

Subscribe to RSS
DOI: 10.4103/wjnm.WJNM_83_19
Solitary metastatic deposit in the mandible from follicular thyroid carcinoma
Authors


Abstract
Follicular thyroid carcinoma (FTC) is the second most common cancer of the thyroid, after papillary carcinoma. Oral metastasis arising from FTC is very rare. Mandible is more commonly affected than maxilla, with the premolar—molar region being the most frequent site of metastasis. We present the case of a 68yearold female, with swelling in the region of the parotid gland, complaining of periodic rightsided pain in the temporomandibular joint, which occurred most often in the morning with numbness and pain, and difficulty in opening the mouth. After ultrasound and X-ray, the patient was operated and the pathohistological finding was in favor of metastasis of FTC. After 3 months, a total thyroidectomy was performed, and FTC was detected in the right thyroid lobe. Laboratory results were as follows: FT4 = 9.92 pmol/L, thyroid-stimulating hormone = 9.9 mIU/L, and hTG >300 μg/L. Bone scan showed no bone metastasis. Radioablation with 131I of 150 mCi was given to the patient, followed by substitutional therapy with levothyroxine. Mandible metastasis as a single skeletal deposit from follicular thyroid carcinomas is a rare clinical finding. Maxillofacial surgeons should consider and rule out thyroid pathology before performing operation of tumor formation in the mandible region. If feasible, surgical-based treatment options offer the best survival outcomes.
Introduction
Follicular thyroid carcinoma (FTC) is a well-differentiated tumor which originates in follicular cells and resembles the normal microscopic pattern of the thyroid. It is the second most common cancer of the thyroid, after papillary carcinoma.[1],[2] Oral metastasis arising from FTC is very rare. The other reported sites in the oral region are parotid gland, tongue, and labial mucosa. Mandible is more commonly affected than maxilla, with the premolar-molar region being the most frequent site of metastasis.[3],[4]
Case Report
We present the case of a 68yearold female patient, with swelling in the region of the parotid gland, complaining of periodic rightsided pain in the temporomandibular joint that occurred most often in the morning with numbness, pain, and difficulty in opening the mouth. A written informed contest was obtained from the patient. These symptoms occurred at certain months of the year, especially in winter, and lasted almost 1 year. In the right parotid region at the level of the outer ear canal, a limited, hard, painful swelling was palpated, which was noticed 2 weeks ago. Laboratory findings were as follows: sedimentation rate = 26; leukocytes = 7,8; Creactive protein = positive; and reuma factor = negative. The treatment started with antibiotic and anti-inflammatory therapy. Ultrasound (US) and X-ray were suggested.
The first X-ray detected neat pneumatization of mastoid cells bilaterally. The right temporomandibular joint with closed mouth showed normal findings of the articular surfaces. There was a well movement with open mouth with condylar contact and articular eminence. US of the mandible showed an oval, well-defined, vascularized, hypoechoic tumor formation (20 mm × 22 mm) preauriculary in the front aspect of the parotid gland. No significant enlarged lymph nodes were detected. The described change was in favor of the right parotid gland adenoma. Computed tomography (CT) revealed expansive soft-tissue tumor formation in the projection of the right condylar processes, with a diameter of 30 mm, with destruction of the skeleton, infiltrating the masticator and the right parotid gland (differential diagnosis — metastasis of unknown origin). The mass infiltrated the right temporal bone, as well as the articular fossa of the right temporomandibular joint. In the projection of the anterior group of the ethmoidal cells, a soft-tissue polypus mass was seen that destroyed the skeletal structure. In the right thyroid lobe, calcified nodule was present with a diameter of 20 mm [Figure 1] and [Figure 2].


After an aspiration biopsy was performed, a diagnosis of Carcinoma of the right parotic gland was made, and the patient was operated (2 months after) Total parotidectomy was performed with resection of the ramus of the right mandible. The patient was prescribed analgesics and vitamin supportive therapy. The pathohistological finding showed metastasis from a follicular thyroid carcinoma. Microscopically, malignant epithelial neoplasm was detected, with predominant follicular trabecular architecture, round-to-oval cells, with eosinophilic cytoplasm and hyperchromic nuclei, and irregular chromatin distribution. Vascular invasion of the tumor was confirmed with positivity of CD34. Imunohistochemistry revealed TTF+, Tg+, CKAE1/AE3+, CD56+, actin (−), CK19 (focal positivity), proliferative index 10%, and chromogranin (low positivity).
After 3 months, a total thyroidectomy was performed. Microscopically dark brown encapsulated fragments of lobes were resected; left lobe with dimension 35 mm × 15 mm × 10 mm and right lobe with dimension 60 mm × 55 mm × 50 mm, total parotidectomy was performed with resection of the ramus of the right mandible. Microscopically, left lobe showed benign thyroid follicle, whereas in the right lobe, a structure of well-differentiated FTCwas identified, with multiple densely packed cells with hyperchromatic nuclei, scarce eosinophilic cytoplasm, arranged in nests, separated by bundles of mature connective tissue. Peripheral encapsulated tumour was found, with capsule invasion and emboluses in the blood vessels. pTNM = pT3 pN0 pM1 G1 Cx NG1 Stage IV.
The patient was admitted at our department for further treatment. US detected remnant thyroid tissue bilaterally, right remnant thyroid tissue of 25 mm, and left remnant thyroid tissue of 20 mm, confirmed with the thyroid pertechnetate scan. Laboratory findings were as follows: FT4 =9.92 pmol/L, thyroid-stimulating hormone (TSH) = 9.9 mIU/L, and hTG >300 (<50 μg/L). The patient refused reoperation. Investigation of the lungs (CT) and abdomen (US) showed no pathological changes. 99mTc-MIBI scan of the whole body was performed, with asymmetry in the parotid glands (left with normal accumulation and right without accumulation due to the resection), and no other focal accumulation in favor of metastasis was detected. Bone scan showed no bone metastasis [Figure 3].

Radioablation with 131I of 150 mCi was given to the patient, 3 months after the total thyroidectomy, and a substitutional therapy was started with levothyroxine. The postablative scan [Figure 4] showed intensive uptake of the radioiodine in the remnant thyroid bed, as well as in the right mandible. Hence, our conclusion was that there was a solitary metastasis in the right mandible, infiltrating the right parotid gland.
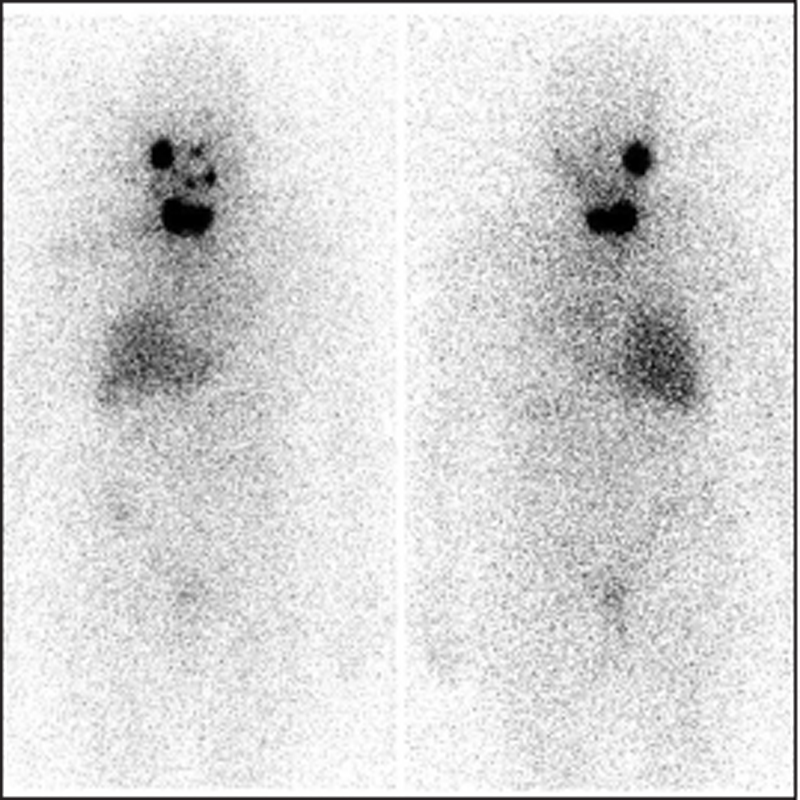
Because of persistently high hTG value >300 μg/L, another dose of radioiodine was given (100 mCi) 8 months after the first radioidine therapeutic dose, and the postablative radioiodine scan detected no new accumulation of radioiodine and showed less intensive accumulation in the mandibular region [Figure 5].

The control CT scan detected predominantly osteosclerotic lesion 10 mm × 8 mm in the posterior aspect of corpus mandibulae on the left side, without cortical or associated periosteal reaction.
At the last control checkup, the patient still complained on occasional pain on the right side of the mandible. The oropharyngeal finding was normal. The otolaryngologist advised further treatment with analgesics and vitamin supportive therapy. Thyroid status, under substitution therapy with L-thyroxine of 150 μg/day, was FT4 =31 pmol/L, TSH = 0.072 mIU/L, aTG <20 kIU/L, and hTG = 195 (<50 μg/L). US showed no enlarged neck lymph nodes. She still complained of some pain in the mandibular region.18 F-labeled fluoro-2-deoxyglucose positron emission tomography scan will be planned as further diagnostic imaging modality, and external beam radiation of the mandible will be considered as a further treatment option.
Discussion
Although distant metastasis of well-differentiated thyroid carcinomas occurs in 10% —15% of patients, the percentage of bone metastasis is very low (1% — 3%), FTCs are more often associated with bone metastasis, usually present in patients older than 40 years of age.[5] When patient is complaining of jaw pain, swelling, loosening of the tooth, numb chin, or mental nerve neuropathy, a clinician should always raise the possibility of a metastatic disease in the mandible. A peculiar site for metastasis is the postextraction site.[4] Metastatic lesions may mimic odontogenic infections or other conditions in the oral cavity, leading to late diagnosis. In 10%—15% of cases, FTC will disseminate hematogenously via angioinvasion. Thyroid malignancy represents 4.2%—6.1% of all jaw metastases; 41% of them occur in the mandible.[6] In the article by Varadarajan et al., the authors summarized 41 reported cases in the literature of thyroid malignancy with metastasis to the mandible, of which 21 reported cases were FTC and from six reported cases of metastasis to the maxilla, two were FTC.[7]
We present a case in which the metastatic lesion of the right mandible was detected before diagnosis of primary thyroid malignancy.
An oval swelling, spontaneously bleeding mass, appeared in a 40-year-old female, after extraction of molars. CT showed destroying the posterior region of body and ramus of the left mandible, 45 mm × 45 mm in size. The patient gave information of cleaning her teeth with mishri (fine black powder of roasted tobacco leaves) over the last 30—35 years. The patient informed about the existing thyroid nodule, 35 mm × 30 mm in size, 4 months before.[8]
In another study, it was found that in 55 cases, tooth extraction preceded the discovery of metastasis. In the majority of the cases, a latency period of 2 months between the extraction and the development of the metastasis was reported. In our case also, we observed a similar finding. Thus, the role of trauma to the oral mucosa in the causation of oral metastasis needs further investigation.[9]
Varadarajan et al. published a case report of a FTC in a female patient, metastasized in mandible (5 cm aggressive mass), as well as enlarged pulmonary nodules and a lytic bone lesion at Th10. Thyroid US revealed enlarged multinodular goiter. The patient underwent total thyroidectomy and was further treated with 200 mCi of radioiodine and stereotactic body radiation to the Th10 metastatic lesion. She had been disease free for 18 months.[7]
Another case of a female patient, 71 years old, was described with a CT scan that showed a lesion of the left body of mandible extending from the lower left canine region to second molar region with diffuse margin, leaving the lower border intact. Afterward, a thyroid nodule as well as enlarged hilar lymph nodes was detected.[10]
Vural and Hanna concluded from their studies that the ramus and angle are more commonly involved, which is due to their better vascularity.[11] Other investigators discussed the possible causes of jaw metastasis, via hematological pathways; some report the presence of hematopoietic active bone marrow well connected with the sinusoidal vascular spaces at the site of deposition of malignant cells, whereas others believe that that the reason is the high bone turnover in this region.[12],[13],[14]
The case of Pasupula described a female patient, 40 years of age, who presented with a swelling involving the left posterior mandible. Radiography showed extensive lytic lesion involving the ramus, up to the condyle. Further US of the thyroid showed the presence of two nodules, with fine-needle aspiration biopsy in favor of a follicular neoplasm. Histopathologically, FTC was confirmed with metastasis in the mandible.[15]
A 56-year-old female patient presented with a solitary, oval, nonpainful swelling on the right side of the lower face, 63 mm × 50 mm, of 6-month duration, associated with paresthesia of the lower lip and body of the mandible. The biopsy detected an odontogenic tumor. US of the right thyroid gland revealed a solitary, hypoechoic, 15 mm × 10-mm nodule. Metastasis to other parts of the body was excluded by a whole-body scan. The serum hTG level was elevated to 480 ng/ml.[16] It is thought that skeletal metastasis has a poorer survival rate than lung metastasis. However, there is some evidence indicating that resection of a solitary bony metastasis, along with a total thyroidectomy, may provide better survival.[17]
Conclusion
Mandible metastasis as a single skeletal deposit from FTC is a rare clinical finding. Maxillofacial surgeons have to consider the possibility of metastatic thyroid tumor involvement of mandible and include thyroid checkup before operation of tumor formation in the mandible region. If feasible, surgical-based treatment options offer the best survival outcomes.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Schlumberger M, Pacini F, Tutle RM. Thyroid Tumors. 4th ed. Paris: Institute Medico-Educatif; 2015.
- 2 Sobrinho-Simo˜es M, Eloy C, Magalhães J, Lobo C, Amaro T. Follicular thyroid carcinoma. Mod Pathol 2011;24:S10-8.
- 3 Lim SY, Kim SA, Ahn SG, Kim HK, Kim SG, Hwang HK, et al. Metastatic tumours to the jaws and oral soft tissues: A retrospective analysis of 41 Korean patients. Int J Oral Maxillofac Surg 2006;35:412-5.
- 4 van der Waal RI, Buter J, van der Waal I. Oral metastases: Report of 24 cases. Br J Oral Maxillofac Surg 2003;41:3-6.
- 5 Mizukami Y, Michigishi T, Nonomura A, Hashimoto T, Terahata S, Noguchi M, et al. Distant metastases in differentiated thyroid carcinomas: A clinical and pathologic study. Hum Pathol 1990;21:283-90.
- 6 Hirshberg A, Berger R, Allon I, Kaplan I. Metastatic tumors to the jaws and mouth. Head Neck Pathol 2014;8:463-74.
- 7 Varadarajan VV, Pace EK, Patel V, Sawhney R, Amdur RJ, Dziegielewski PT. Follicular thyroid carcinoma metastasis to the facial skeleton: A systematic review. BMC Cancer 2017;17:225.
- 8 Bhadage CJ, Vaishampayan S, Umarji H. Mandibular metastasis in a patient with follicular carcinoma of thyroid. Contemp Clin Dent 2012;3:212-4.
- 9 Hirshberg A, Leibovich P, Horowitz I, Buchner A. Metastatic tumors to postextraction sites. J Oral Maxillofac Surg 1993;51:1334-7.
- 10 Ismail SB, Abraham MT, Zaini ZB, Yaacob HB, Zain RB. Metastatic follicular thyroid carcinoma to the mandible: A case report. Cases J 2009;2:6533.
- 11 Vural E, Hanna E. Metastatic follicular thyroid carcinoma to the mandible: A case report and review of the literature. Am J Otolaryngol 1998;19:198-202.
- 12 Hashimoto N, Kurihara K, Yamasaki H, Ohba S, Sakai H, Yoshida S. Pathological characteristics of metastatic carcinoma in the human mandible. J Oral Pathol 1987;16:362-7.
- 13 Standish SM, Shafer WG. Focal osteoporotic bone marrow defects of the jaws. J Oral Surg Anesth Hosp Dent Serv 1962;20:123-8.
- 14 D'Silva NJ, Summerlin DJ, Cordell KG, Abdelsayed RA, Tomich CE, Hanks CT, et al. Metastatic tumors in the jaws: A retrospective study of 114 cases. J Am Dent Assoc 2006;137:1667-72.
- 15 Pasupula AP, Dorankula SP, Thokala MR, Kumar MP. Metastatic follicular thyroid carcinoma to the mandible. Indian J Dent Res 2012;23:843.
- 16 Vishveshwaraiah PM, Mukunda A, Laxminarayana KK, Kasim K. Metastatic follicular thyroid carcinoma to the body of the mandible mimicking an odontogenic tumor. J Cancer Res Ther 2013;9:320-3.
- 17 Ostrosky A, Mareso EA, Klurfan FJ, Gonzalez MJ. Mandibular metastasis of follicular thyroid carcinoma. Case report. Med Oral 2003;8:224-7.
Address for correspondence
Publication History
Received: 08 November 2019
Accepted: 29 January 2020
Article published online:
19 April 2022
© 2020. Sociedade Brasileira de Neurocirurgia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Schlumberger M, Pacini F, Tutle RM. Thyroid Tumors. 4th ed. Paris: Institute Medico-Educatif; 2015.
- 2 Sobrinho-Simo˜es M, Eloy C, Magalhães J, Lobo C, Amaro T. Follicular thyroid carcinoma. Mod Pathol 2011;24:S10-8.
- 3 Lim SY, Kim SA, Ahn SG, Kim HK, Kim SG, Hwang HK, et al. Metastatic tumours to the jaws and oral soft tissues: A retrospective analysis of 41 Korean patients. Int J Oral Maxillofac Surg 2006;35:412-5.
- 4 van der Waal RI, Buter J, van der Waal I. Oral metastases: Report of 24 cases. Br J Oral Maxillofac Surg 2003;41:3-6.
- 5 Mizukami Y, Michigishi T, Nonomura A, Hashimoto T, Terahata S, Noguchi M, et al. Distant metastases in differentiated thyroid carcinomas: A clinical and pathologic study. Hum Pathol 1990;21:283-90.
- 6 Hirshberg A, Berger R, Allon I, Kaplan I. Metastatic tumors to the jaws and mouth. Head Neck Pathol 2014;8:463-74.
- 7 Varadarajan VV, Pace EK, Patel V, Sawhney R, Amdur RJ, Dziegielewski PT. Follicular thyroid carcinoma metastasis to the facial skeleton: A systematic review. BMC Cancer 2017;17:225.
- 8 Bhadage CJ, Vaishampayan S, Umarji H. Mandibular metastasis in a patient with follicular carcinoma of thyroid. Contemp Clin Dent 2012;3:212-4.
- 9 Hirshberg A, Leibovich P, Horowitz I, Buchner A. Metastatic tumors to postextraction sites. J Oral Maxillofac Surg 1993;51:1334-7.
- 10 Ismail SB, Abraham MT, Zaini ZB, Yaacob HB, Zain RB. Metastatic follicular thyroid carcinoma to the mandible: A case report. Cases J 2009;2:6533.
- 11 Vural E, Hanna E. Metastatic follicular thyroid carcinoma to the mandible: A case report and review of the literature. Am J Otolaryngol 1998;19:198-202.
- 12 Hashimoto N, Kurihara K, Yamasaki H, Ohba S, Sakai H, Yoshida S. Pathological characteristics of metastatic carcinoma in the human mandible. J Oral Pathol 1987;16:362-7.
- 13 Standish SM, Shafer WG. Focal osteoporotic bone marrow defects of the jaws. J Oral Surg Anesth Hosp Dent Serv 1962;20:123-8.
- 14 D'Silva NJ, Summerlin DJ, Cordell KG, Abdelsayed RA, Tomich CE, Hanks CT, et al. Metastatic tumors in the jaws: A retrospective study of 114 cases. J Am Dent Assoc 2006;137:1667-72.
- 15 Pasupula AP, Dorankula SP, Thokala MR, Kumar MP. Metastatic follicular thyroid carcinoma to the mandible. Indian J Dent Res 2012;23:843.
- 16 Vishveshwaraiah PM, Mukunda A, Laxminarayana KK, Kasim K. Metastatic follicular thyroid carcinoma to the body of the mandible mimicking an odontogenic tumor. J Cancer Res Ther 2013;9:320-3.
- 17 Ostrosky A, Mareso EA, Klurfan FJ, Gonzalez MJ. Mandibular metastasis of follicular thyroid carcinoma. Case report. Med Oral 2003;8:224-7.