

RSS-Feed abonnieren
DOI: 10.5935/1984-0063.20190052
Use of positional therapy when incorporated into a diagnosis-treatment algorithm for obstructive sleep apnea
Autor*innen

Purpose Positional obstructive sleep apnea (OSA) is prevalent. We hypothesized that by incorporating positional therapy into a diagnosis-treatment algorithm for OSA it would frequently be prescribed as an appropriate first-line therapy.
Methods Fifty-nine members (45 males, 49±9 yrs, BMI 35.2±5.6 kg/m2) of the Law Enforcement Health Benefits (LEHB), Inc. of Philadelphia with clinically suspected OSA were evaluated. Patients completed an Epworth Sleepiness Scale (ESS) questionnaire and a home sleep test (HST). Patients diagnosed with positional OSA (non-supine apnea-hypopnea index [AHI] < 5 events/hr) were offered positional therapy. A cost comparison to continuous positive airway pressure (CPAP) therapy was performed.
Results Fifty-four (92%) of the patients (43 males, 49±9 yrs, BMI 35.2±5.3 kg/m2) had OSA on their HST (AHI 24.2±20.1 events/hr). Sixteen (30%) patients had positional OSA. Compared to non-positional patients, patients with positional OSA were less heavy (32.4±5.1 vs. 36.4±5.1 kg/m2, respectively [p=0.009]), less sleepy (ESS 8±5 vs. 12±5, respectively [p=0.009]), and had less severe OSA (AHI 10.4±4.3 vs. 30.0±21.3 events/hr, respectively [p<0.001]). Thirteen of the 16 patients with positional OSA agreed to positional therapy and 31 non-positional OSA patients agreed to CPAP therapy. Based on initial costs, incorporating positional therapy ($189.95/device compared to CPAP therapy at $962.49/device) into the treatment algorithm resulted in a 24% cost savings compared to if all the patients were initiated on CPAP therapy.
Conclusion With the high prevalence of positional OSA, using a diagnosis-treatment algorithm that incorporates positional therapy allows it to be more frequently considered as a cost effective first-line therapy for OSA.
INTRODUCTION
Obstructive sleep apnea (OSA) syndrome is a disorder characterized by recurrent upper airway obstructive events during sleep in the presence of daytime sleepiness. Recent studies have demonstrated an increasing prevalence of OSA in the general population related to the worsening obesity epidemic[1]. Associated with the high prevalence of OSA is the large economic burden, with an estimated annual cost for the US healthcare system alone of up to $10 billion/year utilized for the diagnosis and treatment of OSA2. In addition, OSA has been associated with the development of significant cardiovascular disease when left untreated, which further adds to overall healthcare costs[2] - [6]. While CPAP therapy has been shown to improve daytime function as well as cardiovascular morbidity and mortality[7] - [9], compliance has been shown to be low, with compliance rates as low as 46% reported[10] , [11].
Positional OSA, where the majority of sleep disordered breathing events occur while in the supine position, has been reported to be present in up to 50-60% of all patients with diagnosed OSA[12] - [19]. Using a narrower definition of normalizing the apnea-hypopnea index (AHI) to < 5 events/hr when in the non-supine position, positional OSA is reported to be present in 27% of OSA patients[20]. While there are a number of positional devices designed to maintain patients with positional OSA in the non-supine position during sleep few have been compared to CPAP therapy[14] , [16] , [21]. We previously demonstrated that the use of positional therapy in these patients was as effective as CPAP therapy at normalizing the AHI[21].
While there have been studies examining the effectiveness, both in terms of diagnosis and cost, of utilizing a home sleep test (HST) vs. in-lab studies, no previous study has examined the effects of incorporating HST with a treatment algorithm that includes positional therapy for those patient diagnosed with positional OSA[22] - [26]. We hypothesized that incorporating positional therapy into a diagnosis-treatment algorithm for OSA would result in its frequent use as an appropriate first-line treatment with an associated cost savings as compared to CPAP therapy.
METHODS
Patient Selection
Patients selected for the study were all active members of Law Enforcement Health Benefits (LEHB) Inc., which oversees the healthcare benefits for the Philadelphia Police Department. Members and their spouses with symptoms suggestive of OSA were offered to participate in a study screening for OSA. All patients enrolled completed an Epworth Sleepiness Scale (ESS), which quantifies subjective measures of sleepiness by asking the subject to rate the chance of “dozing” in eight situations[27]. Patients with previously diagnosed OSA, shift workers, or those patients who refused to undergo a HST were excluded from the study. The study was approved by the Temple University School of Medicine Institutional Review Board for Human Research (Philadelphia, PA).
Home Sleep Test
The HSTs (Nox-T3, CareFusion Respiratory, Yorba Linda, Ca) were performed following the American Academy of Sleep Medicine Guidelines[28]. Studies were scored using established criteria[29] , [30]. Obstructive apneas were defined by the lack of airflow for greater than 10 seconds, associated with the presence of rib cage and abdominal movement[29]. Obstructive hypopneas were defined by a 30% decrease in airflow for greater than 10 seconds, associated with the presence of rib cage and abdominal movement, and accompanied by an oxygen desaturation of > 3%[29]. Apneas were defined as central if there was a lack of respiratory effort during the period of absent airflow[29]. The AHI (also referred to as the respiratory event index [REI]) was calculated as the number of apneic and hypopnic events per hour of recording time[29] , [30]. OSA was defined as an overall AHI of > 5 events/hr with symptoms of excessive daytime sleepiness or an AHI of > 15 events/hr[29]. Positional OSA was defined as a 50% decrease in the AHI in the non-supine position as compared to the supine position. Additionally, the AHI must fall to < 5 events/hr in the non-supine position, and the patient must have slept in the lateral position for a minimum of 1 hour during the study[20] , [21]. All of the HSTs were scored by the same author (SK).
Protocol
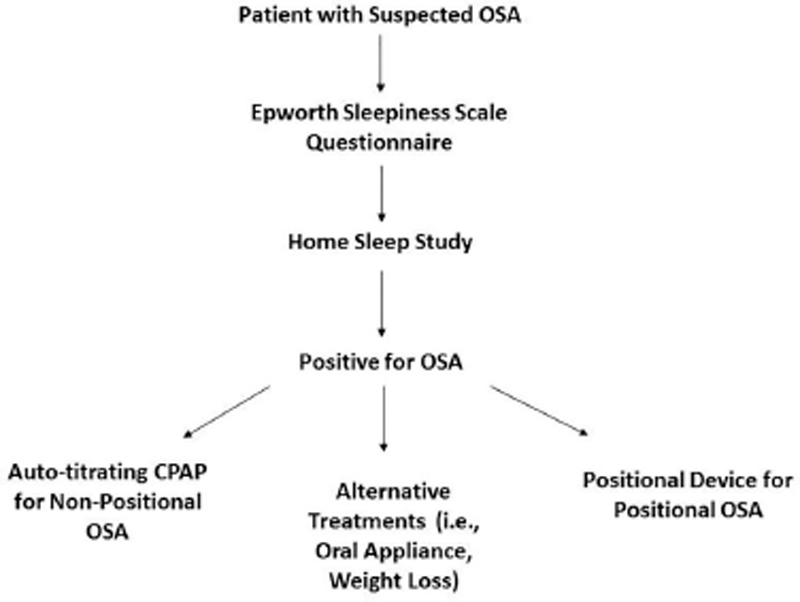
All patients enrolled for suspected OSA entered into a diagnostic and treatment algorithm that included an initial HST ([Figure 1]). If the HST was diagnostic for OSA then treatment options were discussed with the patient, including a trial on auto-titrating CPAP or if their study demonstrated positional OSA the use of the Zzoma Positional Device® (Sleep Specialists, LLC, Abington, PA)[21]. Other treatment options included the use of an oral appliance or conservative therapy with weight loss ([Figure 1]). Patients were instructed to follow-up in the Sleep Clinic or with their primary care physicians 4 weeks after initiating therapy.
Diagnostic and Therapeutic Costs
LEHB is a self-insured corporation with their healthcare management provided by Independent Blue Cross (IBC). Costs for initiating auto-titrating CPAP therapy ($962.49) in the home were based on IBC pricing for LEHB. Costs for the Zzoma Positional Device® ($189.95) were based on the suggested retail price at the time of the study.
Statistical Analysis
Data are displayed as the mean ± SD for continuous variables and the count and percentage for categorical variables. Comparisons between patients with and without positional OSA were performed using Fisher exact test or Wilcoxon rank-sum test. P-values < 0.05 were considered statistically significant. Therapy cost comparisons were determined based on the number of CPAP and positional devices that were distributed to the patients in the study. All statistical analyses were carried out using SAS V9.4 software (SAS Institute, Cary, NC).
RESULTS
Patient Characteristics
Fifty-nine patients (45 males, 49±9 yrs, BMI 35.2±5.6 kg/m2) with symptoms suggestive of OSA were enrolled into the study ([Table 1]). Fifty-four (92%) of the patients (43 males, 49±9 yrs, BMI 35.2±5.3 kg/m2) were found to have OSA on their HST (AHI 24.2 ±20.1 events/hr). Other than the AHI and the lowest SaO2 during the night, there were no significant differences between those patients with and without OSA ([Table 1]). Sixteen (30%) of the 54 patients with OSA were found to have positional OSA ([Table 2]). Patients with positional OSA were significantly less heavy and had significantly less severe OSA than those patients that were not positional; with a significantly lower AHI and significantly less severe nocturnal oxygen desaturation ([Table 2]). In addition, patients with positional OSA had significantly better objective sleep quality based on sleep efficiency, and subjectively were significantly less sleepy with a lower ESS as compared to those patients that were not positional ([Table 2]).
|
Variable |
All Patients (N=59) |
With OSA (N=54) |
Without OSA (N=5) |
p-value † |
|---|---|---|---|---|
|
Age, yrs |
49±9 |
49±9 |
49±7 |
0.95 |
|
Male, n (%) |
45 (76%) |
43 (80%) |
2 (40%) |
0.08 |
|
BMI, kg/m2 |
35.2±5.6 |
35.2±5.3 |
34.8±8.5 |
0.59 |
|
Epworth Sleepiness Scale* |
11±5 |
11±5 |
11±4 |
0.90 |
|
Heart Rate, beats/min* |
69±0 |
69±10 |
62±9 |
0.19 |
|
Recording Time Analyzed, min |
377±76 |
373±77 |
420±55 |
0.21 |
|
Sleep Efficiency, % |
87±16 |
86±17 |
94±6 |
0.30 |
|
Apnea-Hypopnea Index, events/hr |
22.4±20.1 |
24.2±20.1 |
3.0±1.7 |
<0.001 |
|
Mean SaO2, %* |
93±2 |
92±2 |
94±2 |
0.14 |
|
Lowest SaO2, %* |
79±8 |
79±8 |
85±9 |
0.04 |
|
Variable |
Without positional OSA (N=38) |
With positional OSA (N=16) |
p-value† |
|---|---|---|---|
|
Age, yrs |
50±9 |
47±8 |
0.30 |
|
Male, n (%) |
31 (82%) |
12 (75%) |
0.71 |
|
BMI, kg/m2 |
36.4±5.1 |
32.4±5.1 |
0.01 |
|
Epworth Sleepiness Scale* |
12±5 |
8±5 |
0.02 |
|
Recording Time Analyzed, min |
364±81 |
395±64 |
0.22 |
|
Sleep Efficiency, % |
83±18 |
93±8 |
0.01 |
|
Apnea-Hypopnea Index, events/hr |
30.0±21.3 |
10.4±4.3 |
< 0.001 |
|
Mean SaO2, %* |
92±3 |
93±1 |
0.05 |
|
Lowest SaO2, %* |
77±8 |
82±7 |
0.02 |
Therapy for Patients with OSA
The results of the HST and treatment options were discussed with each patient after their study was completed. Following the diagnosis and treatment algorithm ([Figure 1]), 13 of the 16 patients with positional OSA (24% of the patients with OSA) agreed to use the positional device with 1 patient requesting CPAP therapy and 2 patients requesting conservative therapy with weight loss ([Figure 2]). Thirty of the 38 patients who were not positional on their HST agreed to CPAP therapy, with the remaining 3 requesting an oral appliance and 5 requesting conservative treatment with weight loss. Therefore, a total of 31 patients (57% of the patients with OSA) received CPAP therapy ([Figure 2]). Patients treated with CPAP therapy had more severe OSA as compared to those patients treated with positional therapy or alternative treatments of using an oral appliance or weight loss ([Table 3]).

|
Variable |
CPAP Therapy (N=31) |
Positional Therapy (N=13) |
Alternative Treatments (N=10) |
p-value† |
|---|---|---|---|---|
|
Age, yrs |
49±10 |
47±9 |
52±6 |
0.32 |
|
Male, n (%) |
27 (87%) |
9 (69%) |
7 (70%) |
0.29 |
|
BMI, kg/m2 |
37.3±5.5 |
31.6±3.9 |
33.3±3.1 |
0.003 |
|
Epworth Sleepiness Scale* |
12±5 |
8±5 |
11±4 |
0.23 |
|
Heart Rate, beats/min* |
69±9 |
69±13 |
69±12 |
0.84 |
|
Recording Time Analyzed, min |
366±87 |
380±61 |
388±63 |
0.82 |
|
Sleep Efficiency, % |
82±20 |
93±9 |
90±8 |
0.06 |
|
Apnea-Hypopnea Index, events/hr |
34.5±21.1 |
10.8±4.5 |
9.8±4.4 |
<0.0001 |
|
Mean SaO2, %* |
92±3 |
93±1 |
93±2 |
0.30 |
|
Lowest SaO2, %* |
77±8 |
82±7 |
82±6 |
0.03 |
Cost Analysis
In regards to the cost comparison, for those patients that were treated for their OSA with CPAP therapy vs. positional therapy, based on an initial cost for an auto-titrating CPAP device of $962.49/unit the total cost for the 31 patients that received CPAP therapy was $29,837.19. With a cost of each positional device at $189.95, the total cost for the 13 patients that used the positional device was $2,469.35. When compared to a cost of $42,349.56 if all 44 patients had initially been treated with CPAP therapy, this represents a 24% cost savings by incorporating positional therapy into the treatment algorithm for OSA.
DISCUSSION
While there is a high prevalence of positional OSA and positional therapy has been shown to be an effective therapy for these patients, the prevalence of its initial use when incorporated into a diagnosis-treatment algorithm for OSA has not previously been reported[20] , [21]. There were 3 major findings in this study: 1) a structured algorithm can effectively be utilized to diagnose and treat patients with OSA, 2) there is high prevalence of positional OSA for which positional therapy is often accepted as an initial treatment, and 3) incorporating positional therapy into the treatment algorithm is associated with an overall lower cost as compared to CPAP therapy.
The prevalence of OSA has only been increasing in the general population, with the disorder now found in 14% of men and 5% of women[1]. These findings demonstrate a growth rate of 14-55% over the past 2 decades that is related to the rise in obesity[1]. Associated with the increasing prevalence of OSA are the costs associated with the diagnosis and treatment of the disorder[2]. On the diagnostic side, studies comparing the use of HST to in-lab testing have demonstrated similar rates of CPAP compliance and functional outcome[22] , [31] , [32]. In addition, home sleep testing has been shown to be associated with a noted cost savings[22] , [23]. Rosen et al.[22] demonstrated a 25% cost savings when HST followed by auto-titrating CPAP therapy was compared to in-lab polysomnogram followed by a CPAP titration study in patients with newly diagnosed OSA. The cost savings appeared to be more significant from the payer’s rather than the provider’s perspective[23]. In the present study, we incorporated the cost savings aspects of HST and auto-titrating CPAP therapy into the diagnosis and treatment algorithm. We found it to be efficient and diagnostically identified 92% of those who were tested as having OSA.
The reported prevalence of positional OSA at 27%, including 50% of patients with mild OSA and 19% of patients with moderate OSA, and the often low overall compliance rate with CPAP therapy demonstrates the importance of offering other forms of therapy, such as positional therapy, as an initial treatment option[10] , [11] , [20]. In the present study we found a similar prevalence, with 30% of patients overall having positional OSA, including 52% of patients with mild OSA and 20% of patients with moderate OSA. Most of these patients (81%) were treated with a positional device that was previously demonstrated to be equivalent to CPAP therapy at both normalizing the AHI to < 5 events/hr (92% vs. 97%, respectively) and improving nocturnal oxygenation in patients with positional OSA[21].
While our study was not designed as a cost analysis study we did note the initial cost savings associated with the use of positional therapy in our patients as compared to CPAP therapy. By incorporating positional therapy into the treatment algorithm for OSA we demonstrated an overall initial cost savings of 24% as compared to if these patients had been treated with CPAP therapy. Other forms of therapy, in particular oral appliances, have been evaluated in regards to their cost effectiveness in the treatment of OSA[24] - [26]. Sharples et al.[24] compared the clinical and cost effectiveness of oral appliances to CPAP therapy in a revised meta-analysis of patients with mild to moderate OSA. Clinically, CPAP was more effective than oral appliances at decreasing the AHI. In regards to costs, while CPAP produced a lower mean cost, when adjusted for a difference in compliance rates the authors suggested that oral appliances become less costly as compared to CPAP therapy[24]. In contrast, Sadatsafavi et al.[25] utilizing a model based analysis demonstrated that CPAP was more cost effective than oral appliances. However, oral appliances did show a cost savings when compared to conservative therapy[25]. More recently, Poullié et al.[26] reported that for patients with mild to moderate OSA and a high cardiovascular risk CPAP was more cost effective as compared to using an oral appliance. However, while the use of an oral appliance was more cost effective than CPAP in patients with a low cardiovascular risk the present out of pocket expense for an oral appliance may be cost prohibitive[26]. In our study only 3 patients elected to use an oral appliance and therefore the ability to evaluate the cost savings of using an oral appliance was limited. However, in countries where resources are limited, both in regards to costs and consistent home access to electricity, patients with diagnosed OSA may go untreated. With our findings demonstrating a similar prevalence of positional OSA as seen in other studies we believe the cost saving we observed with positional therapy can be applied to larger patient populations where a formal cost analysis could be performed[20].
There are limitations with the study that need to be addressed. First, the patients in the study were a select group of police officers and their spouses who had clinically suspected OSA. However, the prevalence of positional OSA is very similar to a previous study with similar patient characteristics[20]. Second, we did not compare the accuracy of HSTs that were used as part of the diagnostic component of the algorithm to in-lab polysomnograms. However, previous studies have already examined their accuracy and 92% of our patients were found to have OSA on their HST[22] , [31] , [32]. Finally, we did not evaluate more long-term outcomes as they relate to compliance with therapy and cost savings. However, the present study was designed to just evaluate the initial use when incorporating positional therapy into a diagnosis-treatment algorithm for OSA.
CONCLUSION
Use of a diagnosis-treatment algorithm for OSA that incorporates positional therapy demonstrates that positional OSA is prevalent and that positional therapy can often be prescribed as an appropriate first-line therapy and at a lower cost as compared to CPAP therapy. Whether larger studies that allow for a formal cost analysis will demonstrate similar or more substantial findings and whether more long-term use of positional therapy will reveal differences in compliance and functional outcome awaits further study.
Conflict of Interests
The authors have no conflict of interests to declare.
Acknowledgements: The authors would like to thank Donna Gimpel, RPSGT and Karen Nowelski, RPSGT for their help with the home sleep tests.
-
REFERENCES
- 1 Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hia KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9):1006-14.
- 2 McKinsey & Company. The price of fatigue: the surprising economic costs of unmanaged sleep apnea. Boston: Harvard Medical School; 2010
- 3 Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. Sleep Heart Health Study. JAMA. 2000;283(14):1829-36.
- 4 Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378-84.
- 5 Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353(19):2034-41.
- 6 Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Nieto FJ, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med. 2001;163(1):19-25.
- 7 George CF. Sleep. 5: Driving and automobile crashes in patients with obstructive sleep apnoea/hypopnoea syndrome. Thorax. 2004;59(9):804-7.
- 8 Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046-53.
- 9 Weaver TE, Maislin G, Dinges DF, Bloxham T, George CF, Greenberg H, et al. Relationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioning. Sleep. 2007;30(6):711-9.
- 10 Kribbs NB, Pack AI, Kline LR, Smith PL, Schwartz AR, Schubert NM, et al. Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis. 1993;147(4):887-95.
- 11 Wolkove N, Baltzan M, Kamel H, Dabrusin R, Palayew M. Long-term compliance with continuous positive airway pressure in patients with obstructive sleep apnea. Can Respir J. 2008;15(7):365-9.
- 12 Cartwright RD, Lloyd S, Lilie J, Kravitz H. Sleep position training as treatment for sleep apnea syndrome: a preliminary study. Sleep. 1985;8(2):87-94.
- 13 Cartwright R, Ristanovic R, Diaz F, Caldarelli D, Alder G. A comparative study of treatments for positional sleep apnea. Sleep. 1991;14(6):546-52.
- 14 Jokic R, Klimaszewski A, Crossley M, Sridhar G, Fitzpatrick MF. Positional treatment vs continuous positive airway pressure in patients with positional obstructive sleep apnea syndrome. Chest. 1999;115(3):771-81.
- 15 Kavey NB, Blitzer A, Gidro-Frank S, Korstanje K. Sleeping position and sleep apnea syndrome. Am J Otolaryngol. 1985;6(5):373-7.
- 16 Skinner MA, Kingshott RN, Filsell S, Taylor DR. Efficacy of the ‘tennis ball technique’ versus nCPAP in the management of position- dependent obstructive sleep apnoea syndrome. Respirology. 2008;13(5):708-15.
- 17 Oksenberg A, Silverberg DS, Arons E, Radwan H. Positional vs nonpositional obstructive sleep apnea patients: anthropomorphic, nocturnal polysomnographic, and multiple sleep latency test data. Chest. 1997;112(3):629-39.
- 18 Cartwright RD. Effect of sleep position on sleep apnea severity. Sleep. 1984;7(2):110-4.
- 19 Akita Y, Kawakatsu K, Hattori C, Hattori H, Suzuki K, Nishimura T. Posture of patients with sleep apnea during sleep. Acta Otolaryngol Suppl. 2003;(550):41-5.
- 20 Mador MJ, Kufel TJ, Magalang UJ, Rajesh SK, Watwe V, Grant BJ. Prevalence of positional sleep apnea in patients undergoing polysomnography. Chest. 2005;128(4):2130-7.
- 21 Permut I, Diaz-Abad M, Chatila W, Crocetti J, Gaughan JP, D’Alonzo GE, et al. Comparison of positional therapy to CPAP in patients with positional obstructive sleep apnea. J Clin Sleep Med. 2010;6(3):238-43.
- 22 Rosen CL, Auckley D, Benca R, Foldvary-Schaefer N, Iber C, Kapur V, et al. A multisite randomized trial of portable sleep studies and positive airway pressure autotitration versus laboratory-based polysomnography for the diagnosis and treatment of obstructive sleep apnea: the HomePAP study. Sleep. 2012;35(6):757-67.
- 23 Kim RD, Kapur VK, Redline-Bruch J, Rueschman M, Auckley DH, Benca RM, et al. An Economic Evaluation of Home Versus Laboratory- Based Diagnosis of Obstructive Sleep Apnea. Sleep. 2015;38(7):1027-37.
- 24 Sharples L, Glover M, Clutterbuck-James A, Bennett M, Jordan J, Chadwick R, et al. Clinical effectiveness and cost-effectiveness results from the randomised controlled Trial of Oral Mandibular Advancement Devices for Obstructive sleep apnoea-hypopnoea (TOMADO) and long-term economic analysis of oral devices and continuous positive airway pressure. Health Technol Assess. 2014;18(67):1-296.
- 25 Sadatsafavi M, Marra CA, Ayas NT, Stradling J, Fleetham J. Cost-effectiveness of oral appliances in the treatment of obstructive sleep apnoeahypopnoea. Sleep Breath. 2009;13(3):241-52.
- 26 Poullié AI, Cognet M, Gauthier A, Clementz M, Druais S, Späth HM, et al. Cost-effectiveness of treatments for mild-to-moderate obstructive sleep apnea in France. Int J Technol Assess Health Care. 2016;32(1-2):37-45.
- 27 Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-5.
- 28 Kapur VK, Auckley DH, Chowdhuri S, Kuhlmann DC, Mehra R, Ramar K, et al. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(3):479-504.
- 29 Berry RB, Brooks R, Gamaldo CE, Harding SM, Vaughn BV; American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, terminology and technical specifications, Version 2.0. Darien: American Academy of Sleep Medicine; 2012.
- 30 Collop NA, Tracy SL, Kapur V, Mehra R, Kuhlmann D, Fleishman SA. Obstructive sleep apnea devices for out-of-center (OOC) testing: technology evaluation. J Clin Sleep Med. 2011;7(5):531-48.
- 31 Berry RB, Hill G, Thompson L, McLaurin V. Portable monitoring and autotitration versus polysomnography for the diagnosis and treatment of sleep apnea. Sleep. 2008;31(10):1423-31.
- 32 Kuna ST, Gurubhagavatula I, Maislin G, Hin S, Hartwig KC, McCloskey S, et al. Noninferiority of functional outcome in ambulatory management of obstructive sleep apnea. Am J Respir Crit Care Med. 2011;183(9):1238-44.
Corresponding author:
Publikationsverlauf
Eingereicht: 25. Mai 2018
Angenommen: 27. November 2018
Artikel online veröffentlicht:
31. Oktober 2023
© 2023. Brazilian Sleep Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
REFERENCES
- 1 Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hia KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9):1006-14.
- 2 McKinsey & Company. The price of fatigue: the surprising economic costs of unmanaged sleep apnea. Boston: Harvard Medical School; 2010
- 3 Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. Sleep Heart Health Study. JAMA. 2000;283(14):1829-36.
- 4 Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378-84.
- 5 Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353(19):2034-41.
- 6 Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Nieto FJ, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med. 2001;163(1):19-25.
- 7 George CF. Sleep. 5: Driving and automobile crashes in patients with obstructive sleep apnoea/hypopnoea syndrome. Thorax. 2004;59(9):804-7.
- 8 Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046-53.
- 9 Weaver TE, Maislin G, Dinges DF, Bloxham T, George CF, Greenberg H, et al. Relationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioning. Sleep. 2007;30(6):711-9.
- 10 Kribbs NB, Pack AI, Kline LR, Smith PL, Schwartz AR, Schubert NM, et al. Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis. 1993;147(4):887-95.
- 11 Wolkove N, Baltzan M, Kamel H, Dabrusin R, Palayew M. Long-term compliance with continuous positive airway pressure in patients with obstructive sleep apnea. Can Respir J. 2008;15(7):365-9.
- 12 Cartwright RD, Lloyd S, Lilie J, Kravitz H. Sleep position training as treatment for sleep apnea syndrome: a preliminary study. Sleep. 1985;8(2):87-94.
- 13 Cartwright R, Ristanovic R, Diaz F, Caldarelli D, Alder G. A comparative study of treatments for positional sleep apnea. Sleep. 1991;14(6):546-52.
- 14 Jokic R, Klimaszewski A, Crossley M, Sridhar G, Fitzpatrick MF. Positional treatment vs continuous positive airway pressure in patients with positional obstructive sleep apnea syndrome. Chest. 1999;115(3):771-81.
- 15 Kavey NB, Blitzer A, Gidro-Frank S, Korstanje K. Sleeping position and sleep apnea syndrome. Am J Otolaryngol. 1985;6(5):373-7.
- 16 Skinner MA, Kingshott RN, Filsell S, Taylor DR. Efficacy of the ‘tennis ball technique’ versus nCPAP in the management of position- dependent obstructive sleep apnoea syndrome. Respirology. 2008;13(5):708-15.
- 17 Oksenberg A, Silverberg DS, Arons E, Radwan H. Positional vs nonpositional obstructive sleep apnea patients: anthropomorphic, nocturnal polysomnographic, and multiple sleep latency test data. Chest. 1997;112(3):629-39.
- 18 Cartwright RD. Effect of sleep position on sleep apnea severity. Sleep. 1984;7(2):110-4.
- 19 Akita Y, Kawakatsu K, Hattori C, Hattori H, Suzuki K, Nishimura T. Posture of patients with sleep apnea during sleep. Acta Otolaryngol Suppl. 2003;(550):41-5.
- 20 Mador MJ, Kufel TJ, Magalang UJ, Rajesh SK, Watwe V, Grant BJ. Prevalence of positional sleep apnea in patients undergoing polysomnography. Chest. 2005;128(4):2130-7.
- 21 Permut I, Diaz-Abad M, Chatila W, Crocetti J, Gaughan JP, D’Alonzo GE, et al. Comparison of positional therapy to CPAP in patients with positional obstructive sleep apnea. J Clin Sleep Med. 2010;6(3):238-43.
- 22 Rosen CL, Auckley D, Benca R, Foldvary-Schaefer N, Iber C, Kapur V, et al. A multisite randomized trial of portable sleep studies and positive airway pressure autotitration versus laboratory-based polysomnography for the diagnosis and treatment of obstructive sleep apnea: the HomePAP study. Sleep. 2012;35(6):757-67.
- 23 Kim RD, Kapur VK, Redline-Bruch J, Rueschman M, Auckley DH, Benca RM, et al. An Economic Evaluation of Home Versus Laboratory- Based Diagnosis of Obstructive Sleep Apnea. Sleep. 2015;38(7):1027-37.
- 24 Sharples L, Glover M, Clutterbuck-James A, Bennett M, Jordan J, Chadwick R, et al. Clinical effectiveness and cost-effectiveness results from the randomised controlled Trial of Oral Mandibular Advancement Devices for Obstructive sleep apnoea-hypopnoea (TOMADO) and long-term economic analysis of oral devices and continuous positive airway pressure. Health Technol Assess. 2014;18(67):1-296.
- 25 Sadatsafavi M, Marra CA, Ayas NT, Stradling J, Fleetham J. Cost-effectiveness of oral appliances in the treatment of obstructive sleep apnoeahypopnoea. Sleep Breath. 2009;13(3):241-52.
- 26 Poullié AI, Cognet M, Gauthier A, Clementz M, Druais S, Späth HM, et al. Cost-effectiveness of treatments for mild-to-moderate obstructive sleep apnea in France. Int J Technol Assess Health Care. 2016;32(1-2):37-45.
- 27 Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-5.
- 28 Kapur VK, Auckley DH, Chowdhuri S, Kuhlmann DC, Mehra R, Ramar K, et al. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(3):479-504.
- 29 Berry RB, Brooks R, Gamaldo CE, Harding SM, Vaughn BV; American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, terminology and technical specifications, Version 2.0. Darien: American Academy of Sleep Medicine; 2012.
- 30 Collop NA, Tracy SL, Kapur V, Mehra R, Kuhlmann D, Fleishman SA. Obstructive sleep apnea devices for out-of-center (OOC) testing: technology evaluation. J Clin Sleep Med. 2011;7(5):531-48.
- 31 Berry RB, Hill G, Thompson L, McLaurin V. Portable monitoring and autotitration versus polysomnography for the diagnosis and treatment of sleep apnea. Sleep. 2008;31(10):1423-31.
- 32 Kuna ST, Gurubhagavatula I, Maislin G, Hin S, Hartwig KC, McCloskey S, et al. Noninferiority of functional outcome in ambulatory management of obstructive sleep apnea. Am J Respir Crit Care Med. 2011;183(9):1238-44.