

Subscribe to RSS
DOI: 10.4103/jnacc-jnacc-3.17
A comparative study between intraoperativelow-dose ketamine and dexmedetomidine, as an anaesthetic adjuvant in lumbar spine instrumentation surgery for the post-operative analgesic requirement
Authors
Address for correspondence:
Publication History
Publication Date:
08 May 2018 (online)


Abstract
Background: Spinal instrumentation and fusion surgery presents the anaesthesiologist with multiple issues like intraoperative blood loss, hemodynamic changes, prolonged surgery etc, but the most probing aspect is analgesia. While both ketamine and dexmedetomidine as adjuvants have shown to decrease intraoperative anaesthetics and post operative analgesic consumption but there are no comparative studies. The primary aim of this study was comparison of post-operative analgesic requirements for 1st 24 hours after surgery when either of the drugs was used as adjuvants. Methods: Adult patients aged 18-60 years, of either sex, and ASA status I or II scheduled for elective lumbar spine instrumentation (of 2 or more spinal levels) surgery were enrolled for the study. Patients were randomised into one of the 3 treatment regimens ketamine/group K (0.5mg/kg bolus followed by 250 mcg/kg/h infusion), dexmedetomidine/ group D (0.5mcg/kg bolus followed by 0.5 mcg/kg/h infusion) or the placebo/ group S (saline/placebo). The study drugs were started after turning the patient prone. Data were recorded for intraoperative hemodynamics, anesthetic consumption (inhalational agent and opioids), emergence through RAS scale (Riker sedation agitation scale), PCA (patient controlled analgesia)-fentanyl use and VAS (visual analog scale) score in the 1st 24 hours after surgery. Appropriate statistical analysis was done. Results: A total of 42 patients (14 in each group) were enrolled. The total PCA fentanyl consumed in first 24 hours of surgery was maximum with the group-S (1366.6±382.6 mcg) in compared with group- D (1035.4±391.8 mcg) and group- K (1164.9±503.6 mcg) (P=0.13). The post extubation RAS score was lower in group-K (3.7±0.6) when compared with group-D (4±0.4) and group-S (4.5±0.9) (P=.009). Total intraoperative sevoflurane and fentanyl consumption showed no difference (P=0.19 and P=0.28). VAS score at rest was higher at baseline with group-S (P=0.009). The ICU stay was comparable (group-D: 1.4±0.5 d, group-K: 1.5±0.5 d, group-S: 1.9±0.5 d) among the groups. Hospital stay was also comparable (P=0.09). Conclusion: In patients undergoing lumbar instrumentation surgery, opioid consumption, VAS scores, PCA pump bad demands, inhalational agent consumption, hospital stay were comparable when either ketamine or dexmedetomidine was used as intraoperative anesthetic adjuvants.
INTRODUCTION
Spinal instrumentation and fusion surgery represent a broad continuum of anaesthetic possibilities and management not limited only to blood loss, haemodynamic changes but also to analgesic requirements and their associated short- and long-term outcome. The cause of such severe pain is due to tissue damage that occurs during retraction of soft tissue and muscles for exposure.[1] [2] Pain can lead to delayed ambulation with its associated complications such as deep vein thrombosis,[3] respiratory problems such as atelectasis, pneumonia and muscle atrophy.[4]
There are studies which have shown that with the use of increased dose of opioids in the intraoperative period there is central sensitisation[5] and allodynia.[6] There have been number of studies on this aspect using ketamine[7] [8] [9] [10] and dexmedetomidine[11] [12] as anaesthetic adjuvant intraoperatively as well as in the post-operative period causing a decrease in intraoperative anaesthetic and post-operative analgesic requirements.
On the above premise, multiple studies were carried out using a subanaesthetic dose or low-dose ketamine as an anaesthetic adjuvant in the intraoperative period which yielded a decrease in opioid use[7] and post-operative nausea and vomiting.[8] There are few studies evaluating the post-operative analgesic effect of dexmedetomidine in spine surgery[9] although it has been used as hypotensive agent[10] and as an add-on with morphine in the patient-controlled analgesia (PCA) pump in post-operative period.[13] The latter study did show a morphine-sparing effect. With the use of α2 agonists, the animal studies did not show a decrease in opioid consumption[11] while human studies showed a more favourable result.[12]
To the best of our knowledge, there are no studies comparing the analgesic property of ketamine and dexmedetomidine when used as an intraoperative anaesthetic adjuvant in terms of post-operative pain relief or analgesic consumption.
The primary aim of our study was to compare the post-operative analgesic requirements for first 24 h after surgery. The secondary aim was to compare the intraoperative anaesthetic requirements, haemodynamic parameters such as heart rate (HR) and mean arterial pressure (MAP), any side effects of study drugs in first 24 h after surgery and the duration of Intensive Care Unit (ICU) and hospital stay.
MATERIALS AND METHODS
Approval from the Institutional Ethics Committee for conducting this study and the informed consent from the patient was taken (IESC/T-436/01.11.2013).
Adult patients aged 18–60 years belonging to either sex of the American Society of Anesthesiologists (ASA) Status I or II scheduled for elective lumbar spine instrumentation (2 or more spinal levels) surgery were enrolled for the study. Patients were explained about visual analogue scale (VAS) and the use of PCA pump.
Exclusion criteria
Patients were excluded from the study if there was known allergy to ketamine or dexmedetomidine, history of liver or renal disease, patients on chronic β-blocker treatments with low baseline HR (<60/min), pregnancy, increased intraocular pressure, uncontrolled hypertension, increased intracranial pressure, history of psychosis, seizure disorder and ASA Status III or IV.
Routine pre-operative check-up was performed and investigations were reviewed in the evening before surgery. All patients received intramuscular glycopyrrolate 0.2 mg 30 min before transfer to operation theatre (OT).
Study protocol
A computer generated randomisation scheme was used to randomise patients into one of the three treatment regimens. An opaque sealed envelope method was used for allocation of the patients to three groups: Racemic ketamine/Group K (0.5 mg/kg bolus followed by 250 mcg/kg/h infusion), dexmedetomidine/Group D (0.5 mcg/kg bolus followed by 0.5 mcg/kg/h infusion) or the placebo (saline)/Group S. Principal investigator/anaesthesia provider, patient and nursing staff were blinded to the treatment assignment during the entire hospital stay.
A standard anaesthesia induction and maintenance protocol was followed. After shifting the patient to operation theatre (OT) standard monitors such as an electrocardiograph, pulse oximeter and non-invasive blood pressure (NIBP) were connected, and the intravenous (IV) line was established.
After pre-oxygenation for 2 min, general anaesthesia was induced with fentanyl 2 mcg/kg and propofol 2–3 mg/kg. Tracheal intubation was facilitated with rocuronium 1 mg/kg. Anaesthesia was maintained using sevoflurane in oxygen-air mixture in 40:60 ratios with a fresh gas flow rate of 1.5 L/min. Muscle relaxation was achieved with rocuronium 0.25 mg/kg bolus every 40 min and analgesia with fentanyl 1 mcg/kg as and when required. A bispectral index was used with target BIS between 40 and 50. Additional monitors after intubation consisted of end-tidal carbon dioxide (EtCO2), IBP, gases, airway pressure and nasopharyngeal temperature.
Once the patient was turned prone the study drug (bolus) was administered over 10 min using the syringe pump with 10 ml syringe (i.e., 60 ml/h for 10 min). Patients in Group K received 0.5 mg/kg bolus while those Group D received 0.5 mcg/kg. For Group S, 0.9% normal saline was used. HR, blood pressure (BP) and oxygen saturation (SpO2) were noted during the start and end of bolus infusion. A constant infusion rate of ‘(weight of patient in kg/8) ml/h’ was started prior to skin incision which delivered at the rate of 0.5 mcg/kg/h for dexmedetomidine and 250 mcg/kg/h or 4.166 mcg/kg/min for ketamine (by varying the drug concentration in a 50 ml syringe). The study drug infusions were prepared by an anaesthesiologist based on the weight of the patient pre-operatively with random drug selection who was not involved in the management of the patient. Two syringes one labelled as ‘Loading-drug-X’ with a 10 ml syringe (containing net 0.5 mg/kg of ketamine or 0.5 mcg/kg of dexmedetomidine) and another as ‘Infusion-drug-X’ with 50 ml syringes (having a concentration of 2 mg/ml for ketamine and 4 mcg/ml of dexmedetomidine) were prepared for each patient. Systolic BP was maintained within 20% of baseline values. Hypotension was defined as 20% drop from baseline value and hypertension defined as 20% rise from baseline value for >1 min.
Any event of hypotension was treated with:
-
Increase of IV fluid, and/or
-
Bolus doses of phenylephrine 0.5 mcg/kg IV
-
For non-responsive cases, IV infusion of phenylephrine was used.
Hypertension was treated with:
-
Increasing the depth of anaesthesia with sevoflurane if BIS was >50
-
If BIS was between 40 and 50, then fentanyl bolus of 1 mcg/kg was given. Intraoperatively, bradycardia was defined as HR <60 beats/min accompanied with haemodynamic instability or an HR <40 beats/min with or without haemodynamic instability while tachycardia as a 20% increase from baseline in HR.
Bradycardia was treated with:
-
0.6 mg IV atropine bolus and repeated as required
-
For non-responders, dopamine (2–10 mcg/kg/min infusion) or adrenaline (2–10 mcg/min infusion) had been planned.
The number of episodes of bradycardia, hypotension and hypertension were noted. End-tidal sevoflurane concentration was decreased by 50% at the start of skin closure and turned off after turning the patient supine. The study drug infusion was stopped at the closure of muscle layer.
After turning the patient, supine residual neuromuscular blockade was reversed with neostigmine (50 mcg/kg) and glycopyrrolate (8–10 mcg/kg). The trachea was extubated according to the standard extubation criteria and time noted. Emergence agitation if any and scored based on Riker et al. sedation-agitation scale were noted.[13]
HR, BP, EtCO2 and SpO2 were recorded at 0, 5, 15 min and then at every 15 min interval starting from prone positioning till the end of skin closure. Total dose of fentanyl, duration of surgery (from skin incision to skin closure) and anaesthesia, blood loss, sevoflurane consumption and recovery time (time interval between stopping of sevoflurane and ability to follow verbal commands) were noted.
The patients were shifted to ICU where IV PCA was started (bolus dose of 30 μg of fentanyl, lockout interval of 10 min with no basal infusion). Fentanyl consumption via IV-PCA was evaluated for 24 h after surgery. The percentage of bad demands (PCA pump press made within the lockout period leading to non-delivery of fentanyl) and good demands (PCA pump press made beyond the lockout period leading to successful fentanyl delivery) were also noted. Pain was quantified with a 10 cm VAS from 0 to 10 with 0 being pain-free and 10 being worst pain. This score was explained to the patient before surgery during pre-operative assessment. Pain scores in ICU were recorded at rest and during movement at baseline (just before starting PCA pump), 6, 12 and 24 h after surgery. For VAS scores >4 or pain not relieved with PCA bolus (breakthrough pain), the nursing staff were instructed to give 30 mcg of fentanyl as top-up boluses (rescue analgesic). Adverse events such as sedation, headache, nausea/vomiting and hallucination/dreams were recorded. For nausea or vomiting, 4 mg ondansetron was administered. The total days of stay in ICU and hospital were also noted.
Statistical analysis
On literature review[7] and assuming that baseline parameters were same in all the three groups after 24 h, then with α of 5% and power of 80%, 42 cases were required in 3 groups of 14 patients each. Data were analysed by Stata 11.1. Quantitative variables were expressed as mean ± standard deviation or median (range) for normal and skewed data, respectively. Qualitative variables were expressed as frequency and percentage. One-way ANOVA followed by Bonferroni test (for normal data) and Kruskal–Wallis followed by multiple comparisons using Wilcoxon-rank sum with Bonferroni correction (for skewed data) were used to compare mean/median values among the groups. P <0.05 was considered statistically significant.
RESULTS
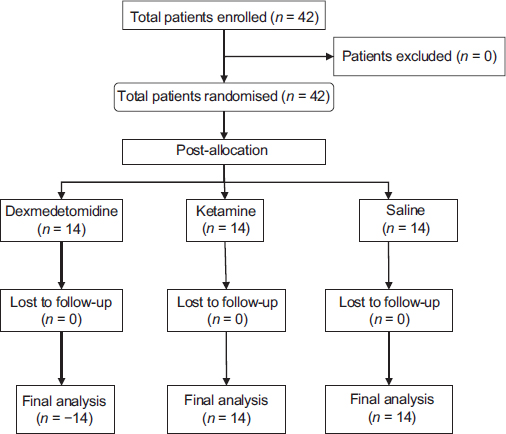
A total of 42 patients with 14 in each were enrolled [Figure 1]. There was no loss of any patient enrolled during the study. The baseline demographics of the patients were similar [Table 1]. The groups were also similar with respect to the duration of surgery and anaesthesia, intraoperative blood loss, fluids/blood used during surgery.
When the average HR and MAP were analysed over time a significant increase of the latter was seen during the initial 30 to 45 min of surgery in the ketamine group just after giving bolus of the drug and starting of infusion [Figures 2] and [3].


The episodes of haemodynamic alterations were seen in all the three groups. Hypotension was observed in all three groups but more in Group D (1 ± 0.9) and Group K (0.6 ± 0.9) (P = 0.33). Similarly, there was no significant difference in the incidence of hypertension among the groups.
Total sevoflurane and fentanyl consumption [Table 1] showed no significant difference (P = 0.19 and P = 0.28) among the groups even though sevoflurane use was higher in Group K. The post-extubation Riker sedation Agitation Scale (RAS) score was significantly lower (P = 0.009) in Group K (3.7 ± 0.6) when compared to Group D (4 ± 0.4) and Group S (4.5 ± 0.9). The recovery time was highest with Group K (13.3 ± 5.7 min) but was not significant (P = 0.37) [Figure 4].

All the patients were extubated uneventfully at the end of surgery and shifted to ICU. The total PCA fentanyl consumed in first 24 h of surgery [Figure 5] was maximum with the Group S (1366.6 ± 382.6 mcg) as compared to Group D (1035.4 ± 391.8 mcg) and Group K (1164.9 ± 503.6 mcg), but this did not reach statistical significance (P = 0.13). The percentage of bad demands (PCA press that did not deliver the analgesic) was more with Group S but was again not significant [Figure 6].


The rescue analgesic in the form of fentanyl within the first 24 h of surgery when compared between the three groups showed higher amount in Group S (117.9 ± 44.8 mcg) and was significant (P = 0.0001) when compared with the other two groups but not between Group D and Group K (P = 0.02) when compared by Mann–Whitney U-test [Figure 7] where between the groups the P is statistically significant when it is <0.017.

The VAS-r (at rest) score [Table 2] showed a significant rise in the Group S at baseline (i.e., at the time of starting PCA pump) (P = 0.009). The VAS-m (with movement) was higher in Group S when compared to the other two groups and was significantly higher at baseline, 12 and 24 h post-surgery. VAS scores were higher in Group K in compared to Group D but were not significant [Table 2].
The most common complication in the post-operative period was constipation affecting three patients in Group S, two in Group K and none in Group D. Nausea and vomiting occurred in one patient in each group which was relieved with ondansetron.
The ICU stay was similar (Group D: 1.4 ± 0.5, Group K: 1.5 ± 0.5, Group S: 1.9 ± 0.5) among the groups. Hospital stay [Figure 8] was least with Group K (Group D: 12.9 ± 6, Group K: 10.3 ± 6.5, Group S: 13.2 ± 6.4) but was not significant (P = 0.09).

DISCUSSION
In this study, the analgesic requirement within the first 24 h of surgery was comparable when either dexmedetomidine or ketamine was used intraoperatively as an anaesthetic adjuvant in lumbar spine instrumentation surgery. The VAS scores at rest and with the movement were significantly higher at baseline in Group S in comparison to other two groups and remained so with movement at 12 and 24 h after surgery. This was reflected in the significantly higher rescue analgesics administered to patients in Group S. The total fentanyl consumed through PCA pump, VAS scores and rescue analgesics were not significant when dexmedetomidine was compared to ketamine.
In case of lumbar instrumentation, it is a routine practice to administer opioid like fentanyl or morphine in the intraoperative period and IV morphine, fentanyl, paracetamol, tramadol or ketorolac in the post-operative period.
Intraoperative use of adjuvants has led to decreased use of opioids during surgery and prevents post-operative opioid tolerance and hyperalgesia. Among these adjuvants ketamine which have a proven efficacy to prevent wind-up phenomena[14] has been used in lumbar instrumentation surgery. Dexmedetomidine has also been used for similar situations, but studies are fewer in comparison to ketamine.
The results of our study were contrary to the study by Kim et al.[7] Sixty patients were assigned randomly to receive one of the three study medications – Group K1: Ketamine infusion of 1 mcg/kg/min following a bolus of 0.5 mcg/kg; Group K2: Ketamine infusion of 2 mg/kg/min following a bolus of 0.5 mg/kg, control group: Saline infusion following a bolus of saline] where they found significant decrease in post-operative fentanyl consumption. Presumably, this was because of continuing the ketamine infusion till 48 h after surgery along with PCA fentanyl unlike in our study where PCA pump was stopped at 24 h and patient started on oral analgesics.
Garg et al.[15] found significant decrease of post-operative opioid consumption when either ketamine (bolus: 0.25 mg/kg, infusion: 0.25 mg/kg/h) or dexmedetomidine (bolus: 0.5 mcg/kg, infusion: 0.3 mcg/kg/h) was used along with PCA morphine in the post-operative period (in patients operated with lumbar instrumentation surgery) when compared to saline. They did not find a significant difference among the study drugs. This study compared ketamine and dexmedetomidine, but unlike our study here the drugs were infused in the post-operative period and not as anaesthetic adjuvant.
Loftus et al.[16] in 2010 evaluated ketamine as an anaesthetic adjuvant to decrease the perioperative opioid use in opioid-dependent patients undergoing back surgery. They found a reduction in opioid consumption and pain intensity without any increase in side effects. In this study, 52 patients in the treatment group were given 0.5 mg/kg IV ketamine at induction followed by continuous infusion at 10 mcg/kg/min which was stopped at wound closure. While in the placebo group saline was used in equivalent volume. Patients were observed for 48 h postoperatively and followed up to 6 weeks. The primary objective as mentioned was 48-h morphine consumption. They found a 37% reduction in opioid consumption unlike in our study where we found about 14.75% mean reduction which was probably due to the lower infusion dosage (4.16 mcg/kg/min vs. 10 mcg/kg/min) and the population of our study were opioid naive.
Yamauchi et al.[17] in 2008, carried out a prospective randomised trial in 202 patients of ASA Status I or II age between 20 and 70 years undergoing cervical or lumbar spinal surgery. Here, they compared the adjuvant effects of ketamine on post-operative fentanyl PCA by co-administration in two different doses as IV infusion i.e.,, ket-1 group with 1 mg/kg bolus followed by 42 mcg/kg/h infusion and ket-2 group with 2 mg/kg bolus followed by 83 mcg/kg/h infusion for 24 h. They found out a significant lowering of pain score and analgesia in ket-2 group than those in control group after cervical surgery while it was only partially improved in lumbar surgery. This again emphasises on the varying degree of pain perception with different spinal levels of surgery.
In our study, the total sevoflurane consumption was comparable within the three groups. However, the consumption of sevoflurane was higher in ketamine which could be attributed to rise in BIS values with ketamine and the constant effort to maintain BIS between the targets of 40–50. This in turn led to patients to emerge more sedated with significantly lower RAS scores. The post-operative complications were similar with constipation being most frequently encountered. There was no incidence of hallucination either following extubation or in post-operative period. We did not use midazolam along with ketamine as previously stated by Elia and Tramèr[18] that in anaesthetised patients, the risk of ketamine-induced hallucinations is minimal and that benzodiazepines are not universally protective. The duration of hospital stay was also comparable between the groups.
The limitation of our study is that we did not use an equivalent dose of ketamine and dexmedetomidine and the dosage used in this study reflect that used in existing literature. BIS was used to assess the anaesthetic depth where ketamine may have caused a paradoxical increase leading to study protocol driven efforts to control it. This could have increased sevoflurane consumption.
CONCLUSION
In this study on 42 patients, it was found both ketamine and dexmedetomidine can be used as an anaesthetic adjuvant to improve the post-operative analgesia in patients undergoing lumbar instrumentation surgery. Larger sample size is needed to prove the superiority of one drug, over the other.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
No conflict of interest has been declared by the author(s).
-
REFERENCES
- 1 Hoh DJ, Wang MY, Ritland SL. Anatomic features of the paramedian muscle-splitting approaches to the lumbar spine. Neurosurgery 2010; 66: 13-24
- 2 Arts M, Brand R, van der Kallen B, Lycklama à Nijeholt G, Peul W. Does minimally invasive lumbar disc surgery result in less muscle injury than conventional surgery? A randomized controlled trial. Eur Spine J 2011; 20: 51-7
- 3 Schulte LM, O'Brien JR, Bean MC, Pierce TP, Yu WD, Meals C. Deep vein thrombosis and pulmonary embolism after spine surgery: Incidence and patient risk factors. Am J Orthop (Belle Mead NJ) 2013; 42: 267-70
- 4 Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth 1997; 78: 606-17
- 5 Chia YY, Liu K, Wang JJ, Kuo MC, Ho ST. Intraoperative high dose fentanyl induces postoperative fentanyl tolerance. Can J Anaesth 1999; 46: 872-7
- 6 Chang G, Chen L, Mao J. Opioid tolerance and hyperalgesia. Med Clin North Am 2007; 91: 199-211
- 7 Kim SH, Kim SI, Ok SY, Park SY, Kim MG, Lee SJ. et al. Opioid sparing effect of low dose ketamine in patients with intravenous patient-controlled analgesia using fentanyl after lumbar spinal fusion surgery. Korean J Anesthesiol 2013; 64: 524-8
- 8 Bell RF, Dahl JB, Moore RA, Kalso E. Peri-operative ketamine for acute post-operative pain: A quantitative and qualitative systematic review (Cochrane review). Acta Anaesthesiol Scand 2005; 49: 1405-28
- 9 Gupta N, Rath GP, Prabhakar H, Dash HH. Effect of intraoperative dexmedetomidine on postoperative recovery profile of children undergoing surgery for spinal dysraphism. J Neurosurg Anesthesiol 2013; 25: 271-8
- 10 El-Gohary MM, Arafa AS. Dexmedetomidine as a hypotensive agent: Efficacy and hemodynamic response during spinal surgery for idiopathic scoliosis in adolescents. Egypt J Anaesth 2010; 26: 305-11
- 11 Kontinen VK, Paananen S, Kalso E. The effects of the alpha2-adrenergic agonist, dexmedetomidine, in the spinal nerve ligation model of neuropathic pain in rats. Anesth Analg 1998; 86: 355-60
- 12 Gurbet A, Basagan-Mogol E, Turker G, Ugun F, Kaya FN, Ozcan B. Intraoperative infusion of dexmedetomidine reduces perioperative analgesic requirements. Can J Anaesth 2006; 53: 646-52
- 13 Riker RR, Fraser GL, Simmons LE, Wilkins ML. Validating the Sedation-Agitation Scale with the Bispectral Index and Visual Analog Scale in adult ICU patients after cardiac surgery. Intensive Care Med 2001; 27: 853-8
- 14 Guirimand F, Dupont X, Brasseur L, Chauvin M, Bouhassira D. The effects of ketamine on the temporal summation (wind-up) of the R(III) nociceptive flexion reflex and pain in humans. Anesth Analg 2000; 90: 408-14
- 15 Garg N, Panda NB, Gandhi KA, Bhagat H, Batra YK, Grover VK. et al. Comparison of small dose ketamine and dexmedetomidine infusion for postoperative analgesia in spine surgery – A prospective randomized double-blind placebo controlled study. J Neurosurg Anesthesiol 2016; 28: 27-31
- 16 Loftus RW, Yeager MP, Clark JA, Brown JR, Abdu WA, Sengupta DK. et al. Intraoperative ketamine reduces perioperative opiate consumption in opiate-dependent patients with chronic back pain undergoing back surgery. Anesthesiology 2010; 113: 639-46
- 17 Yamauchi M, Asano M, Watanabe M, Iwasaki S, Furuse S, Namiki A. Continuous low-dose ketamine improves the analgesic effects of fentanyl patient-controlled analgesia after cervical spine surgery. Anesth Analg 2008; 107: 1041-4
- 18 Elia N, Tramèr MR. Ketamine and postoperative pain – A quantitative systematic review of randomised trials. Pain 2005; 113: 61-70
Address for correspondence:
-
REFERENCES
- 1 Hoh DJ, Wang MY, Ritland SL. Anatomic features of the paramedian muscle-splitting approaches to the lumbar spine. Neurosurgery 2010; 66: 13-24
- 2 Arts M, Brand R, van der Kallen B, Lycklama à Nijeholt G, Peul W. Does minimally invasive lumbar disc surgery result in less muscle injury than conventional surgery? A randomized controlled trial. Eur Spine J 2011; 20: 51-7
- 3 Schulte LM, O'Brien JR, Bean MC, Pierce TP, Yu WD, Meals C. Deep vein thrombosis and pulmonary embolism after spine surgery: Incidence and patient risk factors. Am J Orthop (Belle Mead NJ) 2013; 42: 267-70
- 4 Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth 1997; 78: 606-17
- 5 Chia YY, Liu K, Wang JJ, Kuo MC, Ho ST. Intraoperative high dose fentanyl induces postoperative fentanyl tolerance. Can J Anaesth 1999; 46: 872-7
- 6 Chang G, Chen L, Mao J. Opioid tolerance and hyperalgesia. Med Clin North Am 2007; 91: 199-211
- 7 Kim SH, Kim SI, Ok SY, Park SY, Kim MG, Lee SJ. et al. Opioid sparing effect of low dose ketamine in patients with intravenous patient-controlled analgesia using fentanyl after lumbar spinal fusion surgery. Korean J Anesthesiol 2013; 64: 524-8
- 8 Bell RF, Dahl JB, Moore RA, Kalso E. Peri-operative ketamine for acute post-operative pain: A quantitative and qualitative systematic review (Cochrane review). Acta Anaesthesiol Scand 2005; 49: 1405-28
- 9 Gupta N, Rath GP, Prabhakar H, Dash HH. Effect of intraoperative dexmedetomidine on postoperative recovery profile of children undergoing surgery for spinal dysraphism. J Neurosurg Anesthesiol 2013; 25: 271-8
- 10 El-Gohary MM, Arafa AS. Dexmedetomidine as a hypotensive agent: Efficacy and hemodynamic response during spinal surgery for idiopathic scoliosis in adolescents. Egypt J Anaesth 2010; 26: 305-11
- 11 Kontinen VK, Paananen S, Kalso E. The effects of the alpha2-adrenergic agonist, dexmedetomidine, in the spinal nerve ligation model of neuropathic pain in rats. Anesth Analg 1998; 86: 355-60
- 12 Gurbet A, Basagan-Mogol E, Turker G, Ugun F, Kaya FN, Ozcan B. Intraoperative infusion of dexmedetomidine reduces perioperative analgesic requirements. Can J Anaesth 2006; 53: 646-52
- 13 Riker RR, Fraser GL, Simmons LE, Wilkins ML. Validating the Sedation-Agitation Scale with the Bispectral Index and Visual Analog Scale in adult ICU patients after cardiac surgery. Intensive Care Med 2001; 27: 853-8
- 14 Guirimand F, Dupont X, Brasseur L, Chauvin M, Bouhassira D. The effects of ketamine on the temporal summation (wind-up) of the R(III) nociceptive flexion reflex and pain in humans. Anesth Analg 2000; 90: 408-14
- 15 Garg N, Panda NB, Gandhi KA, Bhagat H, Batra YK, Grover VK. et al. Comparison of small dose ketamine and dexmedetomidine infusion for postoperative analgesia in spine surgery – A prospective randomized double-blind placebo controlled study. J Neurosurg Anesthesiol 2016; 28: 27-31
- 16 Loftus RW, Yeager MP, Clark JA, Brown JR, Abdu WA, Sengupta DK. et al. Intraoperative ketamine reduces perioperative opiate consumption in opiate-dependent patients with chronic back pain undergoing back surgery. Anesthesiology 2010; 113: 639-46
- 17 Yamauchi M, Asano M, Watanabe M, Iwasaki S, Furuse S, Namiki A. Continuous low-dose ketamine improves the analgesic effects of fentanyl patient-controlled analgesia after cervical spine surgery. Anesth Analg 2008; 107: 1041-4
- 18 Elia N, Tramèr MR. Ketamine and postoperative pain – A quantitative systematic review of randomised trials. Pain 2005; 113: 61-70