Keywords
Melanoma - Prognosis - Survival rate
INTRODUCTION
The poor prognosis of cutaneous malignant melanoma remains an important issue, and
many epidemiological studies have been conducted to identify factors that influence
the survival and prognosis of patients with malignant melanoma [1],[2],[3]. In particular, the possibility of the iatrogenic spread of tumor cells and the
resulting metastasis caused by the incisional biopsy of melanomas remains controversial.
The aim of this retrospective study was to evaluate the effect of the type of biopsy
on the metastatic rate and the prognosis of cutaneous melanoma in 81 patients who
were managed at our hospital during a 25-year period.
METHODS
The medical records of 109 patients with cutaneous malignant melanoma who were managed
at Tokushima University Hospital from 1983 to 2007 were reviewed. After excluding
28 cases with either stage 0 tumors (malignant melanoma in situ) or incomplete data, 81 cases were analyzed in detail with respect to patient age,
sex, tumor site, Union for International Cancer Control (UICC) TNM stage [4] at diagnosis, and prognosis.
The patients were divided into three groups (incisional, excisional, and no biopsy)
according to the presence/absence of biopsy and the type of biopsy performed. The
incisional biopsy group included punch biopsies. Of the 20 incisional biopsies, 19
were single biopsies, while 1 was taken from 3 separate points. The residual tumor
after an incisional biopsy was resected with a margin of 3 to 5 cm, and the defect
was covered with a skin graft or a skin flap within 2 to 3 weeks. The defect after
an excisional biopsy was temporarily covered with artificial dermis. In the "no biopsy"
group, a diagnosis was made on the basis of the gross appearance of the lesion and/or
dermoscopic findings, and a biopsy was not performed. Distal metastasis and local
recurrence were determined by physical examination and either computed tomography
or positron emission tomography. Excluding two cases with absent staging data, the
five-year survival rate of melanoma patients according to the clinical stage was calculated.
The clinical features of patients in the three biopsy groups were analyzed. The five-year
survival and five-year disease-free survival rates were calculated for each group.
The survival rates were determined and compared using the Kaplan-Meier method, log-rank
test, and Cox proportional hazard regression, using StatView ver. 5.0 for Windows
software (SAS Institute Japan Ltd., Tokyo, Japan). Other statistical analyses were
performed using Pearson's chi-squared test and analysis of variance, using the SPSS
ver. 21 (Japan IBM, Tokyo, Japan). The statistical significance level was set at P<0.05.
RESULTS
Of the 81 patients with malignant melanoma, 37 (45.7%) were male and 44 (54.3%) were
female. Their ages ranged from 19 to 93 years (mean, 61.6 years). The most common
tumor site was the lower extremity (54.3%) followed by the trunk (16%) ([Table 1]). The number and the percentage of patients according to the UICC stage are given
in [Table 2]. Stage I, II, and III tumors comprised 35.8%, 40.7%, and 21% of all cases, respectively.
Of all cases, 23.5% and 12.3% were stage IA and IB cases, respectively, while 16%,
16%, and 8.6% were stage IIA, IIB, and IIC cases, respectively. Of all cases, 3.7%,
11.1%, and 6.2% were stage IIIA, IIIB, and IIIC cases, respectively. The five-year
survival rates were 95.7%, 73.8%, and 39.2% for stage I, II, and III tumors, respectively
(P=0.0003) ([Fig. 1]).
Table 1.
Clinicopathologic features of cases in the three biopsy groups
|
Characteristic
|
Incisional (n = 20)
|
Excisional (n = 31)
|
No biopsy (n = 30)
|
Total (n = 81)
|
P-value
|
|
The P-values for sex and tumor site were calculated using Pearson’s chi-squared test
while those for age and Breslow thickness were calculated using analysis of variance.
|
|
Sex (n, %)
|
|
|
|
|
0.442
|
|
Male
|
7 (35.0)
|
14 (45.2)
|
16 (53.3)
|
37
|
|
|
Female
|
13 (65.0)
|
17 (54.8)
|
14 (46.7)
|
44
|
|
|
Age (yr)
|
|
|
|
|
0.139
|
|
Mean
|
66.3
|
57.2
|
62.9
|
61.6
|
|
|
Range
|
25–93
|
19–83
|
33–91
|
19–93
|
|
|
Site (n, %)
|
|
|
|
|
0.170
|
|
Head and neck
|
3 (15.0)
|
5 (16.1)
|
4 (13.3)
|
12 (14.8)
|
|
|
Upper extremity
|
4 (20.0)
|
5 (16.1)
|
3 (10.0)
|
12 (14.8)
|
|
|
Trunk
|
2 (10.0)
|
9 (29.0)
|
2 (6.7)
|
13 (16.0)
|
|
|
Lower extremity
|
11 (55.0)
|
12 (38.7)
|
21 (70.0)
|
44 (54.3)
|
|
|
Breslow thickness (mm)
|
|
|
|
|
0.092
|
|
Mean
|
2.94
|
2.29
|
3.59
|
2.93
|
|
|
Range
|
0.5–9.1
|
0.4–9.0
|
0.4–9.5
|
0.4–9.5
|
|
|
Ulceration (n, %)
|
9 (45)
|
7 (22.6)
|
14 (46.7)
|
30 (37.0)
|
0.105
|
|
Lymph node metastasis (n)
|
|
|
|
|
0.115
|
|
Positive
|
2
|
3
|
10
|
15
|
|
|
Negative
|
12
|
15
|
15
|
42
|
|
|
Not assessed
|
6
|
13
|
5
|
24
|
|
Table 2.
Clinical stage of cases in each biopsy group
|
Stage
|
I
|
II
|
III
|
Unknown
|
Total
|
|
Incisional biopsy
|
7
|
10
|
2
|
1
|
20
|
|
Excisional biopsy
|
14
|
12
|
5
|
0
|
31
|
|
No biopsy
|
8
|
11
|
10
|
1
|
30
|
|
Total (%)
|
29 (35.8)
|
33 (40.7)
|
17 (21.0)
|
2 (2.5)
|
81
|
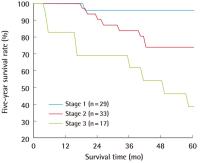 Fig. 1 Five-year survival rate according to clinical stage
P=0.0003. The P-value was calculated using the Kaplan-Meier method and log-rank test.
Fig. 1 Five-year survival rate according to clinical stage
P=0.0003. The P-value was calculated using the Kaplan-Meier method and log-rank test.
The incisional, excisional, and no biopsy groups contained 20, 31, and 30 patients,
respectively ([Table 1]). No significant differences among the three groups existed with respect to patient
age (P=0.139), sex (P=0.442), or tumor site (P=0.170). The mean Breslow thicknesses
were 2.94 mm, 2.29 mm, and 3.59 mm in the incisional, excisional, and no biopsy groups,
respectively. The number of patients with ulceration was 9, 7, and 14 in the incisional,
excisional, and no biopsy groups, respectively. The presence of lymph node metastasis
was diagnosed by either sentinel lymph node biopsy in 12 cases or lymph node dissection
in 45 cases, while neither was performed in the remaining 24 cases. Of the 57 cases
examined for lymph node metastasis, metastasis was found in 15 cases. No significant
differences in the mean Breslow thickness, ulceration, and lymph node metastasis were
observed among the groups (P=0.092, 0.105, and 0.115, respectively). The type or absence
of biopsy did not significantly affect the five-year survival rate (P=0.659) and the
five-year disease-free survival rate (P=0.153) ([Figs. 02]
[]). The median duration of follow-up was 61 months (range, 3-241 months). The hazard
ratios for five-year survival in the incisional and excisional biopsy groups were
1.11 (95% CI, 0.36-3.39) and 0.65 (95% CI, 0.21-2.00), respectively. The hazard ratios
for five-year disease-free survival in the incisional and excisional groups were 1.80
(95% CI, 0.72-4.55) and 0.69 (95% CI, 0.25-1.95), respectively.
 Fig. 2 The five-year survival rate in each biopsy group
P=0.6590. The P-value was calculated using the Kaplan-Meier method and log-rank test.
Fig. 2 The five-year survival rate in each biopsy group
P=0.6590. The P-value was calculated using the Kaplan-Meier method and log-rank test.
 Fig. 3 The five-year disease-free survival rate in each biopsy group
P=0.1535. The P-value was calculated using the Kaplan-Meier method and log-rank test.
Fig. 3 The five-year disease-free survival rate in each biopsy group
P=0.1535. The P-value was calculated using the Kaplan-Meier method and log-rank test.
DISCUSSION
Ishihara et al. [1] investigated 2,065 melanoma patients who were registered with the Prognosis and
Statistical Investigation Committee of the Japanese Skin Cancer Society during 1987
to 2001. The characteristics of patients in our study were similar to those in the
study conducted by Ishihara et al. [1] with respect to age, sex, tumor site, and clinical stage. They reported that the
five-year survival rates of patients with stage I, II, and III disease were 90%, 72%,
and 54%, respectively, which were similar to the survival rates obtained in our study.
Dermoscopy is helpful for the diagnosis of cutaneous malignant melanoma. However,
a pathologic examination of a biopsy of the lesion is required for a definitive diagnosis
and determination of the tumor thickness. The influence of the type of biopsy on the
patient outcome in melanoma, specifically, whether an incisional biopsy causes local
or systemic tumor dissemination, has been debated [5],[6],[7],[8]
[9]. Rampen et al. [5] reported a decreased survival rate in a group of 14 patients who had incisional
biopsies compared with that of 62 patients who had excisional biopsies. In a study
on head and neck melanomas, Austin et al. [6] reported a decreased survival rate among patients who had incisional, shave, or
needle aspiration biopsies compared with those who had excisional biopsies, although
a significant age difference was noted among the patient groups. Lederman and Sober
[7] reported no difference in survival between 119 patients with stage I melanoma who
had incisional biopsies and 353 who had excisional biopsies. Lees and Briggs [8] reported that the type of biopsy had no impact on local recurrence or survival in
1,086 cases of stage I melanoma. Bong et al. [9] reported that the type of biopsy had no significant effect on recurrence or melanoma-related
death rates in 265 and 496 melanoma cases that underwent incisional and excisional
biopsies, respectively, after controlling for patient age, sex, tumor site, and Breslow
thickness. The present study demonstrated that there were no significant differences
in the survival or metastatic rate among the three biopsy groups. Despite the small
number of patients in each group, no significant differences in the clinicopathological
features were observed among the groups. Because the biopsy method reportedly affects
the survival rate of patients with head and neck melanoma [6], the influence of biopsy type on survival might differ according to the tumor location
or other factors. More studies with a large patient population and longer follow-up
periods are necessary to explore this possibility.
An incisional biopsy can be performed under local anesthesia in an outpatient clinic
and is sufficient for diagnosing melanoma. However, an incisional biopsy provides
a small piece of tissue, so it is possible to underestimate the extent of tumor invasion.
Information on the depth of tumor invasion is essential in guiding surgical treatment
including the excision margin and lymph node dissection. Tumor depth can be determined
from an excisional biopsy but not from an incisional biopsy. An excisional biopsy
can also be performed under local anesthesia for small melanomas. However, general
anesthesia is required in the case of large melanomas, and the post-biopsy defect
requires wound coverage for pain and bleeding. Artificial dermis is an excellent option
for covering the wound after an excisional biopsy. Excisional biopsies of large melanomas
were difficult prior to the availability of artificial dermis for wound coverage.
In the present study, some patients in the no biopsy group underwent an excisional
biopsy because wound coverage using artificial dermis was not available at the time.
The use of incisional biopsies has generally been discouraged because it might affect
patient outcome. All patients in the no biopsy group were diagnosed with melanoma
based on typical clinical and/or dermoscopy findings.
The mechanism by which incisional biopsies increase the risk of melanoma metastasis
is unknown. Some researchers postulate that the release of fibroblast growth factors
during wound healing after a diagnostic incisional biopsy may promote melanoma progression.
Hofer et al. [10] found that fewer melanoma cells were needed to induce melanomas in rats with surgical
wounds and that the injection of early wound fluid increased the tumor size.
Our results are consistent with the opinion that the biopsy technique does not affect
the prognosis of melanoma patients. The use of incisional biopsies is generally discouraged
because accurate measurements of tumor thickness are not possible. As the type of
biopsy does not affect the melanoma recurrence rate or prognosis, we believe that
an incisional biopsy can be selected over an excisional biopsy if the clinical diagnosis
of melanoma is uncertain. An excisional biopsy (followed by wound coverage with artificial
dermis) is useful in guiding subsequent treatment because it reveals the thickness
of the tumor.




