
Subscribe to RSS
DOI: 10.4103/ijri.IJRI_145_19
A case report on granular cell ameloblastoma – A rare histological entity
Abstract
Granular cell ameloblastoma is a rare condition, accounting for 3.5% of all ameloblastoma cases that shows marked transformation in the cytoplasm of tumor cells, which are usually stellate reticulum-like cells. The transformed cells possess very coarse, granular eosinophilic cytoplasm. Granular cell ameloblastoma is aggressive in nature with a marked propensity for recurrence and can progress to metastasis. This article discusses a case report of a 35-year-old female patient diagnosed with granular cell ameloblastoma of the right mandible.
#
Introduction
Odontogenic tumors (OT) are a collection of heterogeneous lesions derived from epithelial and/or mesenchymal elements that are part of the tooth-forming apparatus.[[1]] Ameloblastoma is well-documented as a locally invasive benign neoplasm thought to ascend from the cellular components of the enamel organ.[[2]] An epithelial odontogenic tumor of the jaw that exhibits diverse microscopic patterns, which occurs either individually or in combination with other patterns.[[3]] The current World Health Organization (WHO2017) classification of odontogenic tumors divides ameloblastoma into four types as follows: ameloblastoma, unicystic type, ameloblastoma extraosseous or peripheral type, and metastasizing malignant.[[4]] Ameloblastoma most significantly concerns oral pathologists due to its high incidence among all odontogenic tumors and true neoplastic (infiltrative and recurrent) potential combined with its varieties of histopathological patterns.[[5]] The six main histopathological subtypes (variants) of ameloblastoma are as follows: (a) follicular, (b) plexiform, (c) acanthomatous, (d) granular cells, (e) basal cell, and (f) desmoplastic form.[[6]]
It is generally a painless, slow growing, locally aggressive tumor causing expansion of the cortical bone, perforation of the lingual or the buccal cortical plate and infiltration of the soft tissues. It has peak incidence in the third and fourth decade of life, but can be found in any age group with equal gender predilection (1:1). In the mandible, majority of ameloblastomas are found in the molar ramus region.[[7]] Granular cell ameloblastoma is one of the rarest entities and accounts for about 5% of all ameloblastomas.[[8]] Histopathologically, it is characterized by having numerous large eosinophilic granular cells.[[9]]
#
Case Report
A 35-year-old female patient visited the department of Oral Medicine and Radiology with a chief complaint of swelling in the right side of the face for the past 6 months. Patient was apparently normal one year ago. Then she noticed swelling in the right side of the face for which she consulted a dentist and got two teeth extracted from the right lower back tooth region. She gave a history that the swelling was subsided. Again, after 6 months she started to notice the swelling started in the same region, which was initially smaller in size and gradually increased to the present size. There was no history of pain associated with the swelling.
On extra oral examination, diffuse swelling was present on right side of the face measuring about 3 × 5 cm extending anteroposteriorly from the corner of the lip to the angle of the mandible and superoinferiorly from corner of the lip to 2 cm below the inferior border of the mandible [[Figure 1]]. Skin over the swelling was stretched and shiny. No ulcerations or discharge was present. Facial asymmetry was present on the Right side. On palpation, the swelling was hard in consistency and non-tender. Skin over the swelling was pinchable. Mouth opening was not restricted. Lymph node examination revealed two submandibular glands, which were palpable, both measuring 1 cm in diameter, firm in consistency, tender, and freely movable on the right side.

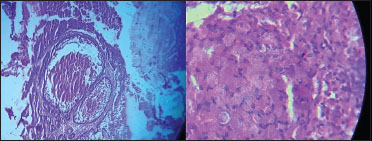
On intraoral examination, diffuse swelling involving the right lower alveolus extending from mesial aspect of 45 to retromolar trigone. There was obliteration of the buccal vestibule. Swelling was present on the lingual aspect extending to 1 cm above the floor of the mouth. The surface over the posterior aspect was erythematous and covered by white slough area [[Figure 2]]. No pus discharge or bleeding was present. On palpation, the swelling was soft to hard in consistency. Buccal and lingual cortical plate expansion was present. Provisionally diagnosed as benign tumor of the right mandible. Investigations carried out were panoramic radiography [[Figure 3]], computed tomography [[Figure 4]], blood investigations, and excisional biopsy. Panoramic Radiograph revealed a multilocular lesion in the right body of the mandible extending from the distal aspect of 43 extending to the right ramus of the mandible. There was destruction of inferior border and posterior border of ramus. Inferior alveolar canal was not appreciated. There was absence of resorption of roots 44, 45, 46. Computed tomography axial slice revealed diffuse expansile lesion in right side of the mandible with soft tissue enlargement of the same side. There was involvement of right angle and ramus of mandible with buccal and cortical plate destruction. 3D CT revealed the involvement of the right body, angle, and ramus of the mandible with bicortical plate expansion. Excisional biopsy was done [[Figure 5]] and specimen [[Figure 6]] was sent for histopathological examination, which revealed granular cell ameloblastoma of the right mandible [[Figure 7]].





#
Discussion
Churchill in 1934, defined ameloblastoma as unicentric, non functional, intermittently growing anatomically benign but clinically persistent tumor.[[10]] Granular cell change in ameloblastoma was first reported by Krompecher in 1918 and was called pseudoxanthomatous cells.[[11]] Granular cell ameloblastoma is an uncommon variant of ameloblastoma. Kameyama et al. stated in their clinico pathological study that only 1 out of 77 ameloblastoma cases was classified as Granular cell ameloblastoma.[[12]] Reichart et al. studied all accessible literature on ameloblastoma of the jaws from 1960 to 1993 and reported that out of a total of 1593 cases with available data on histologic subtypes, there were only 56 cases of the granular cell variant.[[13]]
The biological behavior of granular cell ameloblastoma does not seem to fluctuate from the other histologic subtypes of ameloblastoma; it can be locally aggressive and has a comparatively greater chance of recurrence.[[14]] Granular cell ameloblastoma is analyzed by the presence of granular cells, which characteristically occur within the central area of tumor and progressively replace the stellate reticulum.[[15]] The granular cells have an oval to polyhedral shape and tend to be large. The follicles may have a thin rim of stellate reticulum like cells that separates the granular cells from the peripheral columnar layer and the nucleus is displaced to the periphery of the cells. Conspicuous coarse granules pack and distend the cytoplasm and have a tendency to stain eosin, granting a notable manifestation. Occasionally, granular cell change may affect the peripheral columnar cells.[[16]] Ultrastructurally, the granular cells are consistent with lysosomes and are immunohistochemically positive for vimentin, CD68, muramidase, and bcl-2 and negative for cytokeratin and S-100 protein.[[17]]
Radiographically granular cell ameloblastoma resembles all the classical features of ameloblastoma. The most typical radiographic feature is that of a multilocular radiolucent lesion. The lesion is often described as having a “soap bubble” appearance (when the radiolucent loculations are large) or as being “honeycombed” (when the loculations are small). Buccal and lingual cortical expansion is frequently present. Resorption of the roots of teeth adjacent to the tumor is common. All the classical radiographic features were noted in our case except for root resorption. In many cases an unerupted tooth, most often a mandibular third molar is associated with the radiolucent defect.[[18]]
The granular cell tumor is an unusual benign soft tissue neoplasm that displays predilection for the oral cavity. The most common site is the tongue, followed by the buccal mucosa. Differential diagnosis from a granular cell ameloblastoma is necessary when there is peripheral localization or cortical perforation and soft tissue extension of the ameloblastoma. Granular cell tumor usually occurs in the fourth to sixth decades and shows a female predilection. Clinically, it appears as an asymptomatic sessile nodule of small size.[[18]]
#
Conclusion
Granular cell ameloblastoma is one of the rarest variant of ameloblastoma with unique and higher recurrence rate. However, it should be differentiated from the other granular cell lesions primarily because of its aggressiveness and higher recurrence rate. Patient has to be periodically reviewed because of its high recurrence rate.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
#
#
#
Conflict of Interest
There are no conflicts of interest.
-
References
- 1 Ladeinde AL, Ajayi OF, Ogunlewe MO, Adeyemo WL, Arotiba GT, Bamgbose BO. et al. Odontogenic tumors: A review of 319 cases in a Nigerian teaching hospital. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 99: 191-5
- 2 Thillaikarasi R, Balaji J, Gupta B, Ilayarja V, Vani NV, Vidula B. et al. Cystic granular cell ameloblastoma. J Maxillofac Oral Surg. 2010; 9: 310-3
- 3 Maria A, Sharma Y. Granular cell – Peripheral ameloblastoma: A rare variant. J Maxillofac Oral Surg 2009; 8: 294-7
- 4 Kulkarni D, Ingale Y, Ingale M, Ajabrao BN, Mayank M, Kulkarni A. Granular cell ameloblastoma: A rare case report and review of literature. Indian J Dent Res 2018; 29: 830-5
- 5 Philipsen HP, Reichart PA. Classification of odontogenic tumours. A historical review. J Oral Pathol Med 2006; 35: 525-9
- 6 Rajendran R. Cysts and tumors of odontogenic origin. In: Rajendran R, Shivapathsundaram S. editors Shafer’s Text Book of Oral Pathology. 5th Ed. New Delhi: Elsevier; 2006: 386
- 7 Vohra FA, Hussain M, Mudassir MS. Ameloblastomas and their management: A review. Pak J Surg 2009; 14: 136-42
- 8 Taneeru S, Guttikonda VR, Yeluri S, Madala J. Granular cell ameloblastoma of jaw – Report of a case with an emphasis on its characterization. J Clin Exp Dent 2013; 5: e154-6
- 9 Oza N, Agrawal K. Granular cell ameloblastoma mimicking oncocytoma. J Oral Maxillofac Pathol 2012; 16: 446-9
- 10 Ongole R, Praveen B. Oral Medicine, Oral Diagnosis and Oral Radiology. 2nd Ed. Elsevier Publications; 2013
- 11 Pardhe ND. Granular cell ameloblastoma: A rare entity. J Res Adv Dent 2014; 3: 137-41
- 12 Kameyama Y, Takehana S, Mizohata M, Nonobe K, Hara M, Kawai T. et al. A clinicopathological study of ameloblastomas. Int J Oral Maxillofac Surg 1987; 16: 706-12
- 13 Reichart PA, Philipsen HP, Sonner S. Ameloblastoma: Biological profile of 3677 cases. Eur J Cancer B Oral Oncol 1995; 31B: 86-99
- 14 Nikitakis NG, Tzerbos F, Triantafyllou K, Papadimas C, Sklavounou A. Granular cell ameloblastoma: An unusual histological subtype report and review of literature. J Oral Maxillofac Res 2010; 1: e3
- 15 Nasu M, Takagi M, Yamamoto H. Ultrastructural and histochemical studies of granular-cell ameloblastoma. J Oral Pathol 1984; 13: 448-56
- 16 Patankar SR, Mehta A. Granular cell ameloblastoma: A case report. Int J Oral Maxillofac Pathol 2011; 2: 63-7
- 17 Slater L. Granular cell ameloblastoma versus central odontogenic granular cell tumor. Oral Oncol 1997; 33: 145
- 18 Neville BW, Damm DD, Allen CM, Bouquot JE. Soft tissue tumors. In: Oral and Maxillofacial Pathology. 3rd ed. St Louis, Mo: W.B. Saunders; 2009: 537-8
Address for correspondence
Publication History
Received: 16 August 2019
Accepted: 19 February 2020
Article published online:
19 July 2021
© 2020. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Private Ltd.
A-12, Second Floor, Sector -2, NOIDA -201301, India
-
References
- 1 Ladeinde AL, Ajayi OF, Ogunlewe MO, Adeyemo WL, Arotiba GT, Bamgbose BO. et al. Odontogenic tumors: A review of 319 cases in a Nigerian teaching hospital. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 99: 191-5
- 2 Thillaikarasi R, Balaji J, Gupta B, Ilayarja V, Vani NV, Vidula B. et al. Cystic granular cell ameloblastoma. J Maxillofac Oral Surg. 2010; 9: 310-3
- 3 Maria A, Sharma Y. Granular cell – Peripheral ameloblastoma: A rare variant. J Maxillofac Oral Surg 2009; 8: 294-7
- 4 Kulkarni D, Ingale Y, Ingale M, Ajabrao BN, Mayank M, Kulkarni A. Granular cell ameloblastoma: A rare case report and review of literature. Indian J Dent Res 2018; 29: 830-5
- 5 Philipsen HP, Reichart PA. Classification of odontogenic tumours. A historical review. J Oral Pathol Med 2006; 35: 525-9
- 6 Rajendran R. Cysts and tumors of odontogenic origin. In: Rajendran R, Shivapathsundaram S. editors Shafer’s Text Book of Oral Pathology. 5th Ed. New Delhi: Elsevier; 2006: 386
- 7 Vohra FA, Hussain M, Mudassir MS. Ameloblastomas and their management: A review. Pak J Surg 2009; 14: 136-42
- 8 Taneeru S, Guttikonda VR, Yeluri S, Madala J. Granular cell ameloblastoma of jaw – Report of a case with an emphasis on its characterization. J Clin Exp Dent 2013; 5: e154-6
- 9 Oza N, Agrawal K. Granular cell ameloblastoma mimicking oncocytoma. J Oral Maxillofac Pathol 2012; 16: 446-9
- 10 Ongole R, Praveen B. Oral Medicine, Oral Diagnosis and Oral Radiology. 2nd Ed. Elsevier Publications; 2013
- 11 Pardhe ND. Granular cell ameloblastoma: A rare entity. J Res Adv Dent 2014; 3: 137-41
- 12 Kameyama Y, Takehana S, Mizohata M, Nonobe K, Hara M, Kawai T. et al. A clinicopathological study of ameloblastomas. Int J Oral Maxillofac Surg 1987; 16: 706-12
- 13 Reichart PA, Philipsen HP, Sonner S. Ameloblastoma: Biological profile of 3677 cases. Eur J Cancer B Oral Oncol 1995; 31B: 86-99
- 14 Nikitakis NG, Tzerbos F, Triantafyllou K, Papadimas C, Sklavounou A. Granular cell ameloblastoma: An unusual histological subtype report and review of literature. J Oral Maxillofac Res 2010; 1: e3
- 15 Nasu M, Takagi M, Yamamoto H. Ultrastructural and histochemical studies of granular-cell ameloblastoma. J Oral Pathol 1984; 13: 448-56
- 16 Patankar SR, Mehta A. Granular cell ameloblastoma: A case report. Int J Oral Maxillofac Pathol 2011; 2: 63-7
- 17 Slater L. Granular cell ameloblastoma versus central odontogenic granular cell tumor. Oral Oncol 1997; 33: 145
- 18 Neville BW, Damm DD, Allen CM, Bouquot JE. Soft tissue tumors. In: Oral and Maxillofacial Pathology. 3rd ed. St Louis, Mo: W.B. Saunders; 2009: 537-8