
Subscribe to RSS
DOI: 10.4103/ijri.IJRI_364_20
Exploring the correlation between increased femoral anteversion and pars interarticularis defects in the lumbar spine: A single center experience
Financial support and sponsorship Nil.


Abstract
Introduction: Altered femoral version can result in lumbar hyperlordosis and hip spine syndrome. We conducted a retrosepctive study to evalute if there is correlation between altered femoral version and pars defect. Materal and Methods: A cohort of pateints with CT rotational profile and MR of lumbar spine over a 12 year period were included in the sutdy. The femoral version was calculated and the MR was evaluated for pars defect. Results: 130 patients had CT rotational profile and MR of lumbar spine with a female predomiannce ( 94 female and 36 males) and average age of 24.3 years. There were 6 patients with bilateral pars defects involving L5 ( 3 with increased femoral version, 2 with decreased version and one had normal version). Conclusion: Increased femoral anterversion is not associated with increased prevalence of pars defects.
Introduction
Increased femoral anteversion (IFA) is an axial plane rotational deformity which may contribute to developmental anterior pelvic tilt and lumbar hyperlordosis resulting in hip-spine syndrome, early hip osteoarthrosis, and knee pain owing to altered biomechanics.[1], [2] In addition, patients with IFA, particularly children, demonstrate reduced lower extremity function and higher falling frequencies.[3] IFA is associated with lumbar hyperlordosis, which potentially produces increased pressure on the posterior arch structures including pars interarticularis.[2] It has been proposed that lumbar hyperlordosis may contribute to the development of pars interarticularis defects.[4], [5] We had a few young patients with low back pain (pars defect on MRI) who have altered femoral version. We have, thus, conducted a retrospective study to evaluate whether IFA is associated with an increased incidence of pars interarticularis defects in the lumbar spine.
Methods
Following institutional review board approval (Ref 20-010 on 24/02/2020), a retrospective search for femoral anteversion studies at our tertiary orthopedic institute database over the last 12 years (2007-2019) was performed. Standardized methods for femoral anteversion calculation were utilized.[6]
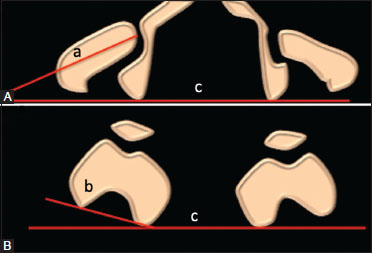
The computed tomography (CT) examination was performed with the patient positioned in the supine and feet first position on the CT table without extra leg support. Keeping legs as close as possible (utilizing tapeing? of feet/knees when needed), a single anteroposterior CT scout from just above femoral heads to the tibial midshafts was obtained. Two ranges of helical CT axial images of 5 mm thickness were acquired at 5 mm interval using a bony algorithm. The first range was taken through the hip from just above the femoral heads through to the lesser trochanters, whereas the second range was acquired from just above the femoral condyles through to the tibial plateaux. Femoral neck anteversion was measured in the axial plane as the angle between a line drawn through the neck of the femur long axis and a line joining the posterior surfaces of the medial and lateral femoral condyles. The exact angle was calculated using the horizontal line as a standard and by adding or subtracting neck-horizontal angle and condyle-horizontal angle depending upon the internal or external rotation of distal femoral condyles, respectively [Figure 1]. Normal femoral version was taken to be 15–20 degrees.[6] Patients with increased femoral version (>20 degrees) in one or both hips were categorized as having increased anteversion, and patients with decreased femoral version in one or both hips (<15 degrees) were categorized as having decreased femoral version. Patients who had increased femoral version in one hip but decreased femoral version in the other were excluded.
Among the above patients with rotational profile CT studies, a search of the radiology information system (RIS) was performed to identify the subset of patients who had a magnetic resonance imaging (MRI) of the lumbar spine. These patients form the study cohort. The MRI images were evaluated for the presence of lumbar spine pars interarticularis defects, and the level of these defects, by the senior author, I reviewed them too!!.
Results
Overall, 1916 patients were identified as having had a CT rotation profile with a female predominance (1282 females, 634 males, with mean age of 24.7 years). Of these 1916 patients, 130 patients had an MR lumbar spine, comprising 94 females and 36 males, with a mean age of 24.3 years (range: 10–40 years). There were 53 patients with increased version, 52 with decreased femoral version, and 5 patients with normal version. A further 20 patients were excluded as there was increased femoral version in one hip and decreased version in the contralateral hip.
Out of 53 patients with increased femoral version, there were three patients with pars defects (prevalence of 5.6%). Out of 52 patients with decreased femoral version, there were two patients with pars defects (prevalence of 3.8%). There was no significant difference in the prevalence of pars defects in patients with IFA and low version (P = 0.68, Fisher’s exact test). All pars defect involved L5 and were bilateral [Figure 2]. There was also 1 pars defect in a patient with normal version [Table 1].

|
Age |
Sex |
Type of pars |
Side of pars defect |
Level of defect |
Femoral anteversion |
|
|---|---|---|---|---|---|---|
|
Right hip |
Left hip |
|||||
|
32 |
F |
Complete |
bilateral |
L5 |
18 |
20 |
|
20 |
F |
Complete |
bilateral |
L5 |
17 |
35 |
|
IS |
F |
Complete |
bilateral |
L5 |
6 |
15 |
|
22 |
F |
Complete |
bilateral |
L5 |
6 |
10 |
|
18 |
F |
Complete |
bilateral |
L5 |
30 |
23 |
|
16 |
F |
Complete |
bilateral |
L5 |
29 |
15 |
Discussion
IFA produces compensatory biomechanical changes in the pelvis and spine. Increased anterior acetabular coverage, anterior pelvic tilt, and hyperlordosis are some of the biomechanical changes typically associated with IFA leading to hip-spine syndrome and early hip osteoarthritis.[2] Hyperlordosis of the lumbar spine—resulting in increased stress over posterior arch structures, ligaments, and facet joints—is considered an important causative factor for low back pain.[7], [8] Hyperlordosis of the lumbar spine is also associated with facet joint arthrosis in the lumbar spine.[9] It has previously been proposed that lumbar hyperlordosis may contribute to the development of pars interarticularis defects.[4], [5]
Our results demonstrate that there is no clinically significant correlation between increased femoral version and the prevalence of pars defects. The prevalence of pars defect in patients with increased or decreased femoral version in our study (4%–8%) is similar to the 5%–9% reported in general population,[10] confirming that the contribution of femoral version to the development of pars defects is either nonexistent or very small. This is in contrast to known factors such as certain athletic activities that have a marked impact on the prevalence of par defects. For example, the prevalence of pars defects is significantly increased in some athletes, such as in divers (35%), cricketers (31%), and rugby athletes (22%).[4]
Our findings add onto the current understanding of the factors that may contribute to the pathogenesis of pars defects, which remains unclear. There are two possible reasons for the lack of positive findings. One interpretation of our findings is that impact of femoral version on lumbar hyperlordosis is small and insufficient to result in the development of pars defects. The impact of changes in femoral version on hyperlordosis has only been investigated indirectly through the impact of the former on anterior pelvic tilt. Okuzu et al. found a correlation between increased femoral version and anterior pelvic tilt (and by implication lumbar hyperlordosis), though this was not statistically significant in their cohort of 66 patiets.[2] Another possible explanation is the association between lumbar hyperlordosis and pars defects[5] is not a causal relationship. For example, it has not been shown that lumbar hyperlordosis precedes the subsequent development of pars defects.
Limitations of our study include single center study and relatively low number of cases. Another possible limitation is the use of MRI instead of CT, the latter which is often considered to be the gold standard for the detection of pars defects. However, the sensitivity (81%) and specificity (99%) of MRI for pars defect is sufficiently high, such that the use of MRI instead of CT is unlikely to result in a significant change in the prevalence of pars defects in our cohort.[11]
Conclusion
A relationship between spinal and hip pathology is recognized, but is not fully understood. This study demonstrates that IFA is not associated with an increased prevalence of pars defects in the lower lumbar spine.
Conflict of Interest
There are no conflicts of interest.
-
References
- 1 Tansey P. Hip and low back pain in the presence of femoral anteversion. A case report. Man Ther 2015; 20: 206-11
- 2 Okuzu Y, Goto K, Okutani Y, Kuroda Y, Kawai T, Matsuda S. Hip-spine syndrome: Acetabular anteversion angle is associated with anterior pelvic tilt and lumbar hyperlordosis in patients with acetabular dysplasia: A retrospective study. JBJS Open Access 2019; 4: e0025
- 3 Leblebici G, Akalan E, Apti A, Kuchimov S, Kurt A, Onerge K. et al. Increased femoral anteversion-related biomechanical abnormalities: Lower extremity function, falling frequencies, and fatigue. Gait Posture 2019; 70: 336-40
- 4 Tawfik S, Phan K, Mobbs RJ, Rao PJ. The incidence of pars interarticularis defects in athletes. Glob Spine J 2020; 10: 89-101
- 5 Bugg WG, Lewis M, Juette A, Cahir JG, Toms AP. Lumbar lordosis and pars interarticularis fractures: A case-control study. Skeletal Radiol 2012; 41: 817-22
- 6 Cassar-Pullicino VN, Davies AM. editors Measurements in Musculoskeletal Radiology. Springer-Verlag; 2020
- 7 Adams MA, Hutton WC. The effect of posture on the role of the apophysial joints in resisting intervertebral compressive forces. J Bone Joint Surg Br 1980; 62: 358-62
- 8 Chun S-W, Lim C-Y, Kim K, Hwang J, Chung SG. The relationships between low back pain and lumbar lordosis: A systematic review and meta-analysis. Spine J 2017; 17: 1180-91
- 9 Jentzsch T, Geiger J, König MA, Werner CML. Hyperlordosis is associated with facet joint pathology at the lower lumbar spine. Clin Spine Surg 2017; 30: 129-35
- 10 Ko S-B, Lee S-W. Prevalence of spondylolysis and its relationship with low back pain in selected population. Clin Orthop Surg 2011; 3: 34-8
- 11 Dhouib A, Tabard-Fougere A, Hanquinet S, Dayer R. Diagnostic accuracy of MR imaging for direct visualization of lumbar pars defect in children and young adults: A systematic review and meta-analysis. Eur Spine J 2018; 27: 1058-66
Address for correspondence
Publication History
Received: 13 May 2020
Accepted: 24 July 2020
Article published online:
19 July 2021
© 2020. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Private Ltd.
A-12, Second Floor, Sector -2, NOIDA -201301, India
-
References
- 1 Tansey P. Hip and low back pain in the presence of femoral anteversion. A case report. Man Ther 2015; 20: 206-11
- 2 Okuzu Y, Goto K, Okutani Y, Kuroda Y, Kawai T, Matsuda S. Hip-spine syndrome: Acetabular anteversion angle is associated with anterior pelvic tilt and lumbar hyperlordosis in patients with acetabular dysplasia: A retrospective study. JBJS Open Access 2019; 4: e0025
- 3 Leblebici G, Akalan E, Apti A, Kuchimov S, Kurt A, Onerge K. et al. Increased femoral anteversion-related biomechanical abnormalities: Lower extremity function, falling frequencies, and fatigue. Gait Posture 2019; 70: 336-40
- 4 Tawfik S, Phan K, Mobbs RJ, Rao PJ. The incidence of pars interarticularis defects in athletes. Glob Spine J 2020; 10: 89-101
- 5 Bugg WG, Lewis M, Juette A, Cahir JG, Toms AP. Lumbar lordosis and pars interarticularis fractures: A case-control study. Skeletal Radiol 2012; 41: 817-22
- 6 Cassar-Pullicino VN, Davies AM. editors Measurements in Musculoskeletal Radiology. Springer-Verlag; 2020
- 7 Adams MA, Hutton WC. The effect of posture on the role of the apophysial joints in resisting intervertebral compressive forces. J Bone Joint Surg Br 1980; 62: 358-62
- 8 Chun S-W, Lim C-Y, Kim K, Hwang J, Chung SG. The relationships between low back pain and lumbar lordosis: A systematic review and meta-analysis. Spine J 2017; 17: 1180-91
- 9 Jentzsch T, Geiger J, König MA, Werner CML. Hyperlordosis is associated with facet joint pathology at the lower lumbar spine. Clin Spine Surg 2017; 30: 129-35
- 10 Ko S-B, Lee S-W. Prevalence of spondylolysis and its relationship with low back pain in selected population. Clin Orthop Surg 2011; 3: 34-8
- 11 Dhouib A, Tabard-Fougere A, Hanquinet S, Dayer R. Diagnostic accuracy of MR imaging for direct visualization of lumbar pars defect in children and young adults: A systematic review and meta-analysis. Eur Spine J 2018; 27: 1058-66