

Subscribe to RSS
DOI: 10.1055/a-2566-9262
Trends in Invasive Prenatal Testing, Diagnosis, and Abortion for Fetal Aneuploidy
Authors

Abstract
Objective
We aimed to assess trends in prenatal testing for aneuploidy, including indications, diagnostic yield, and the timing of diagnosis and abortions since the introduction of cell-free DNA (cfDNA) into routine prenatal care.
Study Design
In this observational retrospective study, all invasive prenatal diagnostic procedures performed at a single institution from 2010 to 2022 were evaluated. Clinical variables included gestational age (GA) at testing, indications, results, and pregnancy outcomes (continuation or abortion). Description statistics were used to characterize the sample.
Results
A total of 1,262 diagnostic procedures were performed during the study period, with 20.5% (n = 258) confirming genetic abnormalities. Amniocentesis accounted for 70.4% (n = 888) of diagnostic procedures, while 29.6% underwent chorionic villus sampling (CVS; n = 374). The number of procedures decreased significantly over time (p < 0.001). Indications for testing shifted dramatically; testing for the indication of advanced maternal age alone fell from 45 to 5.6% (p < 0.001). Patients with abnormal cfDNA screening results underwent diagnostic testing at an earlier average gestational age (15.3 vs. 17.8 weeks; p < 0.001), had a higher likelihood of undergoing CVS (30.7 vs. 8.9%; p < 0.001), and had higher rates of abnormal cytogenetics (60.4 vs. 13.2%; p < 0.001) compared to patients with analyte testing. Patients diagnosed with aneuploidy following abnormal cfDNA underwent abortion at earlier GA (15.5 vs.19.3 weeks; p = 0.002).
Conclusion
cfDNA screening has reduced prenatal invasive diagnostic procedures and shifted testing indications. Abnormal cfDNA screening is associated with a higher diagnostic yield and earlier GA at diagnosis and abortion after confirmation of aneuploidy. Despite these advances, aneuploidy diagnosis continues to extend into the second trimester, highlighting ongoing challenges in early detection.
Key Points
-
The introduction of cfDNA has reduced rates of invasive diagnostic procedures, shifting the most frequent indications for testing from advanced maternal age to abnormal ultrasound findings.
-
Despite the use of cfDNA screening at earlier gestational ages compared with traditional analyte testing, the gestational age at which diagnostic procedures and abortions are performed for fetal aneuploidy has remained in the second trimester.
-
Although cfDNA testing leads to earlier and more frequent identification of aneuploidy, confirmation of abnormal results often occurs after gestational age thresholds for abortion in many states.
Keywords
fetal aneuploidy - CVS - amniocentesis - prenatal diagnosis - abortion - prenatal screeningApproximately 5 to 10% of pregnancies are affected by chromosomal abnormalities.[1] [2] The landscape of prenatal genetic screening and diagnosis experienced a transformative shift in 2011 with the advent of maternal cell-free DNA (cfDNA) screening for fetal aneuploidy.[3] Subsequently, cfDNA has rapidly replaced maternal serum analyte testing due to its higher detection rates, reduced false positive rates, earlier availability in pregnancy, and ease of acquisition.[4] [5]
Prior studies have demonstrated that advances in cfDNA screening and ultrasound have led to decreased rates of invasive prenatal diagnostic testing, which include chorionic villus sampling (CVS) and amniocentesis.[3] [6] [7] [8] Despite advances in screening, the American College of Obstetricians and Gynecologists and the American College of Medical Genetics recommend that prenatal diagnostic testing should be discussed and offered to all patients regardless of maternal age or risk of chromosomal abnormality, or following a positive screening result for suspected fetal aneuploidy.[1]
The rise of the availability of first-trimester cfDNA testing has occurred simultaneously with the rapid proliferation of abortion restrictions across the United States. It is important to understand how this evolution in prenatal screening practices has changed the healthcare landscape. We sought to evaluate trends and indications for invasive prenatal testing, diagnosis, and abortion for fetal aneuploidy over a 12-year period since the introduction of cfDNA screening, in an era with significant legal restrictions.
Materials and Methods
In this retrospective study, we identified patients who had amniocentesis or CVS from January 2010 to December 2022 at a single institution. Both amniocentesis and CVS were available during the entirety of the study period. CfDNA screening became available at our institution in January 2012. The study period could not be extended prior to 2010 due to limitations in our electronic medical record system. This study was approved by the Medical University of South Carolina Institutional Review Board (IRB), with IRB study number 00121930.
For each case, clinical records were abstracted to identify the gestational age (GA) at diagnostic testing, indications for diagnostic testing, results of testing, and pregnancy outcome. Indications for testing included advanced maternal age (AMA) alone, abnormal ultrasound findings, abnormal maternal prenatal screening, parental carrier status, and family history/other as outlined in the procedural note. A fetal aneuploidy diagnosis was confirmed by an abnormal karyotype or other cytogenetic result from either amniocentesis or CVS specimen.
Pregnancy outcome was recorded as either continuation of pregnancy or abortion. GA and date of abortion were extracted from the medical record. Abortion services were available at our center throughout the study period, but South Carolina enacted three abortion restrictions during this period with a potential impact on access. Specifically, South Carolina enacted a 24-hour waiting period in June 2010, a 20-week ban in May 2016, and a 6-week ban in June 2022. Each new restriction required time for interpretation, clarification, and implementation of new policies and procedures to ensure compliance before altered service provision could continue. Patients with no documented date of abortion (e.g., those who pursued abortion at other facilities) or unknown pregnancy outcomes were excluded in the analysis of interval to abortion.
The sample was evaluated with descriptive statistics. Proportions were compared using chi-square and Kruskal–Wallis tests where appropriate. For each study year, median GA with interquartile range (IQR) at diagnosis and abortion were reported, as the data were not normally distributed. All analyses were performed via GraphPad Prism Version 10.0.1 (170).
Results
From 2010 to 2022, 1,262 patients underwent invasive diagnostic testing for suspected fetal aneuploidy, with 258 (20.5%) genetic abnormalities identified. Of total procedures, 888 (70.4%) were amniocentesis, and 374 (29.6%) were CVS. There was a significant decline in total procedures performed over time (p < 0.001; [Fig. 1]). [Table 1] displays the proportion of amniocentesis and CVS during the study period. Amniocentesis remained the most frequently performed procedure, ranging from 60.2 to 76.3% of procedures over the 12-year study period.

[Fig. 2] displays the changes in indication for diagnostic testing over time. AMA as the sole indication for diagnostic testing declined from 45 to 5.6% (p < 0.001). Testing for an indication of abnormal prenatal screen (including maternal serum analyte testing or cfDNA) ranged from 46.2% in 2014 to a nadir of 15.6% in 2021 (p = 0.004). The frequency of testing prompted by ultrasound findings increased from 17.7% in 2020 to 50.0% in 2022 (p < 0.001).

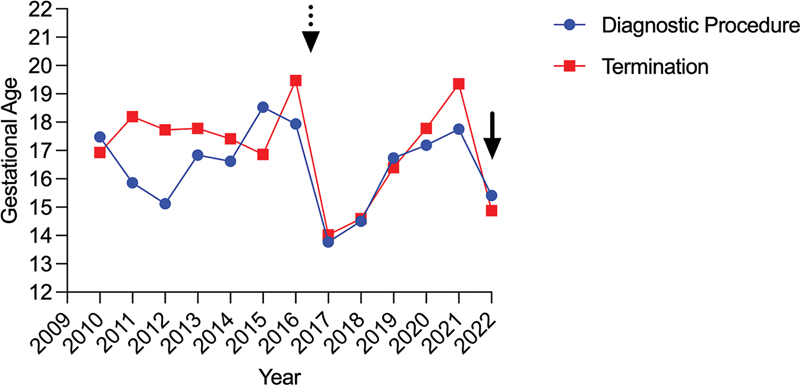
The number of fetal aneuploidy cases varied per year from 12 (2021) to 34 (2012), totaling 253 genetic abnormalities diagnosed by invasive testing. There was considerable variation in GA at diagnosis of fetal aneuploidy over the study period, ranging from 13.5 weeks (IQR: 12.0–15.5) in 2017 to 19.0 weeks (IQR: 12.0–21.0) in 2021. Of the abnormal results, the majority (n = 166, 65.6%) were autosomal trisomies; trisomy 21 was the most frequently diagnosed (56.0%). Microdeletions/duplications were also identified frequently (n = 48, 18.9%), followed by sex chromosome aneuploidy (n = 28, 11.1%; [Table 2]).
A total of 113 patients with invasive prenatal testing and fetal aneuploidy elected for abortion, representing 45% of all patients with diagnosed genetic abnormalities. [Fig. 3] demonstrates the GA of abortion during the study period. The median GA at abortion varied greatly over the study period, ranging from a median GA of 13.9 weeks (IQR: 13.1–16.5) in 2017 to 20.0 weeks (IQR: 18.0–21.0) in 2021.
A total of 388 patients underwent an invasive diagnostic procedure following an abnormal prenatal screen during the study period (quadruple screening, sequential testing, or cfDNA; [Table 3]). Most patients underwent amniocentesis (81.7%); however, when compared by the type of prenatal screen, patients with abnormal cfDNA had a significantly greater proportion of CVS procedures than those with maternal serum analyte testing (30.7 vs. 8.9%; p < 0.001). GA at diagnosis was significantly lower for patients with abnormal cfDNA compared with those with analyte testing (15.4 vs. 17.8 weeks; p < 0.001) and was associated with a significantly higher abnormal diagnostic yield with the invasive procedure (60.4 vs. 13.2%; p < 0.001). Patients with abnormal cfDNA also had earlier abortions than those with abnormal maternal serum analyte testing (15.6 vs. 19.3 weeks; p = 0.002).
Abbreviations: cfDNA, cell-free DNA; CVS, chorionic villus sampling; GA, gestational age.
Note: GA at abortion: n = 14 for analytes, n = 50 for cfDNA. Analyte testing: traditional quadruple screen and sequential testing.
Discussion
Main Findings
There have been significant shifts in the volume and indications for invasive prenatal testing since the introduction of cfDNA for fetal aneuploidy screening. When stratified by the type of prenatal screening, the impact becomes apparent. Patients with abnormal cfDNA testing have diagnostic procedures performed at earlier GA with a significantly higher yield of abnormal genetic results compared with those with abnormal maternal serum analyte testing. Consequently, patients undergoing cfDNA testing with abnormal invasive testing results were able to elect abortion earlier than those with analyte testing. This is important as nearly half of patients with diagnosed genetic abnormalities sought abortion care in this study.
Our study reveals significant shifts in both the volume and indications for invasive testing over a 12-year period, consistent with previous studies.[3] The total number of invasive diagnostic procedures significantly decreased during the study period from approximately 300 per year prior to cfDNA availability, to approximately 100 per year in the era of cfDNA. At our institution, cfDNA testing became available in 2012. While the frequency of both amniocentesis and CVS fell over time, the reduction in amniocentesis procedures was far more remarkable than the reduction in CVS. Many patients in our study received normal diagnostic results after abnormal prenatal screening, reinforcing that prenatal screening is not a replacement for diagnostic testing.
The most dramatic shift in indication for testing was in the AMA alone category, ranging from 45% at the beginning of the study period to 5.6% in 2022. This trend has been confirmed in other studies and alludes to the fact that cfDNA effectively screens for chromosomal abnormalities that are most affected by AMA (autosomal trisomies).[9] [10] [11] As expected, trisomies, sex chromosomal aneuploidies, and microdeletions/duplications were the leading chromosomal abnormalities identified in our cohort.
Awomolo et al demonstrated that diagnostic yield increased in the era of cfDNA, identifying an improved positive predictive value (PPV) of cfDNA, as well as fewer patients seeking testing for lower-risk AMA.[1] [3] As cfDNA testing companies broaden their testing to include less common trisomies, microdeletions/duplications, and genome-wide screening, it is anticipated that the PPV will likely decrease.[12] [13] This has important implications, as a lower PPV may contribute to a decrease in diagnostic yield over time.
These trends collectively paint a picture of evolving prenatal care practices, where diagnostic procedures are increasingly reserved for cases with higher pretest probabilities of genetic abnormalities as is now being provided by cfDNA screening. The improved targeting of high-risk pregnancies for invasive testing reduces the number of pregnancies exposed to the risks of invasive testing.[3] [8]
Stratification by prenatal screening method revealed that patients with abnormal cfDNA underwent earlier diagnostic testing compared with those with abnormal maternal serum analyte screening, along with a significantly earlier GA at abortion. However, even with cfDNA screening, the GA at diagnosis often surpasses the GA limits for legal abortion in numerous states, which is particularly significant given the increasingly restrictive abortion regulations across the United States.[14]
This highlights persistent barriers to early screening and sonography, along with the fact that some fetal anomalies and chromosomal abnormalities remain undetectable in the first trimester. As could be expected, the shift away from AMA and the increase in ultrasound anomalies as the primary indication for testing underscores the growing reliance on detailed anatomical assessment and nuanced risk stratification in prenatal care beyond age-based risks alone. Further, increased emphasis on ultrasound examinations may have led to earlier detection of anomalies, potentially bypassing or complementing screening in some cases.
GA at abortion varied across the study period with a potential correlation with restrictive abortion legislation and mirrors the timing of diagnostic procedures, underscoring the importance of timely screening and diagnosis. GA at abortion was earlier in patients with abnormal cfDNA. This has clinical implications, as the procedural approach to abortion changes with advancing gestation, with differences in cervical preparation, cost, and risk.[15] [16] [17]
Moreover, abortion restrictions in several states include exceptions for lethal fetal anomalies or genetic conditions; however, the definition of lethality regarding genetic abnormalities is often ambiguous and varies between states. While many genetic conditions may not be immediately lethal at birth, they can have profound implications for quality of life. Therefore, clinicians must provide comprehensive counseling that includes the nuances of legal definitions and implications of various conditions.
The findings of our study emphasize the importance of maintaining accessibility to CVS procedures. The primary advantage of CVS over amniocentesis is its earlier timing, particularly in terms of facilitating earlier decision-making. CVS is offered between 10 and 13 weeks of gestation compared with amniocentesis as early as 15 weeks of gestation. The viable cells obtained by CVS allow for specimen processing in 5 to 7 versus 7 to 14 days for amniocentesis, providing results earlier in pregnancy.[18] The timing can be crucial for decision-making and reproductive autonomy.
However, CVS historically carries a slightly higher risk of miscarriage compared with amniocentesis, with rates ranging from 0.5 to 1% for CVS and 0.25 to 0.5% for amniocentesis.[18] Encouragingly, the pregnancy loss rate from CVS has decreased over time and with greater operator experience. A recent meta-analysis encompassing 8,899 women who had CVS calculated a procedure-related loss rate of 0.22% (1 in 455).[19] Further, while early studies suggested a possible link between CVS and limb-reduction defects, current evidence indicates that when performed after 10 weeks of gestation, the risk is comparable to the general population.[20]
Additionally, these findings have implications for maternal–fetal medicine procedural training. Dobson et al found that 62% of patients with abnormal cfDNA opted for diagnostic testing, but only approximately one-third of patients undergoing diagnostic testing for an abnormal cfDNA had a CVS performed.[21] One study revealed that only 30% of maternal–fetal medicine fellows feel comfortable performing CVS, and several studies have demonstrated the steep learning curve associated with CVS training.[22] [23] [24] Considering potential increases in CVS requests as a result of the evolution of cfDNA screening and following the Dobbs decision, further investigation into simulation-based training and procedural learning in the setting of early pregnancy failure or abortion is warranted to enhance provider competence and preparedness.[22] [25]
Extending the study period to include patients in the post-Dobbs era would allow for analysis of temporal changes in prenatal testing patterns, and barriers to abortion access in response to increasingly restrictive policies. Additionally, the definition of fatal fetal diagnoses remains elusive, with varying definitions between states.[14] This has implications for geographic and financial barriers to seeking abortion for fetal aneuploidy, as well as an impact on the delivery of patient-centered care.[26]
Additional questions remain about the residual risk of genetic abnormalities when cfDNA is low risk, in the setting of both normal and abnormal ultrasound findings.[27] [28] This is especially important as technology expands to include exome and genome testing.[29] Future research should focus on the specific cytogenetic technologies employed and diagnostic yield with invasive testing.
Strengths and Limitations
Our study's strengths lie in its extended duration of observation, providing a comprehensive analysis of trends in prenatal diagnostic procedures, indications, and outcomes over a 12-year period. Access to providers with CVS training did not change during the study period. The examination of GA at both diagnosis and abortion offers valuable insights into the timing of care in the context of evolving prenatal testing technologies and increasingly restrictive abortion laws.
Limitations include the lack of data prior to 2012 due to electronic record constraints, preventing temporal cohort comparison before cfDNA testing was available. The study's retrospective design may limit data collection and interpretation. Additionally, changes in referral patterns and access to care could not be ascertained in this study; these variables could contribute to varying patterns in antenatal diagnostic testing.
Patients with structural anomalies who did not undergo diagnostic testing were excluded from this study, yet they constitute an important patient population. Lastly, our design did not account for South Carolina's progressively tightening abortion restrictions during the study period, which included a 24-hour waiting period in 2010, a 20-week ban in 2016, and a 6-week ban in 2022.
Conclusion
In conclusion, our study highlights significant shifts in prenatal diagnostic practices since the introduction of cfDNA testing for fetal aneuploidy screening. Over this time period, there has been a marked reduction in the volume of invasive procedures and a shift in indications—particularly a decline in testing based solely on AMA alone. The increased utilization of cfDNA screening has resulted in significantly earlier diagnostic testing and abortion compared with traditional analyte screening. Unfortunately, the GA at diagnosis of fetal aneuploidy remains advanced into the second trimester. The persistence of an advanced GA at diagnosis and abortion timing even among patients with cfDNA reveals the ongoing challenges related to timely diagnosis of fetal aneuploidy, to optimize patients' opportunities for safe, comprehensive management.
Conflict of Interest
None declared.
Note
The findings were presented at the Society of Maternal Fetal Medicine 44th Annual Pregnancy Meeting, National Harbor, Maryland in February 2024.
Authors' Contributions
All authors contributed to the manuscript substantially and have agreed to the final submitted version. E.R.M. was involved in conceptualizing, designing, analyzing, and interpreting data. R.N. and A.D. contributed to analysis, interpretation, and drafting. J.L., E.A., and K.S. substantially contributed to the acquisition, analysis, and drafting of the manuscript.
Ethical Statement
This study was approved by the Medical University of South Carolina Institutional Review Board (IRB), with IRB study number 00121930; date of approval July 7, 2022. No additional ethics approval is applicable.
-
References
- 1 Rose NC, Kaimal AJ, Dugoff L, Norton ME. American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics, Committee on Genetics, Society for Maternal-Fetal Medicine. Screening for fetal chromosomal abnormalities: ACOG practice bulletin, number 226. Obstet Gynecol 2020; 136 (04) e48-e69
- 2 Hassold T, Hall H, Hunt P. The origin of human aneuploidy: where we have been, where we are going. Hum Mol Genet 2007; 16 Spec No. 2 (16) R203-R208
- 3 Awomolo A, Palomares K, Garcia GH, Rosen T, Duzyj C, Ashkinadze E. Trends in invasive prenatal diagnostic testing at a single institution. Prenat Diagn 2018; 38 (10) 735-739
- 4 Gil MM, Quezada MS, Bregant B, Ferraro M, Nicolaides KH. Implementation of maternal blood cell-free DNA testing in early screening for aneuploidies. Ultrasound Obstet Gynecol 2013; 42 (01) 34-40
- 5 Kim K, Craft LK. Non-invasive prenatal testing in mitigating concerns from invasive prenatal diagnostic testing: retrospective assessment of utility in an academic healthcare system in the US. BMJ Open 2022; 12 (06) e057658
- 6 Hui L, Muggli EE, Halliday JL. Population-based trends in prenatal screening and diagnosis for aneuploidy: a retrospective analysis of 38 years of state-wide data. BJOG 2016; 123 (01) 90-97
- 7 Comas C, Echevarria M, Rodríguez I, Serra B, Cirigliano V. Prenatal invasive testing: a 13-year single institution experience. J Matern Fetal Neonatal Med 2014; 27 (12) 1209-1212
- 8 Khalifeh A, Weiner S, Berghella V, Donnenfeld A. Trends in invasive prenatal diagnosis: effect of sequential screening and noninvasive prenatal testing. Fetal Diagn Ther 2016; 39 (04) 292-296
- 9 Forabosco A, Percesepe A, Santucci S. Incidence of non-age-dependent chromosomal abnormalities: a population-based study on 88965 amniocenteses. Eur J Hum Genet 2009; 17 (07) 897-903
- 10 Hook EB. Rates of chromosome abnormalities at different maternal ages. Obstet Gynecol 1981; 58 (03) 282-285
- 11 Srebniak MI, Joosten M, Knapen MFCM. et al. Frequency of submicroscopic chromosomal aberrations in pregnancies without increased risk for structural chromosomal aberrations: systematic review and meta-analysis. Ultrasound Obstet Gynecol 2018; 51 (04) 445-452
- 12 Lefkowitz RB, Tynan JA, Liu T. et al. Clinical validation of a noninvasive prenatal test for genomewide detection of fetal copy number variants. Am J Obstet Gynecol 2016; 215 (02) 227.e1-227.e16
- 13 Ehrich M, Tynan J, Mazloom A. et al. Genome-wide cfDNA screening: clinical laboratory experience with the first 10,000 cases. Genet Med 2017; 19 (12) 1332-1337
- 14 Raymond MB, Barbera JP, Boudova S. et al. Implications for prenatal genetic testing in the United States after the reversal of Roe v Wade. Obstet Gynecol 2023; 141 (03) 445-454
- 15 Diedrich JT, Drey EA, Newmann SJ. Society of Family Planning clinical recommendations: cervical preparation for dilation and evacuation at 20-24 weeks' gestation. Contraception 2020; 101 (05) 286-292
- 16 Allen RH, Goldberg AB. Cervical dilation before first-trimester surgical abortion (<14 weeks' gestation). Contraception 2016; 93 (04) 277-291
- 17 Spingler T, Sonek J, Hoopmann M, Prodan N, Abele H, Kagan KO. Complication rate after termination of pregnancy for fetal defects. Ultrasound Obstet Gynecol 2023; 62 (01) 88-93
- 18 Norton ME, Jackson M. Practice bulletin no. 162 prenatal diagnostic testing for genetic disorders. Obstet Gynecol 2016; 127 (05) 108-122
- 19 Akolekar R, Beta J, Picciarelli G, Ogilvie C, D'Antonio F. Procedure-related risk of miscarriage following amniocentesis and chorionic villus sampling: a systematic review and meta-analysis. Ultrasound Obstet Gynecol 2015; 45 (01) 16-26
- 20 Botto LD, Olney RS, Mastroiacovo P. et al. Chorionic villus sampling and transverse digital deficiencies: evidence for anatomic and gestational-age specificity of the digital deficiencies in two studies. Am J Med Genet 1996; 62 (02) 173-178
- 21 Dobson LJ, Reiff ES, Little SE, Wilkins-Haug L, Bromley B. Patient choice and clinical outcomes following positive noninvasive prenatal screening for aneuploidy with cell-free DNA (cfDNA). Prenat Diagn 2016; 36 (05) 456-462
- 22 Gimovsky AC, Moreno SC, Nicholas S, Roman A, Weiner S. How many procedures does it take? Success of a CVS training program for maternal fetal medicine fellows. Prenat Diagn 2016; 36 (13) 1257-1260
- 23 Warsof SL, Larion S, Abuhamad AZ. Overview of the impact of noninvasive prenatal testing on diagnostic procedures. Prenat Diagn 2015; 35 (10) 972-979
- 24 Holliman K, Pluym ID, Grechukhina O. et al. Maternal-fetal medicine fellows' perception and comfort with obstetrical ultrasound and prenatal diagnosis. Am J Obstet Gynecol MFM 2022; 4 (03) 100601
- 25 Nicholas S, Orzechowski K, Potti S, Baxter J, Berghella V, Weiner S. Early pregnancy failure as a training tool for chorionic villus sampling. Prenat Diagn 2013; 33 (11) 1110-1112
- 26 Sabbath EL, McKetchnie SM, Arora KS, Buchbinder M. US obstetrician-gynecologists' perceived impacts of post-dobbs v Jackson State abortion bans. JAMA Netw Open 2024; 7 (01) e2352109
- 27 Sagi-Dain L, Singer A, Segel R, Berger R, Kanengisser-Pines B, Maya I. The yield of chromosomal microarray in pregnancies with congenital cardiac defects and normal noninvasive prenatal screening. Am J Obstet Gynecol 2021; 225 (03) 333.e1-333.e14
- 28 Sagi-Dain L, Salzer Sheelo L, Brabbing-Goldstein D. et al. Chromosomal microarray analysis compared with noninvasive prenatal testing in pregnancies with abnormal maternal serum screening. Obstet Gynecol 2022; 139 (05) 877-887
- 29 Van den Veyver IB, Chandler N, Wilkins-Haug LE, Wapner RJ, Chitty LS. ISPD Board of Directors. International Society for Prenatal Diagnosis Updated Position Statement on the use of genome-wide sequencing for prenatal diagnosis. Prenat Diagn 2022; 42 (06) 796-803
Address for correspondence
Publication History
Received: 07 March 2025
Accepted: 25 March 2025
Article published online:
30 April 2025
© 2025. Thieme. All rights reserved.
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Rose NC, Kaimal AJ, Dugoff L, Norton ME. American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics, Committee on Genetics, Society for Maternal-Fetal Medicine. Screening for fetal chromosomal abnormalities: ACOG practice bulletin, number 226. Obstet Gynecol 2020; 136 (04) e48-e69
- 2 Hassold T, Hall H, Hunt P. The origin of human aneuploidy: where we have been, where we are going. Hum Mol Genet 2007; 16 Spec No. 2 (16) R203-R208
- 3 Awomolo A, Palomares K, Garcia GH, Rosen T, Duzyj C, Ashkinadze E. Trends in invasive prenatal diagnostic testing at a single institution. Prenat Diagn 2018; 38 (10) 735-739
- 4 Gil MM, Quezada MS, Bregant B, Ferraro M, Nicolaides KH. Implementation of maternal blood cell-free DNA testing in early screening for aneuploidies. Ultrasound Obstet Gynecol 2013; 42 (01) 34-40
- 5 Kim K, Craft LK. Non-invasive prenatal testing in mitigating concerns from invasive prenatal diagnostic testing: retrospective assessment of utility in an academic healthcare system in the US. BMJ Open 2022; 12 (06) e057658
- 6 Hui L, Muggli EE, Halliday JL. Population-based trends in prenatal screening and diagnosis for aneuploidy: a retrospective analysis of 38 years of state-wide data. BJOG 2016; 123 (01) 90-97
- 7 Comas C, Echevarria M, Rodríguez I, Serra B, Cirigliano V. Prenatal invasive testing: a 13-year single institution experience. J Matern Fetal Neonatal Med 2014; 27 (12) 1209-1212
- 8 Khalifeh A, Weiner S, Berghella V, Donnenfeld A. Trends in invasive prenatal diagnosis: effect of sequential screening and noninvasive prenatal testing. Fetal Diagn Ther 2016; 39 (04) 292-296
- 9 Forabosco A, Percesepe A, Santucci S. Incidence of non-age-dependent chromosomal abnormalities: a population-based study on 88965 amniocenteses. Eur J Hum Genet 2009; 17 (07) 897-903
- 10 Hook EB. Rates of chromosome abnormalities at different maternal ages. Obstet Gynecol 1981; 58 (03) 282-285
- 11 Srebniak MI, Joosten M, Knapen MFCM. et al. Frequency of submicroscopic chromosomal aberrations in pregnancies without increased risk for structural chromosomal aberrations: systematic review and meta-analysis. Ultrasound Obstet Gynecol 2018; 51 (04) 445-452
- 12 Lefkowitz RB, Tynan JA, Liu T. et al. Clinical validation of a noninvasive prenatal test for genomewide detection of fetal copy number variants. Am J Obstet Gynecol 2016; 215 (02) 227.e1-227.e16
- 13 Ehrich M, Tynan J, Mazloom A. et al. Genome-wide cfDNA screening: clinical laboratory experience with the first 10,000 cases. Genet Med 2017; 19 (12) 1332-1337
- 14 Raymond MB, Barbera JP, Boudova S. et al. Implications for prenatal genetic testing in the United States after the reversal of Roe v Wade. Obstet Gynecol 2023; 141 (03) 445-454
- 15 Diedrich JT, Drey EA, Newmann SJ. Society of Family Planning clinical recommendations: cervical preparation for dilation and evacuation at 20-24 weeks' gestation. Contraception 2020; 101 (05) 286-292
- 16 Allen RH, Goldberg AB. Cervical dilation before first-trimester surgical abortion (<14 weeks' gestation). Contraception 2016; 93 (04) 277-291
- 17 Spingler T, Sonek J, Hoopmann M, Prodan N, Abele H, Kagan KO. Complication rate after termination of pregnancy for fetal defects. Ultrasound Obstet Gynecol 2023; 62 (01) 88-93
- 18 Norton ME, Jackson M. Practice bulletin no. 162 prenatal diagnostic testing for genetic disorders. Obstet Gynecol 2016; 127 (05) 108-122
- 19 Akolekar R, Beta J, Picciarelli G, Ogilvie C, D'Antonio F. Procedure-related risk of miscarriage following amniocentesis and chorionic villus sampling: a systematic review and meta-analysis. Ultrasound Obstet Gynecol 2015; 45 (01) 16-26
- 20 Botto LD, Olney RS, Mastroiacovo P. et al. Chorionic villus sampling and transverse digital deficiencies: evidence for anatomic and gestational-age specificity of the digital deficiencies in two studies. Am J Med Genet 1996; 62 (02) 173-178
- 21 Dobson LJ, Reiff ES, Little SE, Wilkins-Haug L, Bromley B. Patient choice and clinical outcomes following positive noninvasive prenatal screening for aneuploidy with cell-free DNA (cfDNA). Prenat Diagn 2016; 36 (05) 456-462
- 22 Gimovsky AC, Moreno SC, Nicholas S, Roman A, Weiner S. How many procedures does it take? Success of a CVS training program for maternal fetal medicine fellows. Prenat Diagn 2016; 36 (13) 1257-1260
- 23 Warsof SL, Larion S, Abuhamad AZ. Overview of the impact of noninvasive prenatal testing on diagnostic procedures. Prenat Diagn 2015; 35 (10) 972-979
- 24 Holliman K, Pluym ID, Grechukhina O. et al. Maternal-fetal medicine fellows' perception and comfort with obstetrical ultrasound and prenatal diagnosis. Am J Obstet Gynecol MFM 2022; 4 (03) 100601
- 25 Nicholas S, Orzechowski K, Potti S, Baxter J, Berghella V, Weiner S. Early pregnancy failure as a training tool for chorionic villus sampling. Prenat Diagn 2013; 33 (11) 1110-1112
- 26 Sabbath EL, McKetchnie SM, Arora KS, Buchbinder M. US obstetrician-gynecologists' perceived impacts of post-dobbs v Jackson State abortion bans. JAMA Netw Open 2024; 7 (01) e2352109
- 27 Sagi-Dain L, Singer A, Segel R, Berger R, Kanengisser-Pines B, Maya I. The yield of chromosomal microarray in pregnancies with congenital cardiac defects and normal noninvasive prenatal screening. Am J Obstet Gynecol 2021; 225 (03) 333.e1-333.e14
- 28 Sagi-Dain L, Salzer Sheelo L, Brabbing-Goldstein D. et al. Chromosomal microarray analysis compared with noninvasive prenatal testing in pregnancies with abnormal maternal serum screening. Obstet Gynecol 2022; 139 (05) 877-887
- 29 Van den Veyver IB, Chandler N, Wilkins-Haug LE, Wapner RJ, Chitty LS. ISPD Board of Directors. International Society for Prenatal Diagnosis Updated Position Statement on the use of genome-wide sequencing for prenatal diagnosis. Prenat Diagn 2022; 42 (06) 796-803