Subscribe to RSS
DOI: 10.1055/s-0038-1641663
Comparing Complication Rates of Proximal versus Subsegmental/Distal Splenic Artery Coiling in Traumatic Splenic Injuries
Authors
Publication History
Publication Date:
22 March 2018 (online)

Purpose Splenic injuries are exceedingly common in the trauma setting and for hemodynamically stable patients who meet clinical criteria, splenic artery embolization (SAE) is considered the standard of care. Comparisons are often made between proximal splenic embolization and distal/selective embolization, with the latter being associated with higher incidence of infarction1 and minor complications.2 This study compares proximal versus distal/selective splenic artery coil embolization and the development of complications ([Fig. 1]).
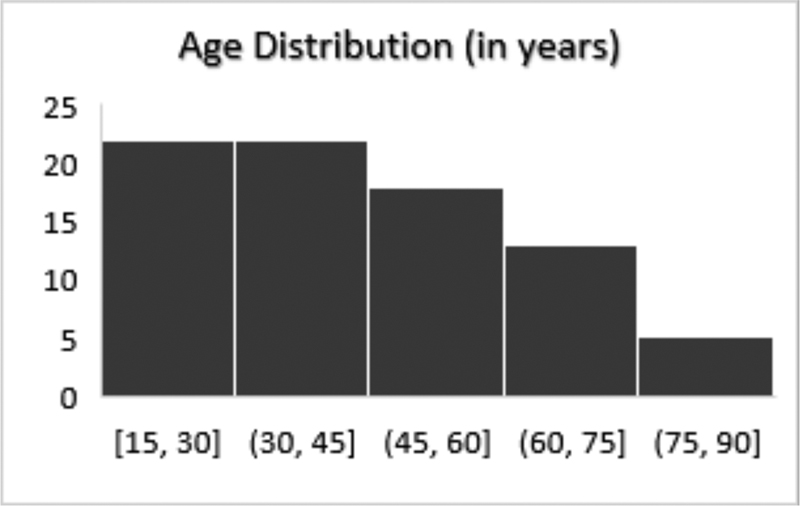
Materials and Methods A retrospective study was conducted obtaining a sample population of various American Association for the Surgery of Trauma (AAST) splenic injury grades from 2010 to 2017. The injuries ranged from grades I to V, all of which required SAE. Patients who were unable to be graded (lack of contrasted study, etc.) were excluded. Patients suffering non-survivable injuries were excluded from the study as well. In general, coiling occurred when active extravasation was identified on contrast-enhanced computed tomography (CT) or with dropping hematocrit (HCT) in the setting of splenic injury identified on CT. Patients were divided into subgroups depending on the AAST injury grade, location of embolization, polytrauma, age, and gender ([Table 1], [Fig. 2]). Using Current Procedural Terminology (CPT) codes and EPIC EMR search, various complications were studied including progression to surgical splenectomy, post-procedural abscess/phlegmon formation, time-to-discharge, and cause of readmission. Statistical significance was calculated using the Fischer’s exact test.
Results Coils were used for all embolizations (n = 80) with 77% placed in the proximal splenic artery and the remainder placed distally in segmental branches ([Figs. 1] and [3]). Embolic agents, such as Gelfoam or particles, were not used during splenic embolization in the trauma setting.
Ten percent (n = 8) of post-SAE patients eventually required a completion splenectomy. The progression to completion splenectomy was seen in two scenarios: (1) dropping HCT and (2) development of pain and abscess formation. The timing of splenectomy was bimodal, with dropping HCT resulting in splenectomy on approximately post-operative day (POD) 1.5, and pain/abscess occurring on POD 33. There was no correlation between progression to completion splenectomy and coil position (p > 0.05).
Five percent (n = 4) of post-SAE patients developed splenic abscesses. Two were treated by interventional radiology (IR) drainage ([Fig. 4]), and two were treated during open laparotomy, washout, and completion splenectomy. There was no correlation between coil position and abscess development (p > 0.05).
On average, patients were discharged 10.5 days after SAE. However, those with solitary splenic injuries (and no other injuries) had been inpatient for just 3.5 days. Patients with osseous fractures resulting in immobility stayed 15.5 days and those with traumatic brain injuries stayed on average 23.5 days. Eighty percent of patients were discharged home, and the remaining 20.0% were discharged to a skilled nursing facility. Patients who received proximal SAE had an average AAST grade of 3.4 (n = 60) and were discharged in 11.1 days. Patients who received distal SAE had an average AAST grade of 3.1 (n = 18) and were discharged in 8.4 days. Patients who had non-survivable injuries were excluded.
A total of 8.8% (n = 7) of all SAE patients required readmission. Causes for readmission included post-SAE abscess (n = 3), pain (n = 2), nausea/weakness (n = 1), and pleural effusion (n = 1).
Post-SAE pain after discharge was determined by complaints of left upper quadrant (LUQ) pain and requests for additional pain medications via telephone calls or at follow-up office visits. A small subset of patients who had isolated splenic injuries without any other injuries (n = 12) were selected. Patients who received a splenectomy during primary admission were also excluded from this group. Of the patients with proximal coiling (n = 9), 44.4% complained of pain (n = 4). Of patients with distal coiling (n = 3), 66.7% complained of pain (n = 2). There was no correlation between post-discharge pain and coil position (p > 0.05).
Conclusion This study compared proximal versus distal coiling and the resultant complications. Combined proximal and distal coiling was placed into the “distal” category ([Fig. 3]). It was assumed that the distal component would be the factor that increases complications, similar to how distal tissue level embolization has increased complications.1,2,3 Regardless, there was no difference between proximal or distal coiling and progression to completion splenectomy (10.0% of population) or abscess formation (5.0% of population). Although the exact mechanism of splenic trauma was extremely variable (from motor vehicle collision to trampled by bull), all patients could be placed in the category of blunt abdominal trauma ([Fig. 5]).
This study highlights the statistic that 10% of post-SAE patients required splenectomy. The most common reason to proceed to splenectomy was continually dropping hematocrit (HCT). All of these patients were evaluated angiographically during SAE, and none had persistent extravasation after coiling. In patients suffering from polytrauma, it is difficult to discern whether falling HCT is due to angiographically occult tissue level splenic bleeding or a result of other traumatic injuries. It raises the question whether these SAEs were truly failures, or perhaps the patients who progressed to the completion of splenectomy had the benefit of reduced bleeding and bridging to splenectomy in a more controlled, semi-elective environment.4
Conversely, 90% of patients had successful hemostasis after SAE and avoided splenectomy, preserving immunologic function and reducing infectious complications.3,5,7 In a literature review, SAE results in splenic salvage rates of 80 to 97%,7,8 which is concordant with our data.
As expected, confounding factors with trauma patients included polytrauma, traumatic brain injury, and long bone/hip fractures, all of which increased the duration of stay ([Table 1]). On average, patients were discharged 10.5 days after SAE, 2.5 days longer than the 8 days reported by Aiolfi et al.5 This can be attributed to the complicated nature of trauma patients, with solitary splenic injuries requiring a much shorter hospital stay than those with long bone/brain injuries (see results above).
Assessment of causation of pain in polytrauma patients is difficult. For example, of our patients with splenic injuries, 56% had overlying rib fractures, which are difficult to distinguish from splenic pain. Therefore, a small selected population of solitary splenic injuries (n = 12) was created to overcome this challenge. Proximal versus distal coiling did not affect post-SAE pain, assessed by the number of post-discharge telephone calls and requests for pain medications in follow up office visits (p > 0.05). Also note that this group contains lower AAST grade injuries than the sample population.
In conclusion, our study demonstrated no difference between proximal and distal/subsegmental splenic artery coil embolization, and the development of complications, including abscess, post procedural pain, or progression to splenectomy. With these considerations, interventionalists should choose the coiling position of their preference.
|
Variables |
Population |
|---|---|
|
Total |
n = 80 |
|
Age |
44 years (16–78) |
|
Sex |
|
|
Male |
54 (67.5%) |
|
Female |
26 (32.5%) |
|
AAST grades |
|
|
Grade I |
2 |
|
Grade II |
7 |
|
Grade III |
38 |
|
Grade IV |
31 |
|
Grade V |
2 |
|
Location of coil |
|
|
Proximal SA |
62 (77%) |
|
Distal SA |
18 (23%) |
|
Disposition |
|
|
Home |
62 (80%) |
|
Skilled nursing facility |
16 (20%) |
|
Associated injuries |
|
|
Rib fractures |
45 (56%) |
|
Leg/pelvic fracture |
23 (29%) |
|
Hemopneumothorax |
20 (25%) |
|
Spine fracture |
15 (19%) |
|
Additional abdominal organ injury |
15 (19%) |
|
Brain injury |
12 (15%) |