

Subscribe to RSS
DOI: 10.1055/a-2542-4290
Management of Direct Oral Anticoagulants in Acute Type A Aortic Dissection
Authors
Funding None.

Abstract
Background Direct oral anticoagulants (DOACs) are a commonly used class of anti-coagulants that may complicate surgical management of acute Type A aortic dissection (ATAAD).
Methods Surgical management and clinical courses were described for patients who presented to our institution with ATAAD while taking DOACs, after FDA approval of the two currently available reversal agents. A thorough literature review was completed for cases of administration of DOAC reversal agents in ATAAD.
Results The only patient treated with andexanet-alfa had heparin insensitivity while on cardiopulmonary bypass. Four other patients were successfully managed with a combination of surgical delay and factor repletion.
Conclusion This case series demonstrates that preoperative management of DOACs in patients with ATAAD may employ factor repletion with success. Literature review demonstrated a safety signal for heparin insensitivity or pump thrombosis when andexanet-alfa was administered before or while on cardiopulmonary bypass or extracorporeal membrane oxygenation. Our institutional clinical practice guidelines recommend against administration of andexanet-alfa within 4 to 6 hours before heparinization for surgery in ATAAD but recommend considering andexanet-alfa administration when there is life-threatening bleeding after heparin reversal that is thought to be due to Xa-inhibition with laboratory evidence of elevated anti-Xa activity.
Introduction
Direct oral anticoagulants (DOACs) are a class of medications that are commonly encountered in cardiac surgery and include the factor Xa-inhibitors apixaban, rivaroxaban, and edoxaban and thrombin inhibitor dabigatran. However, despite their prevalence, evidence on how to proceed with emergent cardiac surgical procedures in the setting of recent DOAC administration is scarce.[1] [2] While it is standard practice to await clearance of the DOAC when surgery can be delayed, proper management is less clear when cardiac surgery is emergently indicated. With regard to acute Type A aortic dissection (ATAAD), a clinical condition distinguished from other emergent cardiac surgical conditions by the high risk of preoperative and postoperative bleeding and thrombosis, evidence for how to manage DOACs is limited to case reports and small case series.[3] [4] [5] [6] [7] [8] [9] [10] [11] [12] Nonetheless, it is known that DOACs carry increased risk for uncontrolled bleeding and prolonged operative time in ATAAD compared with vitamin K antagonists.[13] Furthermore, DOACs are associated with higher mortality after surgery for ATAAD compared with no anticoagulation at all.[13] [14]
There are two FDA-approved reversal agents for DOACs. Andexanet-alfa is a recombinant factor Xa that competitively reverses Xa-inhibitors (approved for apixaban and rivaroxaban).[15] [16] Idarucizumab is a monoclonal antibody that reverses the effects of the thrombin inhibitor dabigatran.[17] In 2020, the European Medicines Agency released a communication warning against use of preoperative andexanet-alfa in cardiac surgery due to risk of heparin insensitivity.[18] However, in 2021, the Society for Thoracic Surgeons (STS) still recommended use of andexanet-alfa or idarucizumab in patients on DOACs before emergent cardiac surgery.[19] A recent review of case reports and series, describing 9 patients on Xa-inhibitors and 84 patients on dabigatran who were undergoing emergent cardiac surgical procedures, found that administration of andexanet-alfa before cardiopulmonary bypass (CPB) was associated with heparin insensitivity, sometimes leading to thrombosis, but that idarucizumab was safe for use at any phase of surgery.[1] They recommended use of prothrombin complex concentrate (4F-PCC) in patients on Xa-inhibitors and the use of idarucizumab in patients on thrombin inhibitors undergoing emergent cardiac surgery.[1] Another recent review reported similar findings, adding that hemoadsorption of DOACs and P2Y12 inhibitors may also be safe and effective to reverse anticoagulation and antiplatelet effects.[2] Nonetheless, evidence supporting or discouraging use of andexanet-alfa or idarucizumab for reversal of DOACs before or after emergent surgery for ATAAD remains limited. Therefore, we conducted a retrospective case series of patients with recent DOAC ingestion undergoing emergent aortic surgery for ATAAD.
Materials and Methods
All patients who underwent aortic repair or replacement for ATAAD from October 2015 through December 2021 were screened in this retrospective chart review. Inclusion criteria for the case series included (1) presentation for ATAAD, defined as symptom onset within the last 2 weeks, (2) underwent aortic repair or replacement, (3) was prescribed outpatient DOACs at the time of dissection and reported a dose within the last 3 days or had laboratory evidence of elevated anti-Xa activity. Of 136 patients who were screened, 6 patients met inclusion criteria. However, one patient did not provide consent, resulting in a series comprising of five patients. Consent to publish clinical information was obtained from all other patients or from their proxies, with the exception of one patient who was lost to follow-up. Institutional review board approval was not required to publish this case series. Their presentations and clinical courses are described below and in [Table 1].
Results
Case 1
Patient one was an 82-year-old man with a history of hypertension, prior stroke without atrial fibrillation on apixaban 5 mg twice a day, abdominal aortic aneurysm status after endovascular aneurysm repair, and peripheral artery disease who presented with 5 days of neck and upper chest pain. He last took apixaban the morning of his presentation. He presented to our institution after an outpatient computed tomography (CT) demonstrated a crescentic intramural hematoma of the ascending aorta extending from the sinotubular junction (STJ) to the mid transverse arch as well as a small pericardial effusion with active extravasation. His fondaparinux-calibrated anti-Xa level on presentation was 1.89 mg/L (discordant assay, reference: prophylactic dosing 0.39–0.5 mg/L).
He was taken emergently to surgery and was given 2,949 units 4F-PCC immediately prior to incision. He underwent successful aortic root repair, aortic valve resuspension, and replacement of the ascending aorta. After weaning from CPB, the patient was given another 4,915 units of 4F-PCC, 1 unit of fresh-frozen plasma (FFP), and 1 unit of platelets.
His postoperative course was complicated by a pleural effusion requiring thoracentesis on postoperative day (POD) 14 and pneumonia requiring antibiotics. He was discharged to a rehabilitation facility on POD 18 but passed away 15 days later from unspecified causes.
Case 2
Patient two was a 73-year-old man with a history of hypertension, unprovoked pulmonary embolism now on apixaban 2.5 mg twice a day, and a known thoracoabdominal aortic aneurysm, who presented 24 hours after acute onset of substernal chest pain with radiation to the back. The time of the last dose of apixaban was unknown, but his apixaban-calibrated anti-Xa level was 40 ng/mL (reference: peak 59–321ng/mL, trough 22–230ng/mL). Computed tomography angiography (CTA) demonstrated a ATAAD extending from the STJ to the level of the infrarenal abdominal aorta, also involving the right brachiocephalic artery, the right subclavian artery, and the right common carotid artery.
He was taken emergently to the operating room (OR) where he underwent aortic valve resuspension, Sinus of Valsalva repair, ascending aorta repair and total arch replacement with an elephant trunk graft extending into the distal aorta. Notably, there was bleeding from the descending aorta beyond the distal suture line, which was controlled with pledgeted sutures. Upon decannulation, there was a sudden increase in bleeding from the aortic root at the noncoronary sinus of Valsalva, so CPB was reinitiated and the area was repaired. In total, he received 4,352 units of 4F-PCC, 14,974 mg of fibrinogen, 3 units of packed red blood cells (pRBCs), 7 units of FFP, and 4 units of platelets.
His postoperative course was complicated by concern for pulmonary embolism requiring a titratable heparin drip, a right basal ganglia stroke secondary to right common carotid dissection, tachycardic–bradycardic syndrome with atrial fibrillation and atrial flutter, delirium, and severe Clostridium difficile colitis. He also required an additional unit of pRBCs on POD 3. He was medically ready for discharge on POD 35 and was discharged to a rehabilitation facility.
Case 3
Patient three was a 79-year-old woman with a history of hypertension, atrial fibrillation on rivaroxaban 20 mg, and pericarditis status after pericardial window who was transferred from an outside hospital (OSH) with 1 day of chest pain and a CTA notable for an intramural hematoma involving the aortic root and ascending aorta. Her last dose of rivaroxaban was taken 24 hours prior to presentation and her fondaparinux-calibrated anti-Xa activity level on admission was 0.76 mg/L (discordant assay, reference: prophylactic dosing 0.39–0.5 mg/L). Given her age and hemodynamic stability, combined with the surgical team's expectation for extensive surgery and unfamiliarity with idarucizumab, surgery was delayed and she was admitted to the intensive care unit to allow rivaroxaban washout.
Two days later, she underwent a bio-Bentall procedure with right coronary artery reconstruction and hemiarch replacement. After rewarming was complete and the patient had been weaned from CPB, significant coagulopathy was encountered but was successfully managed with topical hemostatic agents, 2,000 units 4F-PCC, and 6,853 mg fibrinogen. Intraoperatively, she received 2 units of pRBCs, 2 units FFP, 3 units of platelets, and 350 mL of cell-saver RBCs. Immediately postoperatively, she continued to have sanguineous chest tube output and was given 1 mg recombinant Factor VIIa. Over the remainder of her admission, she received an additional 2 units of pRBCs.
Her postoperative course was otherwise notable for the development of atrial fibrillation on POD 3, pneumonia complicated by respiratory failure requiring reintubation on POD 4, thoracentesis of bilateral loculated pleural effusions on POD 10, and gradual improvement of respiratory status with extubation on POD 11. Following extubation, she was found to have multiple early and late subacute cerebral subacute infarcts, most likely of cardioembolic etiology. She was started on warfarin for stroke prevention on POD 20 and was discharged to a rehabilitation facility on POD 22. Unfortunately, she passed away 7 days later, although the details of her death are not available to our institution.
Case 4
Patient 4 was a 78-year-old woman with a history of hypertension and paroxysmal atrial fibrillation on apixaban 5 mg twice a day who was transferred from an OSH with sharp chest pain that radiated to her back. She was found to have an ATAAD that extended from the aortic root to the left external iliac artery, with the celiac and left renal arteries arising from the false lumen. She reported last taking apixaban approximately 8 hours prior, and her heparin-calibrated anti-Xa activity level on admission was 1.94 IU/mL (discordant assay, therapeutic range: 0.3–0.7 IU/mL).
She was taken emergently to the OR where she underwent repair of the sinus of Valsalva, resuspension of the aortic valve, total arch replacement, and elephant trunk positioned in the descending aorta with reimplantation of the brachiocephalic and left carotid arteries, sacrificing the left subclavian artery. After decannulating from CPB, her anti-Xa activity was 0.68, so the decision was made to not administer andexanet-alfa. Intraoperatively, she received a total of 1,050 mL cell-saver RBCs, 4 units of pRBC, 4 units of platelets, 3 units FFP, 2,282 mg fibrinogen, 3,967 units 4F-PCC, and 250 units activated PCC (aPCC).
On POD 1, due to increased chest tube output she was given 1 unit of platelets. Her postoperative course was otherwise notable for paroxysmal atrial fibrillation and atypical flutter managed with amiodarone, delirium, and a urinary tract infection (UTI) managed with nitrofurantoin. She was started on a heparin bridge to warfarin on POD 4. She was discharged home on POD 12.
Case 5
Patient 5, whose case was previously described by Flaherty et al,[4] was a 46-year-old man with a history of ATAAD status after ascending aorta and aortic arch replacement 2 years prior that was complicated by stroke, atrial fibrillation on apixaban 5 mg twice a day, chronic kidney disease with a baseline creatinine 2.5, and migraines who presented with acute onset left frontal headache and voice hoarseness. He presented 2 days after the onset of symptoms and the last took his apixaban the morning of presentation. CTA demonstrated a 3.5-cm pseudoaneurysm of the aortic root with a surrounding 8 × 8 × 15 cm hematoma. His heparin-calibrated anti-Xa activity level the night of his admission was 1.78 IU/mL (discordant assay, therapeutic range 0.3–0.7 IU/mL). Ten hours preoperatively, he received a 400 mg bolus of andexanet-alfa followed by a continuous infusion at 4 mg/min for 2 hours.
He was taken to the OR for surgical exploration the next morning. Prior to induction, his heparin-calibrated anti-Xa activity level was 1.69 IU/mL, so an additional 400 mg bolus of andexanet-alfa was administered followed by continuous infusion at 4 mg/min for 2 hours, which completed 40 minutes prior to initiation of CPB. Given the proximity of the pseudoaneurysm to the sternum, he was peripherally cannulated and CPB was initiated via the femoral artery and vein prior to sternotomy. Notably, during heparization, 80,000 units of heparin were required to reach an activated clotting time of 434. After sternotomy, a leak was identified at a singular pleat in the noncoronary sinus and was subsequently repaired. After weaning from CPB and reversing with protamine, excellent hemostasis was noted and the sternum was closed without complication. Intra-operatively, the patient received desmopressin but no blood products or factors.
His postoperative course was notable for difficult pain control and dysphagia but was otherwise uncomplicated. He was restarted on apixaban on POD 2, and he was discharged home on POD 8.
Discussion
Herein, we describe the cases of five patients who were taking DOACs and received urgent or emergent surgery at our institution for ATAAD. Of these patients, four were taking apixaban and one was taking rivaroxaban. This case series is notable for the preoperative use of andexanet-alfa to reverse apixaban in one case. Notably, there was evidence of heparin insensitivity in this case, but there was no intraoperative thrombosis and the patient's postoperative course was not complicated by bleeding or thrombosis. The remainder of cases were successfully managed pharmacologically with administration of procoagulant factors, including 4F-PCC, FFP, and aPCC to replete factor X, as well as fibrinogen.
Review of the literature for case reports describing the use of DOAC reversal agents for surgical repair of ATAAD yielded nine articles describing thirteen separate cases, summarized in [Table 2].[1] [2] [4] [5] [6] [7] [8] [9] [10] [11] [12] Of these cases, eight patients were taking direct Xa-inhibitors and received andexanet-alfa, whereas five were taking a direct thrombin inhibitor and received idarucizumab. Of the patients who received andexanet-alfa, six received it either before or on CPB or extracorporeal membrane oxygenation, whereas two received it post-CPB. Of these six patients, all but one had heparin insensitivity or pump thrombosis after administration of andexanet-alfa. The two patients who received andexanet-alfa after CPB did not have any evidence of thrombosis.
Abbreviations: ATAAD, acute Type A aortic dissection; CPB, cardiopulmonary bypass; DOAC, direct oral anticoagulants; ECMO, extracorporeal membrane oxygenation; FFP, fresh-frozen plasma; PCC, prothrombin complex concentrate; POD, postoperative day; pRBC, packed red blood cells.
Of the patients who received idarucizumab, one received it 40 hours before surgery, two received it pre-CPB, and two received it post-CPB; there was no evidence of thrombosis in any of these patients, although there were two fatalities. Although a significant reporting bias is expected, there is additional evidence that the administration of andexanet-alfa pre-CPB is associated with heparin insensitivity or pump thrombosis, whereas this association is not evident for the administration of idarucizumab.[1]
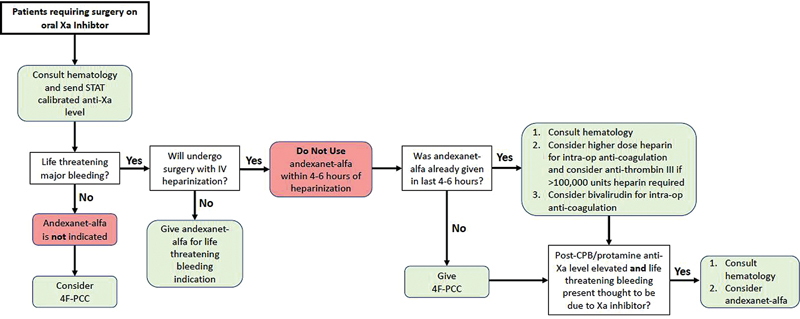
At the authors' institution, patients with normal kidney function are considered to have likely adequately cleared Xa-inhibitors beyond 18 hours after ingestion. Nonetheless, all patients receive a STAT anti-Xa activity level calibrated to the particular anticoagulant ingested and hematology is notified of the case. For patients without major life-threatening bleeding, andexanet-alfa is not indicated, and management can instead proceed with the administration of 4F-PCC. For patients with major life-threatening bleeding and who are expected to undergo surgery requiring intravenous (IV) heparin, andexanet-alfa should not be used within 4 to 6 hours of heparin administration due to its ability to induce heparin insensitivity. Instead, 4F-PCC can be given as an attempt to supply additional factor X. For patients who already received andexanet-alfa but require surgery with IV heparin, hematology is consulted, and clinicians can consider using higher doses of IV unfractionated heparin with possible administration of antithrombin III concentrate if marked heparin insensitivity is observed. They can alternatively consider anticoagulation with bivalirudin. In cases where surgery cannot be delayed, it is standard institutional practice to withhold andexanet-alfa preoperatively but to check anti-Xa activity level again after cessation of CPB and reversal of heparin, and to administer andexanet-alfa if there is life-threatening bleeding and the bleeding is thought to be due to activity of the DOAC ([Fig. 1]).
For patients who have taken dabigatran and require emergent surgery, idarucizumab 5 g is considered the first-line agent for reversal. When idarcuziumab is not available, 4F-PCC or activated PCC can be administered instead. The description of practice within the authors' institution should not be taken as a fixed protocol nor as a substitute for clinical judgment but does reflect a multidisciplinary review of existing evidence for the management of these agents.
Conclusion
In our institutional review of patients undergoing surgery for ATAAD with recent ingestion of DOACs, four patients were able to be managed with a combination of factor Xa repletion or surgical delay, while one patient who was treated with andexanet-alfa demonstrated heparin insensitivity. A review of the literature demonstrated a similar safety signal, wherein preoperative andexanet-alfa has been reported to induce heparin insensitivity or thrombosis while on CPB. We recommend against the use of andexanet-alfa in patients who are to undergo surgical aortic repair within 4 to 6 hours but rather recommend treating preoperatively with 4F-PCC or aPCC and consider post-CPB administration of andexanet-alfa if anti-Xa levels are still elevated and there is clinically relevant bleeding.
Erratum: An erratum has been published for this article (DOI: 10.1055/a-2734-4614)
Conflict of Interest
K.D.L.C. discloses being a nonpaid consultant and speaker for Terumo Aortic and Edwards Lifesciences. All other authors certify that there are no relationships with any financial organization regarding the material discussed in the manuscript.
Authors' Contribution
All authors have given substantial contributions to the conception and design of the manuscript as well as the interpretation of the data. Robert Semco performed data acquisition and Robert Semco, Thais Faggion Vinholo, and Jake Awtry substantially contributed to drafting the manuscript. All authors revised it critically. All authors read and approved the final version of the manuscript.
-
References
- 1 Heuts S, Ceulemans A, Kuiper GJAJM. et al. Optimal management of cardiac surgery patients using direct oral anticoagulants: recommendations for clinical practice. Eur J Cardiothorac Surg 2023; 64 (04) ezad340
- 2 Matejic-Spasic M, Hassan K, Thielmann M. et al. Management of perioperative bleeding risk in patients on antithrombotic medications undergoing cardiac surgery-a systematic review. J Thorac Dis 2022; 14 (08) 3030-3044
- 3 Sabe AA, Percy ED, Kaneko T, Plichta RP, Hughes GC. When to consider deferral of surgery in acute type A aortic dissection: a review. Ann Thorac Surg 2021; 111 (06) 1754-1762
- 4 Flaherty D, Connors JM, Singh S, Sylvester KW, Rimsans J, Cornella L. Andexanet alfa for urgent reversal of apixaban before aortic surgery requiring cardiopulmonary bypass: a case report. A A Pract 2019; 13 (07) 271-273
- 5 Al-Attar N, Sedeek AF, McCall P, Travers J. Andexanet alfa in acute aortic syndrome: first UK experience. Eur J Cardiothorac Surg 2023; 63 (06) ezad100
- 6 Brenner B, Guerra J, Williams C. et al. Heparin insensitivity and thrombotic risk associated with sequential uses of prothrombin complex concentrate and andexanet alfa for apixaban reversal during acute type A aortic dissection repair: a case report. A A Pract 2022; 16 (11) e01636
- 7 Honda J, Itakura Y, Tanaka S, Inoue S. Successful use of an antithrombin for heparin resistance with andexanet alfa. JA Clin Rep 2023; 9 (01) 26
- 8 Kainz M, Bsuchner P, Schellongowski P, Dworschak M. Intraoperative off-label reversal of apixaban by andexanet alfa while on VA-ECMO immediately after emergent surgery for acute type A aortic dissection. J Cardiothorac Vasc Anesth 2021; 35 (01) 262-264
- 9 Henderson Jr RS, Deshpande S, Williams B, Taylor BS, Tanaka KA. Idarucizumab for dabigatran reversal in emergency type-A aortic dissection. J Cardiothorac Vasc Anesth 2017; 31 (06) e80-e81
- 10 Tomaszuk-Kazberuk A, Łopatowska P, Młodawska E, van Ryn J, Reilly PA, Pollack CV. Successful use of idarucizumab as a reversal agent for dabigatran in a patient with acute dissected aortic aneurysm. Pol Arch Intern Med 2017; 127 (01) 68-70
- 11 Mazur P, Darocha T, Filip G, Grudzień G, Drwiła R, Kapelak B. Idarucizumab for dabigatran reversal in patients with atrial fibrillation undergoing emergency surgery for acute aortic syndrome. Pol Arch Intern Med 2016; 126 (7–8): 579-581
- 12 Hamad R, Amr G, Demers P. Delayed surgery in patients with acute type A aortic dissection who are receiving novel oral anticoagulants. J Thorac Cardiovasc Surg 2018; 155 (01) e1-e4
- 13 Sromicki J, Van Hemelrijck M, Schmiady MO. et al. Prior intake of new oral anticoagulants adversely affects outcome following surgery for acute type A aortic dissection. Interact Cardiovasc Thorac Surg 2022; 35 (01) ivac037
- 14 Bjørnstad JL, Khan AM, Røed-Undlien H. et al. Operative survival in patients with acute aortic disease in the era of newer oral anticoagulants. Open Heart 2020; 7 (02) e001278
- 15 Beik N, Reddy P, Sylvester KW. et al. Andexanet alfa (Andexxa) formulary review. Crit Pathw Cardiol 2019; 18 (02) 66-71
- 16 Reed M, Tadi P, Nicolas D. Andexanet alfa. In: StatPearls. 2024. . Accessed February 20, 2024 at: http://www.ncbi.nlm.nih.gov/books/NBK519499/
- 17 van der Horst SFB, Martens ESL, den Exter PL. et al. Idarucizumab for dabigatran reversal: a systematic review and meta-analysis of indications and outcomes. Thromb Res 2023; 228: 21-32
- 18 European Medicines Agency. Ondexxya (andexanet alfa): avoid use of Andexanet prior to heparinization. 2020
- 19 Tibi P, McClure RS, Huang J. et al. STS/SCA/AmSECT/SABM update to the clinical practice guidelines on patient blood management. J Cardiothorac Vasc Anesth 2021; 35 (09) 2569-2591
Address for correspondence
Publication History
Received: 26 July 2024
Accepted: 19 February 2025
Article published online:
08 May 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Heuts S, Ceulemans A, Kuiper GJAJM. et al. Optimal management of cardiac surgery patients using direct oral anticoagulants: recommendations for clinical practice. Eur J Cardiothorac Surg 2023; 64 (04) ezad340
- 2 Matejic-Spasic M, Hassan K, Thielmann M. et al. Management of perioperative bleeding risk in patients on antithrombotic medications undergoing cardiac surgery-a systematic review. J Thorac Dis 2022; 14 (08) 3030-3044
- 3 Sabe AA, Percy ED, Kaneko T, Plichta RP, Hughes GC. When to consider deferral of surgery in acute type A aortic dissection: a review. Ann Thorac Surg 2021; 111 (06) 1754-1762
- 4 Flaherty D, Connors JM, Singh S, Sylvester KW, Rimsans J, Cornella L. Andexanet alfa for urgent reversal of apixaban before aortic surgery requiring cardiopulmonary bypass: a case report. A A Pract 2019; 13 (07) 271-273
- 5 Al-Attar N, Sedeek AF, McCall P, Travers J. Andexanet alfa in acute aortic syndrome: first UK experience. Eur J Cardiothorac Surg 2023; 63 (06) ezad100
- 6 Brenner B, Guerra J, Williams C. et al. Heparin insensitivity and thrombotic risk associated with sequential uses of prothrombin complex concentrate and andexanet alfa for apixaban reversal during acute type A aortic dissection repair: a case report. A A Pract 2022; 16 (11) e01636
- 7 Honda J, Itakura Y, Tanaka S, Inoue S. Successful use of an antithrombin for heparin resistance with andexanet alfa. JA Clin Rep 2023; 9 (01) 26
- 8 Kainz M, Bsuchner P, Schellongowski P, Dworschak M. Intraoperative off-label reversal of apixaban by andexanet alfa while on VA-ECMO immediately after emergent surgery for acute type A aortic dissection. J Cardiothorac Vasc Anesth 2021; 35 (01) 262-264
- 9 Henderson Jr RS, Deshpande S, Williams B, Taylor BS, Tanaka KA. Idarucizumab for dabigatran reversal in emergency type-A aortic dissection. J Cardiothorac Vasc Anesth 2017; 31 (06) e80-e81
- 10 Tomaszuk-Kazberuk A, Łopatowska P, Młodawska E, van Ryn J, Reilly PA, Pollack CV. Successful use of idarucizumab as a reversal agent for dabigatran in a patient with acute dissected aortic aneurysm. Pol Arch Intern Med 2017; 127 (01) 68-70
- 11 Mazur P, Darocha T, Filip G, Grudzień G, Drwiła R, Kapelak B. Idarucizumab for dabigatran reversal in patients with atrial fibrillation undergoing emergency surgery for acute aortic syndrome. Pol Arch Intern Med 2016; 126 (7–8): 579-581
- 12 Hamad R, Amr G, Demers P. Delayed surgery in patients with acute type A aortic dissection who are receiving novel oral anticoagulants. J Thorac Cardiovasc Surg 2018; 155 (01) e1-e4
- 13 Sromicki J, Van Hemelrijck M, Schmiady MO. et al. Prior intake of new oral anticoagulants adversely affects outcome following surgery for acute type A aortic dissection. Interact Cardiovasc Thorac Surg 2022; 35 (01) ivac037
- 14 Bjørnstad JL, Khan AM, Røed-Undlien H. et al. Operative survival in patients with acute aortic disease in the era of newer oral anticoagulants. Open Heart 2020; 7 (02) e001278
- 15 Beik N, Reddy P, Sylvester KW. et al. Andexanet alfa (Andexxa) formulary review. Crit Pathw Cardiol 2019; 18 (02) 66-71
- 16 Reed M, Tadi P, Nicolas D. Andexanet alfa. In: StatPearls. 2024. . Accessed February 20, 2024 at: http://www.ncbi.nlm.nih.gov/books/NBK519499/
- 17 van der Horst SFB, Martens ESL, den Exter PL. et al. Idarucizumab for dabigatran reversal: a systematic review and meta-analysis of indications and outcomes. Thromb Res 2023; 228: 21-32
- 18 European Medicines Agency. Ondexxya (andexanet alfa): avoid use of Andexanet prior to heparinization. 2020
- 19 Tibi P, McClure RS, Huang J. et al. STS/SCA/AmSECT/SABM update to the clinical practice guidelines on patient blood management. J Cardiothorac Vasc Anesth 2021; 35 (09) 2569-2591