

Subscribe to RSS
DOI: 10.4103/ijri.IJRI_77_16
Magnetic resonance imaging of ankle ligaments: A pictorial essay
Authors
Subject Editor:
Financial support and sponsorship Nil.


Abstract
Ankle trauma is commonly encountered and is most often a sprain injury affecting the ligaments. Accurate diagnosis and appropriate treatment rest on knowledge of complex ligamentous anatomy of ankle and the entire spectrum of pathologies. Magnetic resonance imaging (MRI) is the imaging modality of choice for diagnosing ligament pathologies because of its multiplanar capability and high soft tissue contrast. With MRI, it is possible to triage and attribute the cause of post traumatic ankle pain to bone, ligament, or tendon pathologies, which otherwise overlap clinically. In this pictorial essay, emphasis is given to the intricate and unique anatomy and orientation of ankle ligaments. Pathologies of ankle ligaments have been elaborated.
Introduction
Ankle is a complex mechanism consisting of two joints: the true ankle joint and the subtalar joint. The true ankle joint is composed of three bones, seen from the front: tibia medially; fibula laterally; and talus inferiorly. The true ankle joint is responsible for dorsiflexion and plantar flexion of the foot. Below the true ankle joint is the subtalar joint, composed of calcaneum inferiorly, and talus superiorly. The subtalar joint is responsible for inversion and eversion of the foot.
The two joints are supported and maintained by ligaments, each connecting two bones and the tendons. Injury to the ankle joint is a common emergency and usually a sprain related to sports, walking, fall, or road traffic accident. In ankle sprain, ligaments are frequently injured in association with bone fractures, avulsion, and contusions.
Imaging protocol
The sequences and parameters for optimal high resolution images are described in [Table 1].
|
Sequences and Parameters |
FOV (mm) |
TR (ms) |
TE (ms) |
Matrix |
Flip angle (°) |
Slice thickness (mm) |
Inversion (ms) |
|---|---|---|---|---|---|---|---|
|
FOV: Field of view, TR: Repetition time, TE: Echo time, PD: Proton Density, STIR: Short tau inversion recovery, DESS: Dual echo steady state |
|||||||
|
T1 axial/coronal |
120/100 |
600 |
15 |
320x448 |
140 |
3.0 |
|
|
PD axial/coronal |
120/100 |
3100 |
23 |
275x384 |
150 |
3.0 |
|
|
STIR sagittal |
250/70 |
4000 |
29 |
250x384 |
150 |
3.0 |
210 |
|
DESS |
120/100 |
13.01 |
4.79 |
210x256 |
25 |
0.7 |
|
Anatomy
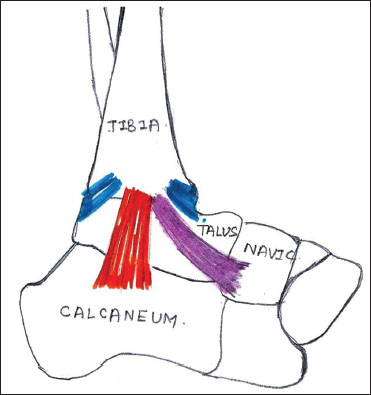
There are three major groups of ligaments supporting the ankle joint: lateral, medial or deltoid (superficial and deep component) and syndesmotic.
Sketch diagrams representing these groups are shown in [Figure 1] and [Figure 2].

Lateral ligaments
Anterior talofibular ligament (ATFL), Posterior talofibular ligament (PTFL), and Calcaneofibular ligament (CFL) [Figure 3]A and [Figure 3]B. Use of oblique coronal plane (CFL view) helps in better evaluation of anatomy and pathology (injury) of CFL as compared to orthogonal plane.[1]


Normal thickness of ATFL is 2 – 3 mm, and CFL is 2 mm.
Medial or deltoid ligaments
Superficial component of deltoid ligament
Tibiocalcaneal ligament (TCL), Tibionavicular ligament (TNL), and Tibiospring ligament (TSL) [Figure 4] and [Figure 5].


Deep component of deltoid ligament
Anterior tibiotalar ligament (ATTL) and Posterior tibiotalar ligament (PTTL) [Figure 6].

Normal thickness of TNL is 1–2 mm, and TSL is 2 mm (1–4mm). The PTTL is thickest ligament and normally measures 6–11 mm.
Syndesmotic ligaments
Anteroinferior tibiofibular ligament (AITFL), Posteroinferior tibiofibular ligament (PITFL), Interosseus membrane or ligament (IOL), and Inferior transverse (ITL). Of these AITFL and PITFL can be easily identified on routine MRI [Figure 7]. Anterior and posterior inferior tibiofibular ligaments are injured simultaneously.[2] A 45° oblique plane is superior in demonstrating their normal integrity/pathologies as compared to orthogonal imaging.[3] Fluid in Tibiofibular recess normally measures 5–7 mm.

In addition to these, the ankle is supported by the spring ligament. The spring ligament complex consists of superomedial (SM), medioplantar oblique (MPO), and inferoplantar longitudinal (IPL) components [Figure 8] and [Figure 9]. Normal thickness of SM component is 3 mm (2–5 mm), and IPL component is 4 mm (2–6 mm).


Pathology
Ligaments connect two bones; have higher proteoglycan and water content and less collagen. Normal ligaments are seen as uniform low-intensity band on T1 and T2 W images.[4] Notable exceptions include posterior talofibular, deep components of the deltoid ligament, and anterior inferior tibiofibular ligament that show heterogeneous signal and striations because of the interspersed fat between their fascicles.
Following acute injury the ligament undergoes repair in three stages. The first three days are characterized by inflammation, interstitial edema, and hemorrhage. The third to fifth days represent stage of repair with proliferation of fibroblasts. The second to fourth weeks are the stage of remodeling with formation of collagen. Periarticular edema is seen up to the seventh week.
Acute Injury
MRI shows blurred margins, irregular contours, discontinuous/wavy/lax fibers, inhomogeneous signal, or loss of normal hypointense signal within the ligament. Certain ligaments such as PTFL, deep components of the deltoid ligament, and AITFL show loss of normal striations due to presence of edema and hemorrhage. The ligament may be attenuated, thick, thin, or elongated.
Acute ligament injuries can be graded as interstitial, partial, or complete tear.
Interstitial tears
Hyperintense signal within the ligament on PD and T2W images due to presence of edema or hemorrhage [Figure 10].

Partial tears
Partial discontinuity of ligaments reaching up to the surface but not involving the entire thickness of ligament [Figure 11].

Complete tears
Discontinuity involving the entire thickness of ligament and is seen as fluid filled defect and retraction [Figure 12] and [Figure 13]. Joint effusion and obliteration of adjacent fat planes can be seen.


Ankle sprain contributes to 20–40% of sport injuries.[5] Depending on the mechanism of injuries, particular group of ligaments are injured.
Inversion injury accounts for 85% of ankle sprain and is commonly seen with high velocity sports such as basketball, soccer, and football.[5],[6] Inversion injury commonly affects the lateral ligament complex. Of these, ATFL being the weakest is more prone to injury[7],[8] [Figure 14]. Injury to ATFL is less common at the talar attachment because of the denser fibrocartilage and greater bone density than that of the fibular attachment.[9]

Eversion injuries commonly affect the medial deltoid ligament complex, accounting for approximately 5% of ankle sprains and are associated with sports such as gymnastic, rugby, and soccer.[10],[11]
High ankle/syndesmotic sprains account for 7% of routine ankle sprains and 40% of injuries in athletes. These are more often seen in association with sports such as football, ice hockey, soccer, skiing, running, and jumping.[12],[13] Fluid in the tibiofibular recess measuring >12 mm is definitely abnormal and suggestive of acute injury to syndesmotic ligaments or high ankle sprains[14],[15] [Figure 15].

Chronic Injury
MRI shows an attenuated, thin - hypoplastic, or alternately a thick - hyperplastic ligament with irregular contours and absence of edema or hemorrhage.
Impingement Syndrome
Anatomical variations of the ligaments alter joint mechanics, thus, making the individual prone to repeated injuries and chronic instability.[16] Anterolateral and medial impingement syndromes are the result of such chronic repetitive stress; these can be adequately diagnosed on MRI.
In chronic ATFL tear, granulation/scar tissue or fibrosis in the anterolateral gutter resembles a “meniscus” and can lead to clinical anterolateral impingement syndrome [Figure 16]. Similar findings can be seen in anteromedial and posteromedial impingement syndromes [Figure 17].


Post contrast fat-suppressed 3D-FSPGR (3D fast spoiled gradient echo recalled acquisition in the steady state) sequence of the ankle is superior and accurate in assessing anterolateral impingement syndrome by better delineation of synovial thickening/inflammation and granulation tissue.[8]
Important Associations
Ligaments and adjacent tendons have synergistic functions, and their injuries are most often simultaneous. Peroneal tendinosis is commonly seen with ATFL injury followed by CFL and PTFL injury[17] [Figure 12]. Partial longitudinal tear of peroneus brevis tendon is commonly associated with lateral ankle sprain.[18] Tibialis posterior tendon injuries are seen simultaneously with tibiospring and spring ligament complex injuries because of their synergistic action in maintaining the medial plantar arch[19],[20] [Figure 18] and [Figure 19]. Bone contusion, osteochondral lesion, and joint effusion are other common associations [Figure 19].


Conclusion
Knowledge of anatomy and imaging appearance of normal and abnormal ankle ligaments on MRI with an understanding of biomechanics of injury aids in achieving accurate diagnosis and appropriate treatment of ankle sprains. Depending on the MRI features and the clinical co-relates (Drawers test, inversion and eversion tests), it is possible for the clinicians to grade the ankle injury from mild to severe and also assess instability. Most of the ankle sprains are stable and are treated conservatively (rest, immobilization, ice compression, and elevation). Those associated with osteochondral lesions are treated with arthroscopic repair. Severe ankle sprain injuries with instability are treated with surgical reconstruction of ligaments.
Conflict of Interest
There are no conflicts of interest.
-
References
- 1 Park HJ, Lee SY, Park NH, Kim E, Chung EC, Kook SH. et al. Usefulness of the oblique coronal plane in ankle MRI of the calcaneofibular ligament. Clin Radiol 2015; 70: 416-23
- 2 Dattani R, Patnaik S, Kantak A, Srikanth B, Selvan TP. Injuries to the tibiofibular syndesmosis. J Bone Joint Surg Br 2008; 90: 405-10
- 3 Hermans JJ, Ginai AZ, Wentink N, Hop WC, Beumer A. The additional value of an oblique image plane for MRI of the anterior and posterior distal tibiofibular syndesmosis. Skeletal Radiol 2011; 40: 75-83
- 4 Hodgson RJ, O’Connor PJ, Grainger AJ. Tendon and ligament imaging. Br J Radiol 2012; 85: 1157-72
- 5 Dubin JC, Comeau D, McClelland RI, Dubin RA, Ferrel E. Lateral and syndesmotic ankle sprain injuries: A narrative literature review. J Chiropr Med 2011; 10: 204-19
- 6 Purcell SB, Schuckman BE, Docherty CL, Schrader J, Poppy W. Differences in ankle range of motion before and after exercise in 2 tape conditions. Am J Sports Med 2009; 37: 383-9
- 7 Boruta PM, Bishop JO, Braly WG, Tullos HS. Acute lateral ankle ligament injuries: A literature review. Foot Ankle 1990; 11: 107-13
- 8 Choo HJ, Suh JS, Kim SJ, Huh YM, Kim MI, Lee JW. et al. Ankle MRI for anterolateral soft tissue impingement: Increased accuracy with the use of contrast-enhanced fat-suppressed 3D-FSPGR MRI. Korean J Radiol 2008; 9: 409-15
- 9 Kumai T, Takakura Y, Rufai A, Milz S, Benjamin M. The functional anatomy of the human anterior talofibular ligament in relation to ankle sprains. J Anat 2002; 200: 457-65
- 10 Hintermann B, Knupp M, Pagenstert GI. Deltoid ligament injuries: Diagnosis and management. Foot Ankle Clin 2006; 11: 625-37
- 11 Waterman BR, Belmont Jr. PJ, Cameron KL, Svoboda SJ, Alitz CJ, Owens BD. et al. Risk factors for syndesmotic and medial ankle sprain: Role of sex, sport, and level of competition. Am J Sports Med 2011; 39: 992-8
- 12 Boytim MJ, Fischer DA, Neumann L. Syndesmotic ankle sprains. Am J Sports Med 1991; 19: 294-8
- 13 Norkus SA, Floyd RT. The anatomy and mechanisms of syndesmotic ankle sprains. J Athl Train 2001; 36: 68-73
- 14 Brown KW, Morrison WB, Schweitzer ME, Parellada JA, Nothnagel H. MRI findings associated with distal tibiofibular syndesmosis injury. AJR Am J Roentgenol 2004; 182: 131-6
- 15 Takao M, Ochi M, Naito K, Iwata A, Kawasaki K, Tobita M. et al. Arthroscopic diagnosis of tibiofibular syndesmosis disruption. Arthroscopy 2001; 17: 836-43
- 16 Imhauser CW, Siegler S, Udupa JK, Toy JR. Subject-specific models of the hindfoot reveal a relationship between morphology and passive mechanical properties. J Biomech 2008; 41: 1341-9
- 17 Ziai P, Benca E, Wenzel F, Schuh R, Krall C, Auffahrt A. et al. Peroneal tendinosis as a predisposing factor for the acute lateral ankle sprain in runners. Knee Surg Sports Traumatol Arthrosc 2016; 24: 1175-9
- 18 Karlsson J, Wiger P. Longitudinal split of the peroneus brevis tendon and lateral ankle instability: Treatment of concomitant lesions. J Athl Train 2002; 37: 463-6
- 19 Hintermann B. Biomechanics of the unstable ankle joint and clinical implications. Med Sci Sports Exerc 1999; 31: S459-69
- 20 Deland JT, de Asla RJ, Sung IH, Ernberg LA, Potter HG. Posterior tibial tendon insufficiency: Which ligaments are involved?. Foot Ankle Int 2005; 26: 427-35
Publication History
Article published online:
26 July 2021
© 2018. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Private Ltd.
A-12, Second Floor, Sector -2, NOIDA -201301, India
-
References
- 1 Park HJ, Lee SY, Park NH, Kim E, Chung EC, Kook SH. et al. Usefulness of the oblique coronal plane in ankle MRI of the calcaneofibular ligament. Clin Radiol 2015; 70: 416-23
- 2 Dattani R, Patnaik S, Kantak A, Srikanth B, Selvan TP. Injuries to the tibiofibular syndesmosis. J Bone Joint Surg Br 2008; 90: 405-10
- 3 Hermans JJ, Ginai AZ, Wentink N, Hop WC, Beumer A. The additional value of an oblique image plane for MRI of the anterior and posterior distal tibiofibular syndesmosis. Skeletal Radiol 2011; 40: 75-83
- 4 Hodgson RJ, O’Connor PJ, Grainger AJ. Tendon and ligament imaging. Br J Radiol 2012; 85: 1157-72
- 5 Dubin JC, Comeau D, McClelland RI, Dubin RA, Ferrel E. Lateral and syndesmotic ankle sprain injuries: A narrative literature review. J Chiropr Med 2011; 10: 204-19
- 6 Purcell SB, Schuckman BE, Docherty CL, Schrader J, Poppy W. Differences in ankle range of motion before and after exercise in 2 tape conditions. Am J Sports Med 2009; 37: 383-9
- 7 Boruta PM, Bishop JO, Braly WG, Tullos HS. Acute lateral ankle ligament injuries: A literature review. Foot Ankle 1990; 11: 107-13
- 8 Choo HJ, Suh JS, Kim SJ, Huh YM, Kim MI, Lee JW. et al. Ankle MRI for anterolateral soft tissue impingement: Increased accuracy with the use of contrast-enhanced fat-suppressed 3D-FSPGR MRI. Korean J Radiol 2008; 9: 409-15
- 9 Kumai T, Takakura Y, Rufai A, Milz S, Benjamin M. The functional anatomy of the human anterior talofibular ligament in relation to ankle sprains. J Anat 2002; 200: 457-65
- 10 Hintermann B, Knupp M, Pagenstert GI. Deltoid ligament injuries: Diagnosis and management. Foot Ankle Clin 2006; 11: 625-37
- 11 Waterman BR, Belmont Jr. PJ, Cameron KL, Svoboda SJ, Alitz CJ, Owens BD. et al. Risk factors for syndesmotic and medial ankle sprain: Role of sex, sport, and level of competition. Am J Sports Med 2011; 39: 992-8
- 12 Boytim MJ, Fischer DA, Neumann L. Syndesmotic ankle sprains. Am J Sports Med 1991; 19: 294-8
- 13 Norkus SA, Floyd RT. The anatomy and mechanisms of syndesmotic ankle sprains. J Athl Train 2001; 36: 68-73
- 14 Brown KW, Morrison WB, Schweitzer ME, Parellada JA, Nothnagel H. MRI findings associated with distal tibiofibular syndesmosis injury. AJR Am J Roentgenol 2004; 182: 131-6
- 15 Takao M, Ochi M, Naito K, Iwata A, Kawasaki K, Tobita M. et al. Arthroscopic diagnosis of tibiofibular syndesmosis disruption. Arthroscopy 2001; 17: 836-43
- 16 Imhauser CW, Siegler S, Udupa JK, Toy JR. Subject-specific models of the hindfoot reveal a relationship between morphology and passive mechanical properties. J Biomech 2008; 41: 1341-9
- 17 Ziai P, Benca E, Wenzel F, Schuh R, Krall C, Auffahrt A. et al. Peroneal tendinosis as a predisposing factor for the acute lateral ankle sprain in runners. Knee Surg Sports Traumatol Arthrosc 2016; 24: 1175-9
- 18 Karlsson J, Wiger P. Longitudinal split of the peroneus brevis tendon and lateral ankle instability: Treatment of concomitant lesions. J Athl Train 2002; 37: 463-6
- 19 Hintermann B. Biomechanics of the unstable ankle joint and clinical implications. Med Sci Sports Exerc 1999; 31: S459-69
- 20 Deland JT, de Asla RJ, Sung IH, Ernberg LA, Potter HG. Posterior tibial tendon insufficiency: Which ligaments are involved?. Foot Ankle Int 2005; 26: 427-35