
Subscribe to RSS
DOI: 10.1055/a-2058-8760
Colorectal self-expanding metal stent insertion using a small-caliber tapered transparent hood and electrolyte-free gel

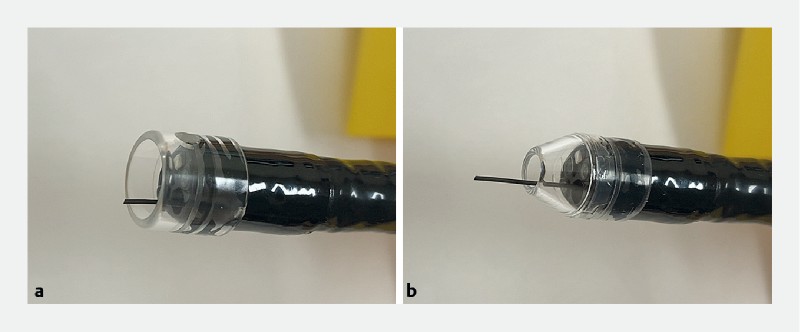
Colorectal self-expanding metal stent insertion is a useful procedure to treat acute colorectal obstruction caused by advanced colorectal cancer; however, guidewire perforation has been reported to occur as a result of inadequate endoscopic visibility [1] [2]. It is therefore important to maintain endoscopic visibility of the stricture to allow safe insertion of the colorectal stent. A method to maintain endoscopic visibility using an electrolyte-free gel (Viscoclear; Otsuka Pharmaceutical Factory) has recently been reported [3] [4]; however, it is difficult to maintain proper endoscopic visibility when the endoscopic hood has a large volume, as in the case of a conventional transparent hood. We previously reported a technique to obtain an appropriate field of view under saline immersion conditions using a calibrated, small-caliber tip, transparent hood (CAST hood; TOP, Tokyo, Japan) that has a tapered tip ([Fig. 1]) [5]. Herein, we report the use of a novel technique for colorectal stent insertion using this small-caliber tapered transparent hood and electrolyte-free gel ([Video 1]).
Video 1 Stent insertion to treat a colonic stricture using a small-caliber tapered transparent hood.
The patient was an 84-year-old woman with acute colorectal obstruction due to advanced colorectal cancer of the sigmoid colon. We inserted a colonic stent to decompress the obstruction. To maintain endoscopic visibility, a transparent hood was placed on the endoscope tip, and endoscopy was performed using an electrolyte-free gel; however, due to the severity of the stricture, endoscopic visualization with the standard hood was restricted ([Fig. 2 a]). The tapered tip of the new transparent hood limited the amount of blood that could enter the tip attachment, and appropriate endoscopic visibility was maintained using this hood with the gel ([Fig. 2 b]). Central stricture of the tumor was confirmed. A guidewire was placed through the colonic stricture from the oral side and a colonic stent was successfully inserted ([Fig. 2 c, d]).

Use of the small-caliber tapered transparent hood and gel is a reliable method to maintain adequate endoscopic vision and ensure safe colonic stent insertion.
Endoscopy_UCTN_Code_TTT_1AQ_2AF
E-Videos is an online section of the journal Endoscopy, reporting on interesting cases and new techniques in gastroenterological endoscopy.
All papers include a high-quality video and are published with a Creative Commons
CC-BY license. Endoscopy E-Videos qualify for HINARI discounts and waivers and eligibility is automatically checked during the submission
process. We grant 100% waivers to articles whose corresponding authors are based in
Group A countries and 50% waivers to those who are based in Group B countries as classified
by Research4Life (see: https://www.research4life.org/access/eligibility/).
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
#
Competing interests
The authors declare that they have no conflict of interest.
-
References
- 1 Arezzo A, Forcignanò E, Bonino MA. et al. Long-term oncologic results after stenting as a bridge to surgery versus emergency surgery for malignant left-sided colonic obstruction – a multicenter randomized controlled trial (ESCO trial). Ann Surg 2020; 272: 703-708
- 2 Arezzo A, Balague C, Targarona E. et al. Colonic stenting as a bridge to surgery versus emergency surgery for malignant colonic obstruction – results of a multicentre randomised controlled trial (ESCO trial). Surg Endosc 2017; 31: 3297-3305
- 3 Khurelbaatar T, Miura Y, Yano T. et al. Electrolyte-free gel immersion endoscopic submucosal dissection of gastric lesions. Endoscopy 2022; 54: E512-E513
- 4 Yano T, Ohata A, Hiraki Y. et al. Development of a gel dedicated to gel immersion endoscopy. Endosc Int Open 2021; 9: E918-E924
- 5 Nomura T, Sugimoto S, Oyamada J. et al. GI endoscopic submucosal dissection using a calibrated, small-caliber-tip, transparent hood for lesions with fibrosis. VideoGIE 2021; 6: 301-304
Corresponding author
Publication History
Article published online:
12 April 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Arezzo A, Forcignanò E, Bonino MA. et al. Long-term oncologic results after stenting as a bridge to surgery versus emergency surgery for malignant left-sided colonic obstruction – a multicenter randomized controlled trial (ESCO trial). Ann Surg 2020; 272: 703-708
- 2 Arezzo A, Balague C, Targarona E. et al. Colonic stenting as a bridge to surgery versus emergency surgery for malignant colonic obstruction – results of a multicentre randomised controlled trial (ESCO trial). Surg Endosc 2017; 31: 3297-3305
- 3 Khurelbaatar T, Miura Y, Yano T. et al. Electrolyte-free gel immersion endoscopic submucosal dissection of gastric lesions. Endoscopy 2022; 54: E512-E513
- 4 Yano T, Ohata A, Hiraki Y. et al. Development of a gel dedicated to gel immersion endoscopy. Endosc Int Open 2021; 9: E918-E924
- 5 Nomura T, Sugimoto S, Oyamada J. et al. GI endoscopic submucosal dissection using a calibrated, small-caliber-tip, transparent hood for lesions with fibrosis. VideoGIE 2021; 6: 301-304