
Subscribe to RSS
DOI: 10.1055/a-2505-9067
Intravaginal endoscopic vacuum therapy of a rectovaginal fistula: expanding boundaries

A 36-year-old woman underwent anterior resection of the rectum owing to endometriosis. The procedure was complicated by a rectovaginal fistula, which needed several surgical reinterventions. Despite diversion colostomy and reconstruction of the posterior vaginal wall with a fasciocutaneous flap, the rectovaginal fistula persisted, with a 50-mm abscess interposed between the coloanal anastomosis and the neovagina. The patient was referred for endoscopic evaluation.
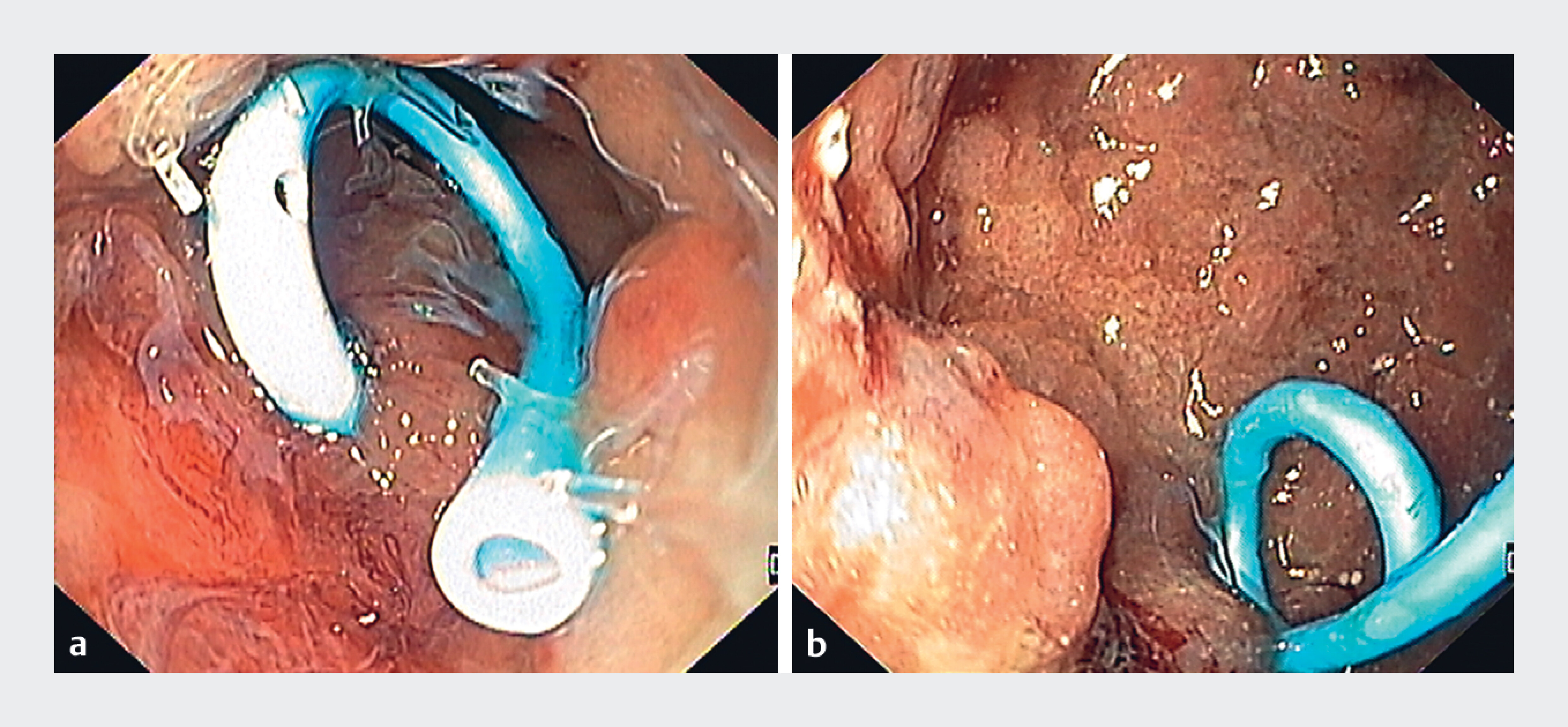
Endoscopy confirmed a 4-mm fistulous tract at the coloanal anastomosis with communication between the abscess and vagina. Two sessions of endoscopic internal drainage were performed ([Fig. 1] a); however, because of the lack of significant improvement in terms of the vaginal drainage and abscess dimensions, endoscopic intravaginal evaluation was performed, which revealed a 30-mm wide communication between the fornix and the abscess ([Fig. 1] b).
A total of seven sessions of intracavitary endoscopic vacuum therapy (EVT) were performed through the vagina ([Fig. 2] a), each 3–4 days apart, with progressive reduction of the cavity size ([Video 1]). Foreign bodies (surgical sutures/staples) were retrieved between the sessions to enhance tissue healing. At the end of the intravaginal EVT treatment, successful shrinkage of the cavity had been achieved, with a residual pseudodiverticulum ([Fig. 2] b). Because of the persistence of contrast extravasation from the rectum to the pseudodiverticulum on rectal evaluation, a 12/6t over-the-scope (OTS) clip was placed on the rectal side ([Fig. 2] c).

After 1 month, a double endoscopic evaluation (rectal and vaginal) was performed simultaneously, which showed OTS clip displacement, with no extravasation of contrast or methylene blue on either side. A computed tomography scan with rectal contrast and magnetic resonance imaging confirmed resolution of the fistula, with there being no recurrence during 12 months of follow-up.
Treatment of gastrointestinal fistulas frequently requires a multimodality approach, tailored to each phase of the healing process to enhance the possibility of clinical success [1] [2]. To the best of our knowledge, this is the first report of intravaginal EVT, highlighting the expanding applications of EVT in the treatment of surgical complications.
Endoscopy_UCTN_Code_TTT_1AQ_2AG
E-Videos is an open access online section of the journal Endoscopy, reporting on interesting cases and new techniques in gastroenterological endoscopy.
All papers include a high-quality video and are published with a Creative Commons
CC-BY license. Endoscopy E-Videos qualify for HINARI discounts and waivers and eligibility is automatically checked during the submission
process. We grant 100% waivers to articles whose corresponding authors are based in
Group A countries and 50% waivers to those who are based in Group B countries as classified
by Research4Life (see: https://www.research4life.org/access/eligibility/).
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Medas R, Rodrigues-Pinto E. Endoscopic treatment of upper gastrointestinal postsurgical leaks: a narrative review. Clin Endosc 2023; 56: 693-705
- 2 Loske G, Müller CT. Tips and tricks for endoscopic negative pressure therapy. Chirurg 2019; 90: 7-14
Correspondence
Publication History
Article published online:
16 January 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Medas R, Rodrigues-Pinto E. Endoscopic treatment of upper gastrointestinal postsurgical leaks: a narrative review. Clin Endosc 2023; 56: 693-705
- 2 Loske G, Müller CT. Tips and tricks for endoscopic negative pressure therapy. Chirurg 2019; 90: 7-14