defect are likely.
The propeller flap does not have a specific indication but is an excellent reconstructive option when certain conditions outlined in the text are met. First, an appropriate perforator within 3 cm of the defect must be evaluated and confirmed through imaging modalities such as CT angiography or color Doppler ultrasound. Additionally, the donor site must be assessed using a pinching test to ensure sufficient surrounding tissue is available for transfer. A comprehensive evaluation is essential to determine whether the propeller flap is optimal. If deemed unsuitable, alternative reconstructive options should be considered before proceeding with surgery.
The major complications associated with the propeller flap are arterial insufficiency, venous congestion, and partial or total necrosis of the flap. Among these, venous congestion is generally believed to be the most common complication in propeller flap surgery, occurring in 5 to 11% of cases.[26] Given that veins have thinner and more pliable walls than arteries, venous congestion is more easily related to pedicle compromise, including compression, kinking, and stretching. Care should be taken during pedicle dissection to avoid damaging the veins and to check the pedicle vein for any compression, kinking, or stretching.
Venous congestion management varies depending on its timing. If congestion arises immediately after flap elevation, supercharging should be attempted to enhance venous outflow. If unsuccessful, leech therapy and systemic heparinization may be employed. In cases where congestion occurs after flap rotation, additional pedicle dissection should be performed to identify and correct kinking or excessive stretching. If these measures fail, the flap can be derotated and temporarily returned to the donor site, with re-insetting attempted approximately 5 days later. This approach leverages the delayed phenomenon, which improves flap perfusion through angiogenesis and vascular adaptation.
Partial flap necrosis is another frequent complication in propeller flaps.[11] [13] [27] To reduce partial flap necrosis, one of the most challenging considerations in designing the propeller flap is determining the location of the perforator from the flap margin. The authors described a perforator less than 3 cm from the defect and a perforator near the tip of the defect. However, the possibility of partial necrosis increases if the perforator is too close to the flap margin and far from the distal area. According to a large-volume report on partial necrosis of the perforator flap, a distance of 10.25 cm from the perforator significantly increases the possibility of partial necrosis.[20] Partial necrosis of the propeller flap usually occurs in the most distal area, which is crucial for covering the defect. Surgeons should consider this point when designing large propeller flaps. ICG angiography after harvesting the flap can help predict the occurrence of partial necrosis.[28]
Another consideration in the propeller flap is radiation after cancer resection. The biggest difference between the free flap and the propeller flap in the reconstruction of sarcoma resection is that the resection margin may move away from its original position during flap rotation by as much as 7 to 8 cm from the original tumor margin.[29] Although there is a report that there were no significant differences in disease-free survival between patients who underwent propeller flap reconstruction and those who underwent free flap reconstruction, a multidisciplinary approach and discussion are needed to determine the accurate planning target volume of adjuvant radiotherapy.
There are several limitations in this study. First, it is designed as a retrospective study, not a prospective one. Second, the sample size is relatively small. However, this article aims to describe the surgical details and share cases of the propeller flap.
Conclusion
In this article, we described the proper planning and technical details. Preoperative planning and proper design are crucial in reducing complications and ensuring successful surgery. This article will be beneficial for surgeons who are not familiar with propeller flaps.
Conflict of Interest
J.P.H. and H.P.S. are editorial board members of the journal but were not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Authors' Contributions
H.P.S. and H.B.K. conceptualized the study. H.B.K. and S.J.H. conducted the literature review and data extraction. All authors contributed to the interpretation of results and manuscript writing. All authors reviewed and approved the final manuscript.
Ethical Approval
This retrospective study, approved by the Institutional Review Board (No. 2025-0099).
Patient Consent
Written informed consent was obtained from all patients for the publication of their clinical photographs.
-
References
- 1 Hyakusoku H, Yamamoto T, Fumiiri M. The propeller flap method. Br J Plast Surg 1991; 44 (01) 53-54
- 2 Kedar DJ, Pak CJ, Suh HP, Hong JP. Propeller flaps in the posterior trunk. Semin Plast Surg 2020; 34 (03) 176-183
- 3 Pignatti M, Pinto V, Docherty Skogh AC. et al. How to design and harvest a propeller flap. Semin Plast Surg 2020; 34 (03) 152-160
- 4 Ellabban MA, Awad AI, Hallock GG. Perforator-pedicled propeller flaps for lower extremity reconstruction. Semin Plast Surg 2020; 34 (03) 200-206
- 5 Cordova A, D'Arpa S, Rosatti F. et al. Propeller flaps in the head and neck. Semin Plast Surg 2020; 34 (03) 165-170
- 6 D'Arpa S, Toia F, Pirrello R, Moschella F, Cordova A. Propeller flaps: a review of indications, technique, and results. BioMed Res Int 2014; 2014: 986829
- 7 D'Arpa S, Cordova A, Pignatti M, Moschella F. Freestyle pedicled perforator flaps: safety, prevention of complications, and management based on 85 consecutive cases. Plast Reconstr Surg 2011; 128 (04) 892-906
- 8 Hyakusoku H, Ono S. The history of propeller flaps. Semin Plast Surg 2020; 34 (03) 133-138
- 9 Teo TC. Propeller flaps for reconstruction around the foot and ankle. J Reconstr Microsurg 2021; 37 (01) 22-31
- 10 Lazzeri D, Huemer GM, Nicoli F. et al. Indications, outcomes, and complications of pedicled propeller perforator flaps for upper body defects: a systematic review. Arch Plast Surg 2013; 40 (01) 44-50
- 11 Cajozzo M, Jiga LP, Jandali Z. et al. Complications and solutions in propeller flap surgery. Semin Plast Surg 2020; 34 (03) 210-220
- 12 Gir P, Cheng A, Oni G, Mojallal A, Saint-Cyr M. Pedicled-perforator (propeller) flaps in lower extremity defects: a systematic review. J Reconstr Microsurg 2012; 28 (09) 595-601
- 13 Paik JM, Pyon JK. Risk factor analysis of freestyle propeller flaps. J Reconstr Microsurg 2017; 33 (01) 26-31
- 14 Georgescu AV. Propeller perforator flaps in distal lower leg: evolution and clinical applications. Arch Plast Surg 2012; 39 (02) 94-105
- 15 Hong JP, Hur J, Kim HB, Park CJ, Suh HP. The use of color duplex ultrasound for local perforator flaps in the extremity. J Reconstr Microsurg 2022; 38 (03) 233-237
- 16 Hallock GG. Doppler sonography and color duplex imaging for planning a perforator flap. Clin Plast Surg 2003; 30 (03) 347-357 , v–vi
- 17 Moore R, Mullner D, Nichols G, Scomacao I, Herrera F. Color Doppler ultrasound versus computed tomography angiography for preoperative anterolateral thigh flap perforator imaging: a systematic review and meta-analysis. J Reconstr Microsurg 2022; 38 (07) 563-570
- 18 Lee JW, Kim HK, Kim SR, Han YS, Park JH. Preoperative identification of a perforator using computed tomography angiography and metal clip marking in perforator flap reconstruction. Arch Plast Surg 2015; 42 (01) 78-83
- 19 Visconti G, Bianchi A, Hayashi A. et al. Thin and superthin perforator flap elevation based on preoperative planning with ultrahigh-frequency ultrasound. Arch Plast Surg 2020; 47 (04) 365-370
- 20 Min K, Hong JP, Suh HP. Risk factors for partial flap loss in a free flap: a 12-year retrospective study of anterolateral thigh free flaps in 303 lower extremity cases. Plast Reconstr Surg 2022; 150 (05) 1071e-1081e
- 21 Song S, Jeong HH, Lee Y. et al. Direction of flap rotation in propeller flaps: does it really matter?. J Reconstr Microsurg 2019; 35 (08) 549-556
- 22 Ozgentaş HE, Shenaq S, Spira M. Study of the delay phenomenon in the rat TRAM flap model. Plast Reconstr Surg 1994; 94 (07) 1018-1024 , discussion 1025–1026
- 23 Wallace CG, Kao HK, Jeng SF, Wei FC. Free-style flaps: a further step forward for perforator flap surgery. Plast Reconstr Surg 2009; 124 (06) e419-e426
- 24 Nelson JA, Fischer JP, Brazio PS, Kovach SJ, Rosson GD, Rad AN. A review of propeller flaps for distal lower extremity soft tissue reconstruction: Is flap loss too high?. Microsurgery 2013; 33 (07) 578-586
- 25 Mohan AT, Sur YJ, Zhu L. et al. The concepts of propeller, perforator, keystone, and other local flaps and their role in the evolution of reconstruction. Plast Reconstr Surg 2016; 138 (04) 710e-729e
- 26 Sisti A, D'Aniello C, Fortezza L. et al. Propeller flaps: a literature review. In Vivo 2016; 30 (04) 351-373
- 27 Innocenti M, Menichini G, Baldrighi C, Delcroix L, Vignini L, Tos P. Are there risk factors for complications of perforator-based propeller flaps for lower-extremity reconstruction?. Clin Orthop Relat Res 2014; 472 (07) 2276-2286
- 28 Burnier P, Niddam J, Bosc R, Hersant B, Meningaud JP. Indocyanine green applications in plastic surgery: A review of the literature. J Plast Reconstr Aesthet Surg 2017; 70 (06) 814-827
- 29 Cha HG, Kang MK, Kim W, Lee JS, Hong JP, Suh HP. Oncologic safety of propeller flap and free flap in reconstruction after soft tissue sarcoma resection. J Surg Oncol 2020; 122 (04) 787-794
Address for correspondence
Publication History
Received: 06 October 2024
Accepted: 16 April 2025
Accepted Manuscript online:
26 May 2025
Article published online:
23 July 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Hyakusoku H, Yamamoto T, Fumiiri M. The propeller flap method. Br J Plast Surg 1991; 44 (01) 53-54
- 2 Kedar DJ, Pak CJ, Suh HP, Hong JP. Propeller flaps in the posterior trunk. Semin Plast Surg 2020; 34 (03) 176-183
- 3 Pignatti M, Pinto V, Docherty Skogh AC. et al. How to design and harvest a propeller flap. Semin Plast Surg 2020; 34 (03) 152-160
- 4 Ellabban MA, Awad AI, Hallock GG. Perforator-pedicled propeller flaps for lower extremity reconstruction. Semin Plast Surg 2020; 34 (03) 200-206
- 5 Cordova A, D'Arpa S, Rosatti F. et al. Propeller flaps in the head and neck. Semin Plast Surg 2020; 34 (03) 165-170
- 6 D'Arpa S, Toia F, Pirrello R, Moschella F, Cordova A. Propeller flaps: a review of indications, technique, and results. BioMed Res Int 2014; 2014: 986829
- 7 D'Arpa S, Cordova A, Pignatti M, Moschella F. Freestyle pedicled perforator flaps: safety, prevention of complications, and management based on 85 consecutive cases. Plast Reconstr Surg 2011; 128 (04) 892-906
- 8 Hyakusoku H, Ono S. The history of propeller flaps. Semin Plast Surg 2020; 34 (03) 133-138
- 9 Teo TC. Propeller flaps for reconstruction around the foot and ankle. J Reconstr Microsurg 2021; 37 (01) 22-31
- 10 Lazzeri D, Huemer GM, Nicoli F. et al. Indications, outcomes, and complications of pedicled propeller perforator flaps for upper body defects: a systematic review. Arch Plast Surg 2013; 40 (01) 44-50
- 11 Cajozzo M, Jiga LP, Jandali Z. et al. Complications and solutions in propeller flap surgery. Semin Plast Surg 2020; 34 (03) 210-220
- 12 Gir P, Cheng A, Oni G, Mojallal A, Saint-Cyr M. Pedicled-perforator (propeller) flaps in lower extremity defects: a systematic review. J Reconstr Microsurg 2012; 28 (09) 595-601
- 13 Paik JM, Pyon JK. Risk factor analysis of freestyle propeller flaps. J Reconstr Microsurg 2017; 33 (01) 26-31
- 14 Georgescu AV. Propeller perforator flaps in distal lower leg: evolution and clinical applications. Arch Plast Surg 2012; 39 (02) 94-105
- 15 Hong JP, Hur J, Kim HB, Park CJ, Suh HP. The use of color duplex ultrasound for local perforator flaps in the extremity. J Reconstr Microsurg 2022; 38 (03) 233-237
- 16 Hallock GG. Doppler sonography and color duplex imaging for planning a perforator flap. Clin Plast Surg 2003; 30 (03) 347-357 , v–vi
- 17 Moore R, Mullner D, Nichols G, Scomacao I, Herrera F. Color Doppler ultrasound versus computed tomography angiography for preoperative anterolateral thigh flap perforator imaging: a systematic review and meta-analysis. J Reconstr Microsurg 2022; 38 (07) 563-570
- 18 Lee JW, Kim HK, Kim SR, Han YS, Park JH. Preoperative identification of a perforator using computed tomography angiography and metal clip marking in perforator flap reconstruction. Arch Plast Surg 2015; 42 (01) 78-83
- 19 Visconti G, Bianchi A, Hayashi A. et al. Thin and superthin perforator flap elevation based on preoperative planning with ultrahigh-frequency ultrasound. Arch Plast Surg 2020; 47 (04) 365-370
- 20 Min K, Hong JP, Suh HP. Risk factors for partial flap loss in a free flap: a 12-year retrospective study of anterolateral thigh free flaps in 303 lower extremity cases. Plast Reconstr Surg 2022; 150 (05) 1071e-1081e
- 21 Song S, Jeong HH, Lee Y. et al. Direction of flap rotation in propeller flaps: does it really matter?. J Reconstr Microsurg 2019; 35 (08) 549-556
- 22 Ozgentaş HE, Shenaq S, Spira M. Study of the delay phenomenon in the rat TRAM flap model. Plast Reconstr Surg 1994; 94 (07) 1018-1024 , discussion 1025–1026
- 23 Wallace CG, Kao HK, Jeng SF, Wei FC. Free-style flaps: a further step forward for perforator flap surgery. Plast Reconstr Surg 2009; 124 (06) e419-e426
- 24 Nelson JA, Fischer JP, Brazio PS, Kovach SJ, Rosson GD, Rad AN. A review of propeller flaps for distal lower extremity soft tissue reconstruction: Is flap loss too high?. Microsurgery 2013; 33 (07) 578-586
- 25 Mohan AT, Sur YJ, Zhu L. et al. The concepts of propeller, perforator, keystone, and other local flaps and their role in the evolution of reconstruction. Plast Reconstr Surg 2016; 138 (04) 710e-729e
- 26 Sisti A, D'Aniello C, Fortezza L. et al. Propeller flaps: a literature review. In Vivo 2016; 30 (04) 351-373
- 27 Innocenti M, Menichini G, Baldrighi C, Delcroix L, Vignini L, Tos P. Are there risk factors for complications of perforator-based propeller flaps for lower-extremity reconstruction?. Clin Orthop Relat Res 2014; 472 (07) 2276-2286
- 28 Burnier P, Niddam J, Bosc R, Hersant B, Meningaud JP. Indocyanine green applications in plastic surgery: A review of the literature. J Plast Reconstr Aesthet Surg 2017; 70 (06) 814-827
- 29 Cha HG, Kang MK, Kim W, Lee JS, Hong JP, Suh HP. Oncologic safety of propeller flap and free flap in reconstruction after soft tissue sarcoma resection. J Surg Oncol 2020; 122 (04) 787-794