

RSS-Feed abonnieren
DOI: 10.1055/a-1368-3796
Underwater endoscopic mucosal resection for a sporadic adenoma located at severe longitudinal ulcer scars in ulcerative colitis
Autoren

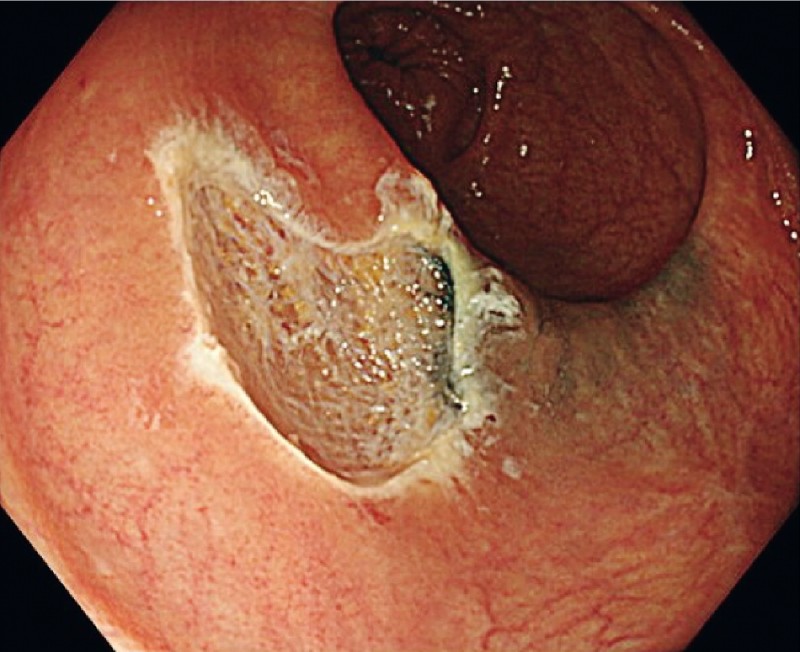
A 52-year-old woman diagnosed with ulcerative colitis (UC) and a history of repeated flare-ups and remissions was referred to our hospital. Colonoscopy revealed a 15-mm, flat elevated lesion in the transverse colon. Magnifying colonoscopy with narrow-band imaging (NBI) showed Japan NBI Expert Team classification type 2A and no flat dysplasia lesion in the periphery. Pathological findings of the biopsy specimen revealed a partial expression of p53. Based on these findings, we suspected sporadic adenoma ([Fig. 1]) rather than ulcerative colitis-associated neoplasia. There were obvious longitudinal ulcer scars as a result of UC inflammation and an endoscopic tattooing scar adjacent to the lesion ([Fig. 2]).


We decided to carry out underwater endoscopic mucosal resection (UEMR) for this lesion. After full immersion of the target lesion in natural saline, we captured it under NBI observation using a 20-mm snare (Snare Master; Olympus, Tokyo, Japan) ([Fig. 3]) and removed it. The procedure was completed without any visible neoplastic tissue on the margin of the mucosal defect ([Fig. 4]). En bloc resection without complications was achieved ([Fig. 5], [Video 1]). Histopathological examination revealed a low-grade tubular adenoma without tumor involvement on the horizontal and vertical margins.


Video 1 Underwater endoscopic mucosal resection for a sporadic adenoma located at severe longitudinal ulcer scars in ulcerative colitis.
Conventional endoscopic mucosal resection (EMR) of polyps on severe scars due to UC is technically challenging [1] because submucosal fibrosis from background inflammation makes it difficult to lift the lesion during submucosal injection and to snare the entire tumor. UEMR has been reported to be an effective technique in cases of severe submucosal fibrosis [2] [3] [4] [5], but it has not been performed in patients with UC after healing from inflammation. This report presents the first case of successful UEMR of a lesion associated with fibrosis secondary to UC remission and tattooing. UEMR may also be effective in resecting polyps on the fibrous mucosa within the area affected by UC.
Endoscopy_UCTN_Code_TTT_1AQ_2AD
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high
quality video and all contributions are
freely accessible online.
This section has its own submission
website at
https://mc.manuscriptcentral.com/e-videos
Competing interests
The authors declare that they have no conflict of interest.
-
References
- 1 Nishio M, Hirasawa K, Ozeki Y. et al. An endoscopic treatment strategy for superficial tumors in patients with ulcerative colitis. J Gastroenterol Hepatol 2020;
- 2 Hosotani K, Imai K, Hotta K. et al. Underwater endoscopic mucosal resection for complete R0 removal of a residual adenoma at a perforated scar in a patient with colostomy. Endoscopy 2017; 49: E121-E122
- 3 Takeuchi Y, Tonai Y, Ikeda K. Underwater endoscopic mucosal resection for a superficial polyp located at the anastomosis after surgical colectomy. Dig Endosc 2017; 29: 67-68
- 4 Rodrigues JP, Pinho R, Sousa M. et al. Underwater endoscopic mucosal resection of a laterally spreading tumor overlying a previous endoscopic carbon tattoo. Endoscopy 2018; 50: E231-E232
- 5 Kim HG, Thosani N, Banerjee S. et al. Underwater endoscopic mucosal resection for recurrences after previous piecemeal resection of colorectal polyps (with video). Gastrointest Endosc 2014; 80: 1094-1102
Corresponding author
Publikationsverlauf
Artikel online veröffentlicht:
22. Februar 2021
© 2021. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Nishio M, Hirasawa K, Ozeki Y. et al. An endoscopic treatment strategy for superficial tumors in patients with ulcerative colitis. J Gastroenterol Hepatol 2020;
- 2 Hosotani K, Imai K, Hotta K. et al. Underwater endoscopic mucosal resection for complete R0 removal of a residual adenoma at a perforated scar in a patient with colostomy. Endoscopy 2017; 49: E121-E122
- 3 Takeuchi Y, Tonai Y, Ikeda K. Underwater endoscopic mucosal resection for a superficial polyp located at the anastomosis after surgical colectomy. Dig Endosc 2017; 29: 67-68
- 4 Rodrigues JP, Pinho R, Sousa M. et al. Underwater endoscopic mucosal resection of a laterally spreading tumor overlying a previous endoscopic carbon tattoo. Endoscopy 2018; 50: E231-E232
- 5 Kim HG, Thosani N, Banerjee S. et al. Underwater endoscopic mucosal resection for recurrences after previous piecemeal resection of colorectal polyps (with video). Gastrointest Endosc 2014; 80: 1094-1102