

RSS-Feed abonnieren
DOI: 10.4103/ajns.AJNS_539_20
Fourth ventricular epidermoid cyst – Case series, systematic review and analysis
Autor*innen

Background: Epidermoid cysts are extra-axial, pearly white avascular lesions mostly found in the cerebellopontine region. They are slow-growing and mostly become symptomatic when they attain significant size. They do occur at other anatomical locations, but fourth ventricle is a rare location. Three representative cases with their outcomes are described here. Methods: The systematic review was done with adherence to predefined criteria. The studied variables were age, gender, duration of symptoms (DOS), clinical features, hydrocephalus (HCP), extent of resection, postoperative complications, outcome, follow–up, and recurrence. Statistical analysis was done to identify predictive factors for outcome. Results: Final analysis included 58 studies containing 131 patients. The most common clinical feature was cerebellar dysfunction (93%). The most common cranial nerve involved was the abducens nerve (n = 37, 28.46%). Preoperative HCP was present in nearly a third (35%) of patients. The outcomes were not different with age (P = 0.23), gender (P = 0.74), DOS (P = 0.09), and HCP (P = 0.50). Improved outcomes were associated with total resections (P = 0.001), absence of preoperative cranial nerve dysfunctions (P = 0.004), and presentation with features of raised intracranial pressure (P = 0.005). Longer DOS (mean 76.74 months) was associated with significantly increased cranial nerve nuclei involvement (P = 0.03). Aseptic meningitis was reported in 14.5% of cases. Recurrences were infrequently reported (n = 9). Conclusions: Although the fourth ventricular epidermoid lesions are difficult to detect in an innocuous stage, when found, they should be extirpated early and totally, as a longer DOS leads to cranial nerve dysfunctions and suboptimal outcomes.
Introduction
Intracranial epidermoid cysts are avascular, pearly white, benign capsulated lesions with inner stratified squamous epithelium, accounting for <2% of all brain tumors.[[1]],[[2]],[[3]] They are thought to be congenital lesions, first described by Cruveilheir, a French pathologist in the early 18th century.[[3]],[[4]],[[5]],[[6]] They arise as epithelial sequestrations during the 3rd to 5th week of development and persist after neural tube closure.[[7]],[[8]] Their growth rate is linear to that of the epidermis.[[9]] They become symptomatic, usually in the second to fourth decades of life.[[5]],[[6]],[[10]] Tumor grows due to the accumulation of desquamated cells and their breakdown products such as keratin and cholesterol.[[7]] Unlike dermoid cyst, they are located off-midline. They are also more common than dermoid cysts.[[7]] About half of these intracranial lesions occur in the cerebellopontine angle.[[3]],[[6]],[[11]] Epidermoid cysts are the third most common lesion in this location after vestibular schwannomas and meningiomas.[[5]] Other common sites are sellar-suprasellar regions, Sylvian cisterns, basal cisterns, and interhemispheric regions.[[7]] Epidermoids in the fourth ventricle occur rarely. Because of its slow-growing nature and tendency to creep in between the neural structures without invading them, they often go unnoticed and become symptomatic only when large.[[9]],[[12]] Three of such cases are described here with a literature review and an analysis of data so found.
Case 1
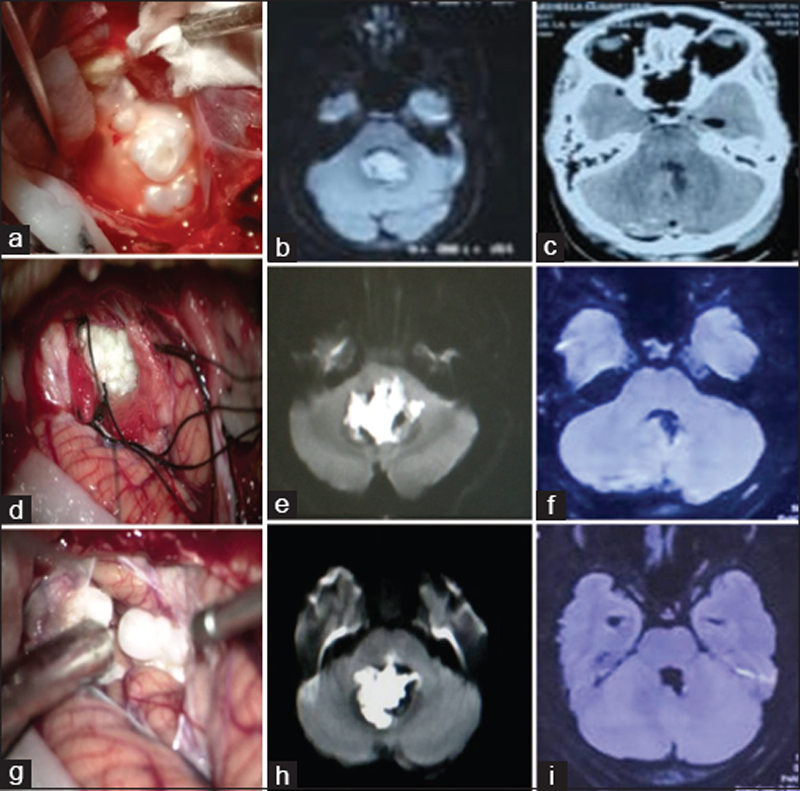
A 36-year-old female presented with mild suboccipital headache and nonpositional vertigo for 5 months. On clinical examination, she had intention tremors involving left upper limb and impaired finger to nose test. She had impaired tandem gait with a tendency to fall toward left. There were no cranial nerve deficits, and fundus examination was unremarkable. Magnetic resonance imaging (MRI) of the brain showed a multilobulated lesion filling the fourth ventricle's cavity, with an indentation on the brainstem and protruding out through the foramen of Magendie. The lesion was hypointense on T1-weighted image (T1WI) and hyperintense on T2WI, with no contrast enhancement. Diffusion restriction was present in the lesion, suggesting the diagnosis of epidermoid. There was no hydrocephalus (HCP) even though the fourth ventricle was filled with tumor. The patient underwent midline suboccipital craniotomy, and after dural opening, a pearly white tumor wrapped in arachnoid layers was evident at cistern magna. The tumor had displaced the tonsils laterally, filling the fourth ventricle and indenting its floor. After internal decompression, adhered capsular remnants were grasped and dissected away from brainstem using sharp dissection at the brain–tumor interface. Outmost care and patience were taken to avoid injury to critical neural elements on the fourth ventricle floor. The aqueductal opening was visible after tumor removal. The completeness of resection was confirmed with a 30° endoscope. The diagnosis of an epidermoid cyst was confirmed on histology. The patient was discharged on the postoperative day 6 without new neurological deficits. At 43 months of follow-up, there was no recurrence [[Figure 1]]a, [[Figure 1]]b, [[Figure 1]]c.
Case-2
A 46-year-old woman had diplopia for 2 years' duration. Diplopia was horizontal and worsened on looking toward left and on looking at distant objects. It resolved on closing the left eye. For this, she was prescribed glasses with a left eye patch. Over the last 6 months, her gait worsened, and she tended to fall toward left. She also had a mild headache. On examination, she had House and Brackmann Grade II facial palsy, left lateral rectus palsy, cerebellar ataxia, and nystagmus along with incoordination of the left side. On imaging, she had a lesion in the fourth ventricle, which was T1 hypointense with some areas of hyperintensity, T2 hyperintense, nonenhancing on contrast, and with diffusion restriction. There was no HCP. She underwent midline suboccipital craniotomy. After separating the tonsils and telovelar dissection, the tumor became visible. Most of the tumor was removed in a piecemeal fashion. The tumor had nubbin insinuating the facial colliculus, it could only be decompressed internally, and a small bit of densely adhered capsule was left behind. The fourth ventricular cavity was inspected with an endoscope. Her preoperative neurological status remained unchanged after surgery. She was discharged on day 8 of surgery. At 26 months of follow-up, her gait had improved, but facial palsy and sixth nerve palsy did not. Repeat MRI did not show any recurrence or areas of diffusion restriction even though a small piece of the capsule could not be removed during surgery [[Figure 1]]d, [[Figure 1]]e, [[Figure 1]]f.
Case 3
A 26-year-old female presented with a chronic headache of 1-year duration. Headache was intermittent, suboccipital, and increased on coughing without nausea or vomiting. On neurological examination, she had horizontal gaze-evoked nystagmus without any other neurological deficits. Her gait was normal. Computed tomography (CT) scan of the brain showed a hypodense lesion filling the cavity of the fourth ventricle without any HCP. MRI revealed T1 hypointense and T2 hyperintense lesion in the fourth ventricle with diffusion restriction. There was no contrast enhancement. The tumor was approached via midline suboccipital craniotomy. On opening the dura, the pearly white tumor wrapped in arachnoid layers was visible at the foramen of Magendie. We used the facial nerve, lower cranial nerve, and Somato Sensory Evoked Potential monitoring during surgery. The tumor was decompressed internally and dissected from neural structures. Small remnants of the capsule attached to the fourth ventricular floor were dissected carefully using the above-mentioned technique under neuromonitoring and maximum optical magnification, and total excision was achieved. The tumor bed was irrigated with dexamethasone saline. There were no new neural deficits or untoward complications in the postoperative period. She was discharged on day 6 postoperatively. At 8 months of follow-up, there were no recurrence and no new neurological deficits [[Figure 1]]g, [[Figure 1]]h, [[Figure 1]]i.
Methods
Protocol and registration
This systematic review was done with adherence to Preferred Reporting Items for Systematic Review and Meta-Analysis 2009 criteria throughout the study. The study protocol was predefined to search cases of epidermoid cyst in the fourth ventricle only. This study aimed to gather information and analyze data to manage cases of a fourth ventricular epidermoid cyst. The variable studied were age, gender, duration of symptoms (DOS), presenting symptoms and signs, presence or absence of HCP, extent of resection (EOR), complications, clinical outcomes, recurrence, and follow-up duration. This study being a purely retrospective review of literature, ethical approval was not sought for it. This study was neither funded nor registered with any agency.
Database search
No restrictions were imposed regarding publication date. All review articles, systematic review, meta-analysis, case series, and case reports of fourth ventricular epidermoid were included in the search. This literature review was done in June 2020 with a contribution by all authors. The keywords/MeSH terms searched were -”Epidermoid,” “Fourth ventricle,” “Epidermal cyst,” “Cholesteatoma,” “Keratin cyst,” “Pearly tumor,” “Intraventricular” individually and in combinations. The databases searched were PubMed, Web of Science, Cochrane, Scopus, Medline/Medscape, Ovid, Publons, ScienceDirect, Google Scholar, and Google General Search Engine. The references of selected articles were cross-checked and reviewed to improve the comprehensiveness and included if found eligible. The articles in non-English languages were also screened after Google translation and included if the full text was available. All abstracts and full articles were thoroughly reviewed.
In addition, articles available online, which had vital information, but not included in the indexing agencies, as mentioned above, were also included. Duplication of patients reported in multiple studies was also taken care of and excluded [[Figure 2]].

Inclusion criteria
-
The studies with human subjects
-
Studies that had substantial information (defined as at least 50% of the ten mentioned study parameters).
Exclusion criteria
-
Studies that do not have substantial information.
-
Cases associated with additional intracranial pathology-confounding factors for outcome
-
Recurrent cases
-
Duplication of patients in other studies.
Data synthesis
In the first step of the literature search, three authors independently searched different databases. Next, two senior authors further reviewed the three sets of selected articles. The articles found common in any of the three sets were included for screening. Two other authors further screened the rest of the articles. The articles thus selected for screening were further reviewed by the senior most authors for their eligibility as per inclusion and exclusion criteria. Disputes regarding the selection of articles were sorted out by voting. For quantitative assessment, clinical parameters were categorized into groups. The description of clinical signs and symptoms had some discrepancies and was categorized based on predefined criteria by authors. Likewise, all complications were categorized for quantitative assessment only. The EOR was labeled as subtotal if any part of the tumor or capsule was left behind. Surgical outcomes were recorded as mentioned in qualified studies and dichotomized between “improved” and “not improved” categories for analysis. Not improved category included death, worsened, and unchanged outcomes.
Statistical analysis
Statistical analysis was done using statistical packages for SPSS 25.0 for Windows (SPSS Inc., Chicago, IL, USA). Continuous and categorical variables were evaluated as mean ± standard deviation (SD). For qualitative analysis, all cases from selected articles were included, but studies with appropriate information were included only for quantitative analysis. Univariate descriptive analysis was done for all variables. Multivariate analysis was done using the Chi-square test and Fisher's exact test for categorical variables. Continuous variables were analyzed by independent t-test and Mann–Whitney U-tests. For multivariate analysis, stepwise logistic regression was applied to analyze the influence of variables on outcome. Two-tailed P values were considered statistically significant at P < 0.05.
Results
Database search results
A total of 836 studies were found on literature search with an above-described combination of MeSH terms (PubMed – 215, Web of Science – 47, Publons – 3, Medscape/Medline – 71, ScienceDirect – 66, Ovid – 16, Cochrane – 0, Google Scholar – 99, Scopus – 136, Google General Search – 183). Out of these 836 studies, 12 animal studies were excluded. There were 711 duplications of results. In 23 studies, the full text was not available, and 32 studies did not fulfill the inclusion criteria. Eight studies in other languages, which met the inclusion criteria, were included after Google translation.[[13]],[[14]],[[15]],[[16]],[[17]],[[18]],[[19]],[[20]] Fifty-eight studies having 131 cases were included in the final review. There was one systematic review,[[21]] 13 case series (3 or more cases),[[1]],[[7]],[[9]],[[12]],[[14]],[[15]],[[19]],[[22]],[[23]],[[24]],[[25]],[[26]],[[27]] and 44 case reports (<3 cases) [[Table 1]] and [[Figure 2]].




Descriptive analysis
Age
Individual data regarding age at presentation was available for 74 patients (50 studies). Case series, which described the mean age of the study population, were excluded from this statistical analysis. The mean age of presentation was 39.80 ± 12.92 years (median 41, range 12–71 years).
Gender
Data about gender were available for 111 patients (55 studies); there were more females (n = 64, 57.6%) than males (n = 47, 42.4%), with a ratio of 1.36:1.
Duration of symptoms
Data for DOS were available for 89 cases, out of which four case series comprising 30 patients described only their mean value. Thus, mean DOS ± SD was calculated for 59 patients. The mean DOS was 50.16 ± 87.63 months.
Clinical presentation
Data for clinical signs and symptoms were available for all patients, except one (n = 130, total signs and symptoms 336). For analysis, these symptoms were categorized as cerebellar, raised intracranial pressure (ICP), motor, sensory, cranial nerve palsy/paresis (CNP) I, CNP II, CNP III, CNP V, CNP VI, CNP VII, CNP, VIII, CNP lower cranial nerves (LCN), and others. Cerebellar signs and symptoms (n = 121/130, 93%) were the most common presentation, followed by cranial nerve involvement. Most commonly involved cranial nerves were VI (n = 37, 28.46%), II (n = 18, 13.84%), VIII (n = 17, 13%), VII (n = 16, 12.3%), and LCNs (n = 12, 9.2%). Cranial nerves V (n = 09), III (n = 08), and I (n = 02) were infrequently involved. The fourth ventricular epidermoid has a close relationship with the fourth ventricle floor and the underlying cranial nerve nuclei. Therefore, for multivariate analysis, the involvement of cranial nerve I and II was not considered. Features of raised ICP were seen in 74 (56.9%) patients. There were 18 (13.84%) patients with motor impairment, two patients with sensory symptoms, one asymptomatic, and one who had asthma. Individual outcomes could be calculated for 16 patients of motor impairment found in 12 studies, out of which 12 patients (75%) had improved outcomes.
Hydrocephalus
HCP was present in 46 (35.1%) cases of the cohort. As the HCP is an easily noticeable finding on radiological evaluation, for studies that did not mention their absence or presence (59 cases), it was presumed to have been absent. The preoperative ventriculo-peritoneal shunt was placed in 11 cases (23.9%).
Extent of resection
Data for the EOR were available for 121 patients in 52 studies, out of which 63 (52%) patients underwent total resection and 58 (48%) patients underwent subtotal resections. Subtotal resection was defined as leaving behind any trace of tumor or capsule.
Complications
Information about postoperative complications was available in 44 studies (110 patients). Most common complications were aseptic meningitis (AM, n = 16, 14.5%), cerebellar (n = 11, 10%), CNP VI (n = 10, 9%), CNP LCN (n = 9, 8.1%), CNP VII (n = 8, 7.2%), HCP (n = 7, 6.3%), CNP V (n = 1), and other nonneurological complications in 15 cases. Out of seven postoperative HCP, six required VP shunt postoperatively.
Outcome
Surgical outcomes were reported in 53 studies, including 125 patients. Ninety-five patients (76%) had improvement in symptoms, while 30 patients (24%) did not improve (unchanged – 18, death – 11, and worsen – 1).
Follow-up
Postoperative follow-up information was reported in 29 studies, including a total of 75 patients. The average follow-up duration was 30 months (range 1–194 months).
Recurrence
Information about recurrences was only reported in nine patients.
Multivariate analysis
Age
The mean age was not significantly different among males and females (70 patients, 48 studies). Mean age of presentation of males (n = 25) was 40.32 ± 15.29 years and for females (n = 45) was 39.11 ± 11.50 years (P = 0.87). There was a weak positive correlation between age and DOS (41 studies, n = 55, Pearson r value = 0.029, P = 0.025). Statistical significance was also not found between age and raised ICP (47 studies, 68 patients, P = 0.804), age and CNP (48 studies, 70 patients, P = 0.485), age and HCP (50 studies, 74 patients, P = 0.53), and age and outcomes (45 studies, 68 patients, P = 0.21). Age and EOR were analyzed for 65 patients from 45 studies. On the independent t-test, the mean age of patients who underwent subtotal resection (42.60 ± 11.30 years, standard error of the mean [SEM] = 2.13 years) was significantly higher (P = 0.04) than those who underwent total resection (36.351 ± 13.05 years, SEM = 2.14 years).
Gender
Analysis between gender and other variables did not reach statistical significance (gender with DOS – 41 studies, 55 patients, P = 0.164; gender with ICP – 50 studies, 81 patients, P = 0.655; gender with CNP – 51 studies, 94 patients, P = 0.83; gender with HCP – 52 studies, 92 patients, P = 0.84; gender with EOR – 44 studies, 64 patients, P = 0.15; gender with the outcome – 46 studies, 80 patients, P = 0.74).
Duration of symptoms
When DOS was analyzed concerning other variables, the only variable where statistical significance was present was with CNP (40 studies, 55 patients). Patients with CNP have significantly (P = 0.03) longer DOS (mean 76.740 ± 121.1 months) than patients who do not have CNP (mean 26.29 ± 38.35 months). Although the mean DOS with features of raised ICP was 38.06 ± 55.89 months in comparison to 68.96 ± 128.95 months without features of raised ICP, but this difference did not reach significance (39 studies, 53 patients, P = 0.233). There was no statistical significance in DOS with HCP (42 studies, 59 cases, P = 0.53). DOS was lesser in the improved group than the improved group (38 studies, 55 patients, mean DOS 40.01 months vs. 94.22 months); however, this difference did not reach statistical significance (P = 0.09).
Cranial nerve dysfunction
Multivariate analysis showed that preoperative cranial nerve dysfunction is significantly (P = 0.004) related to outcomes “not improved.” This significance was also confirmed on logistic regression (47 studies, 89 patients, P = 0.006). However, there was no significant difference with HCP (53 studies, 95 cases, P = 0.31) and with EOR (46 studies, 85 patients, P = 0.23). Likewise, the incidence of CNP was not significantly higher with features of raised ICP (53 studies, 95 patients, P = 0.08).
Hydrocephalus
Correlation of HCP with outcomes or with other variables did not reach statistical significance (HCP with EOR – 48 studies, 89 cases, P = 0.85 and HCP with the outcome – 50 studies, 101 patients, P = 0.50).
Outcome
The outcomes were significantly different among EOR, as total resection was better than subtotal resections (44 studies, including 89 patients, P = 0.001, logistic regression, P = 0.002). However, EOR did not significantly affect postoperative neurological complications, including AM (35 studies, 57 patients, P = 0.81). Outcomes were significantly better in patients presenting with raised ICP (48 studies, 97 patients, P = 0.005). Cross tabulation and statistical analysis of variables have been summarized in [[Table 2]].

Overall, the outcomes were affected by three variables – ICP, CNP, and EOR. When these factors were analyzed together in stepwise logistic regression, all were significant (P = 0.01, 0.01, and 0.03).
Discussion
As the fourth ventricle is a rare location for epidermoid cysts, randomized trials for this entity are far from possible, and all conclusions need to be drawn out of the information obtained from case series and case reports. There was only one available systematic review that analyzed the outcomes and the clinical variables. Chung et al. included only 23 studies and 37 patients and excluded certain cases with substantial information.[[21]] Our analysis included 58 studies, including 131 patients, which was much higher than the mentioned study. Chung et al. found longer age and DOS as predictors of outcome.[[21]] In our study, increasing age has significantly higher chances of subtotal resections, probably due to chronic presence, leading to adherences to neurological structures. The mean age, however, did not significantly affect the outcomes. Likewise, longer DOS significantly increased the chances of cranial nerve dysfunctions but did not affect outcomes. It is noticeable that the mean age of presentation and DOS are similar in both the reviews. Similarly, there were more females than males in both reviews.
The results of our study have few sharp contrasts compared to the study by Chung et al. In our study, 93% of patients had cerebellar signs and symptoms in comparison to 67.6% of patients in the study by Chung et al. Similarly, the percentage of cranial nerve dysfunctions and HCP was more in our study.[[21]] This difference is probably due to the inclusion of a higher number of patients for analysis in our study. Although fourth ventricular epidermoids fill up the fourth ventricle, HCP always does not occur. HCP was present in about one-third (35%) of patients in this cohort. It was postulated that cerebrospinal fluid seeps between the interstices of the tumor's capsule and maintains the outflow.[[1]],[[5]],[[9]],[[22]],[[49]] Some authors had reported remission of symptoms once the tumor extrudes through the foramen of the fourth ventricle.[[9]],[[24]]
This analysis explored possible associations between multiple variables and their effects on outcomes. The only predictors affecting outcomes were presence of features of raised ICP, preoperative cranial nerve dysfunctions, and the EOR. As decompression of these lesions restores the CSF flow, symptoms of raised ICP are almost immediately relieved. Presence of cranial nerve palsy often suggests brainstem involvement and heralds poor outcome. Epidermoids, being extra-axial and avascular lesions, are generally considered easy to remove surgically, but this is not always so in cases of fourth ventricular epidermoids.[[24]],[[48]] Adherence of the capsule to vital neurological structures, especially with brainstem and its nuclei, often leads to subtotal resections.[[1]],[[12]],[[21]],[[24]],[[25]] Many surgeons prefer subtotal resection in such cases, but this analysis emphasizes the role of total resections. Authors do not debate the importance of patient safety during surgery, but total removal is often possible under neuromonitoring in selected cases with meticulous dissection. Careful dissection of the capsule from arachnoid layers is the surgical pearl for removing this pearly tumor.[[26]] Endoscopic assistance may help visualize tumors in otherwise inaccessible areas.[[51]] The risks associated with total resection attempts should not outweigh the benefits, and subtotal removal may be justified in some cases.[[9]],[[25]],[[27]] We analyzed the risks of postoperative neurological and tumor-specific complications such as AM and found that total resections were not associated with higher complications, contrary to popular belief. During the internal decompression, every effort to avoid spillage of the tumor needs consideration. Spillage and incomplete removal may cause AM requiring steroids.[[4]],[[35]] However, in this review, only 16 patients (14.5%) had AM.[[1]],[[4]],[[6]],[[9]],[[13]],[[24]],[[26]],[[36]],[[38]],[[48]],[[51]],[[57]]
Incomplete resection may lead to late recurrences requiring surgery.[[1]] As previously mentioned, there is scarce reporting of recurrences; only nine cases were reported in the literature at a mean follow-up period of 30 months.[[1]],[[12]],[[24]],[[26]] Scott et al. mentioned the most prolonged duration of follow-up (194 months), and after total resection, there was no recurrence; however, after a mean follow-up duration of 174 months, Tancredi et al. observed three recurrences in seven subtotal resections.[[1]],[[28]] In one of our patients, where a tiny piece of capsule adherent to the brainstem was left behind, 26 months of follow-up did not show recurrence on MRI. However, we agree that with this short follow-up duration for such a slow-growing tumor, it is not prudent to conclude the incidence of recurrence.
Before advancements in technology, neurosurgeons did not have the luxury of imaging tools available today. In the pre-CT era, most cases were diagnosed on plain X-ray, pneumo-encephalogram, ventriculogram, and arteriogram.[[13]],[[36]] Evolution of imaging modalities has led to early detection of these lesions and prompt reporting. On CT, epidermoids appear as nonenhancing hypodense lesions with mass effect.[[29]] CT may show calcification at times.[[30]] MRI has now become the diagnostic modality of choice.[[5]],[[6]],[[8]] Epidermoids are hypointense on T1WI and heterogeneously hyperintense on T2WI. When protein and triglyceride contents of tumors are high, they appear hyperintense on T1WI and are known as “white epidermoids.”[[5]],[[53]] These lesions are well encapsulated and insinuate into cisterns. Due to their slow-growing nature, they deform the surrounding structures, and despite significant compression, perilesional edema is absent. They do not enhance with gadolinium and show diffusion restriction.[[37]] In the fourth ventricle, they produce signals similar to CSF on T2WI and can be differentiated by the absence of suppression on FLAIR images.[[5]],[[44]] Pathological slides show a nuclear attenuated squamous epithelium without atypia. Unlike in dermoid cyst, dermal inclusion structures are absent. Malignant changes are rare.[[5]],[[33]]
Limitations
The study, being retrospective in nature, has certain limitations. Some studies published in radiological journals got excluded as they did not qualify the inclusion criteria due to limited clinical information. Factors such as age, DOS, and follow-up durations were described as mean in some case series and get excluded from the final statistical analysis. Data for DOS were missing in many studies. Clinical signs and symptoms have been described vaguely in different studies, thus needed categorization for the statistical analysis.
. Further, certain symptoms may be attributed to more than one neurological structure and were categorized based on the authors' opinion, which may vary. One such example is “nystagmus and ataxia;” both may be attributed to either cerebellar or vestibular dysfunction or both. The information about the presence or absence of HCP was incomplete in many studies. As HCP is hard to miss finding on imaging, authors presumed their absence in cases where this description was absent. Likewise, the EOR was described in various studies as total or gross total resection even when “some part of the capsule” was left behind. In our analysis, any part of the tumor or capsule left behind was considered as subtotal resection. Postoperative complications, follow-up duration, and recurrences were scarcely mentioned in studies.
Conclusions
The fourth ventricle epidermoid is a relatively rare entity. Determining its incidence is, therefore, difficult at this stage. Our study determined that total resection and preoperative absence of cranial nerve involvement predicted better postoperative outcomes in such patients. In addition, a longer DOS was associated with higher chances of cranial nerve nuclei involvement. Early detection of this innocuously slow-growing tumor may not be feasible but, when found, needs adequate surgical resection to help improve outcomes.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the legal guardian has given his consent for images and other clinical information to be reported in the journal. The guardian understands that names and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Acknowledgments
Authors would like to thank Dr. Shashank Nahar and Dr. Naman Chandrakar (MCh students), Department of Neurosurgery, DKS Post Graduate Institute and Research Center, for their helpful suggestions and motivations during the writing of this manuscript. The suggestions and statistical analysis by Dr. Kittu Jain were invaluable to the completion of this review. Authors are also thankful to Dr. Hemant Sharma, Assistant Superintendent, for providing optimal library assess for literature search and statistical analysis.
Financial support and sponsorship
Nil.
-
References
- 1 Tancredi A, Fiume D, Gazzeri G. Epidermoid cysts of the fourth ventricle: Very long follow up in 9 cases and review of the literature. Acta Neurochir (Wien) 2003;145:905-10.
- 2 Kambe A, Anno Y, Oda N, Shiomi Y, Aoki H, Sasaki A. Reversible bilateral vestibular impairment caused by fourth ventricle epidermoid tumor. Neurol Med Chir (Tokyo) 2003;43:201-3.
- 3 Cardoso AC, Lemos LE, Marques MA. Epidermoid cyst located in the fourth ventricle: Case report and review. Braz Neurosurg 2016;35:174-7.
- 4 Cantu RC, Ojemann RG. Glucosteroid treatment of keratin meningitis following removal of a fourth ventricle epidermoid tumour. J Neurol Neurosurg Psychiatry 1968;31:73-5.
- 5 Forghani R, Farb RI, Kiehl TR, Bernstein M. Fourth ventricle epidermoid tumor: Radiologic, intraoperative, and pathologic findings. Radiographics 2007;27:1489-94.
- 6 Bryl M, Czapiga B, Gosztyla MK, Halon A. Fourth ventricle epidermoid cyst – A cases report. Aktulan Neurol 2018;18:177-82.
- 7 Bini W, Sepehmia A, Dündar M, Samii M. Epidermoid tumors of the IV ventricle: Report of 3 cases. Neurocirugía 1993;4:205-10.
- 8 Bohara M, Yonezawa H, Hanaya R, Takeshita S, Sumida M, Arita K. Posterior fossa epidermoid cysts presenting with unusual radiological appearances – Two case reports. Neurol Med Chir (Tokyo) 2011;51:85-8.
- 9 Nassar SI, Haddad FS, Abdo A. Epidermoid tumors of the fourth ventricle. Surg Neurol 1995;43:246-51.
- 10 Pepus M, Hutcheson JB, Tamayo JL. Pearly tumor of the fourth ventricle. South Med J 1968;61:487-90.
- 11 Alpers BJ. The cerebral epidermoids (cholesteatomas). Am J Surg 1939;43:55-65.
- 12 Gopalakrishnan CV, Ansari KA, Nair S, Menon G. Long term outcome in surgically treated posterior fossa epidermoids. Clin Neurol Neurosurg 2014;117:93-9.
- 13 Gellad F, Rao KC, Arora S, Chiantella N, Salcman M. Epidermoid tumor of the fourth ventricle: Use of metrizamide-computed tomography. J Comput Tomogr 1982;6:231-5.
- 14 Isla A, Alvarez F, Higueras AP, Blázquez MG. Quistes epidermoides intracraneales: Revision de 16 casos [Intracranial epidermoid cyst: Review of 16 cases]. Neurocirugia 1990;1:209-17.
- 15 Taguchi Y, Yamaguchi Y, Sekino H, Sakurai T, Hayashi T, Sakamoto T. Epidermoid tumor of the forth ventricle: Clinical features and surgical treatment. Jpn J Neurosurg 1997;6:513-19.
- 16 Hila H, Bouhaouala MH, Darmol M, Jelassi H, Yedeas M. Kyste épidermoïde vermien révélé par un traumatisme crânien [Vermian epidermoid cyst revealed by head injury]. Neurochirurgie 2006;52:63-6.
- 17 Trijolet JP, Pondaven-Letourmy S, Robier A, Morinière S. Vertige positionnel paroxystique découvrant un kyste épidermoïde du quatrième ventricule [Epidermoid cysts of the fourth ventricle mimicking benign paroxysmal positional vertigo]. Ann Otolaryngol Chir Cervicofac 2008;125:146-50.
- 18 Aggouri M, Moussaoui A, Benzagmout M, Chakour K, Chaoui ME. Kyste epidermoïde du quatrieme ventricule: A propos d'un cas [Epidermoid cyst of the fourth ventricle: Case report]. Afr J Neurol Sci 2010;29:64-8.
- 19 Moumen N, Maroudi AE, Hassani RE, Chakir N, Jiddane M. Kystes épidermoïdes de la grande citerne et du quatrième ventricule [Epidermoid cysts of the cisterna magna and fourth ventricle]. Feuill Radiol 2010;50:313-8.
- 20 Oulali N, Moufid F, Ghailan MR, Hosni B. Kyste epidermoïde de la grande citerne et du quatrieme ventricule [Epidermoid cyst of the cisterna magna and fourth ventricle]. Pan Afr Med J 2012;13:19.
- 21 Chung LK, Beckett JS, Ong V, Lagman C, Nagasawa DT, Yang I, et al. Predictors of outcomes in fourth ventricular epidermoid cysts: A case report and a review of literature. World Neurosurg 2017;105:689-96.
- 22 Rosario M, Becker DH, Conley FK. Epidermoid tumors involving the fourth ventricle. Neurosurgery 1981;9:9-13.
- 23 Sabin HI, Bordi LT, Symon L. Epidermoid cysts and cholesterol granulomas centered on the posterior fossa: Twenty years of diagnosis and management. Neurosurgery 1987;21:798-805.
- 24 Lunardi P, Missori P, Gagliardi FM, Fortuna A. Epidermoid tumors of the 4th ventricle: Report of seven cases. Neurosurgery 1990;27:532-4.
- 25 Talacchi A, Sala F, Alessandrini F, Turazzi S, Bricolo A. Assessment and surgical management of posterior fossa epidermoid tumors: Report of 28 cases. Neurosurgery 1998;42:242-51.
- 26 Meng L, Yuguang L, Shugan Z, Xingang L, Chengyuan W. Intraventricular epidermoids. J Clin Neurosci 2006;13:428-30.
- 27 Raghunath A, Devi BI, Bhat DI, Somanna S. Unusual complications of a benign tumour-Our experience with midline posterior fossa epidermoids. Br J Neurosurg 2013;27:69-73.
- 28 Scott M. Epidermoid tumour (tumor perlée, cholesteatoma) of the fourth ventricle: Case report and review of literature. J Neurol Neurosurg Psychiatry 1974;37:1329-32.
- 29 Davis KR, Roberson GH, Taveras JM, New PF, Trevor R. Diagnosis of epidermoid tumor by computed tomography. Analysis and evaluation of findings. Radiology 1976;119:347-53.
- 30 Fawcitt RA, Isherwood I. Radiodiagnosis of intracranial pearly tumours with particular reference to the value of computer tomography. Neuroradiology 1976;11:235-42.
- 31 Hanamura T, Amano K, Hatanaka H, Tsukagoshi H. A case of epidermoid of the fourth ventricle. J Neurol 1978;219:145-9.
- 32 Schraeder PL, Cohen MM, Goldman W. Bilateral internuclear ophthalmoplegia associated with fourth ventricular epidermoid tumor. Case report. J Neurosurg 1981;54:403-5.
- 33 Dubois PJ, Sage M, Luther JS, Burger PC, Heinz ER, Drayer BP. Case report. Malignant change in an intracranial epidermoid cyst. J Comput Assist Tomogr 1981;5:433-5.
- 34 Imamura Y, Ninchoji T, Nakajima S, Uemura K. Epidermoid tumor in the fourth ventricle, with particular reference to metrizamide CT cisternography findings. Surg Neurol 1982;18:444-7.
- 35 Salazar J, Vaquero J, Saucedo G, Bravo G. Posterior fossa epidermoid cysts. Acta Neurochir (Wien) 1987;85:34-9.
- 36 Bret P, Remond J, Fischer C, Fischer G, Kzaiz M. Epidermoid cyst of the fourth ventricle. Br J Neurosurg 1988;2:109-13.
- 37 Yuh WT, Barloon TJ, Jacoby CG, Schultz DH. MR of fourth-ventricular epidermoid tumors. AJNR Am J Neuroradiol 1988;9:794-6.
- 38 Iihara K, Kikuchi H, Ishikawa M, Nagasawa S. Epidermoid cyst traversing the pons into the fourth ventricle. Case report. Surg Neurol 1989;32:377-81.
- 39 Yamakawa K, Shitara N, Genka S, Manaka S, Takakura K. Clinical course and surgical prognosis of 33 cases of intracranial epidermoid tumors. Neurosurgery 1989;24:568-73.
- 40 Sakamoto M, Seo Y, Fukami T, Matsumoto K. A case of epidermoid in the fourth ventricle associated with bronchial asthma-like symptom. No Shinkei Geka 1989;17:663-8.
- 41 Wagle WA, Jaufmann B, Mincy JE. Magnetic resonance imaging of fourth ventricular epidermoid tumors. Arch Neurol 1991;48:438-40.
- 42 Misra AK, Mishra SK, Ortiz W. Differential involvement of brainstem pathways due to fourth ventricular epidermoid cyst: A case study. Clin Neurol Neurosurg 1994;96:170-3.
- 43 Jeon JY, Kim JM, Cheong JH, Kim CH. Epidermoid cyst of the forth ventricle. J Korean Neurosurg Soc 2005;38:478-80.
- 44 Cekic PY, Evlice AO, Sener RN. Epidermoid tumor in the fourth ventricle. J Pediatr Neurol 2005;03:195-6.
- 45 Lauvin-Gaillard MA, Legeais M, Velut S, François P, Bergemer-Fouquet AM, Bibi R, et al. Epidermoid cyst of the fourth ventricle. J Radiol 2009;90:618-21.
- 46 Agrawal A, Borle RM, Bhola N, Daga A, Bora S, Sachdeva S. Multiple fractures involving the orbit and incidental finding of large fourth ventricular epidermoid. J Craniofac Surg 2009;20:261-2.
- 47 Su CH, Young YH. Disorders affecting the fourth ventricle: Etiology and clinical correlates. Otol Neurotol 2011;32:1329-35.
- 48 Mathai KI, Bhatia K, Hashim PI. Epidermoid tumour of 4th ventricle: A case report and review of literature. J Marine Med Soc 2013;15:121-2.
- 49 Chowdhury FH, Haque MR, Sarker MH. Intracranial epidermoid tumor; microneurosurgical management: An experience of 23 cases. Asian J Neurosurg 2013;8:21-8.
- 50 Sengupta SK, Singh P. Cerebellar vermian epidermal cyst. Med J Armed Forces India 2015;71:S166-8.
- 51 Tuchman A, Platt A, Winer J, Pham M, Giannotta S, Zada G. Endoscopic-assisted resection of intracranial epidermoid tumors. World Neurosurg 2014;82:450-4.
- 52 Taschner CA, Erny D, Weyerbrock A, Urbach H, Maurer C, Prinz M. Freiburg neuropathology case conference. A mass lesion of the fourth ventricle. Clin Neuroradiol 2015;25:439-43.
- 53 Patil A, Kulkarni V, Singh G, Sehrawat P. Fourth ventricle epidermoid tumor: Radiologic findings. Med J DY Patil Univ 2016;9:136-9.
- 54 Akcakaya MO, Altunrende ME, Navruz Y, Ozlu HM, Canpolat A, Akdemir O. Epidermoid tumor of the forth ventricle with accompanying congenital posterior arch effect of the atlas. J Nervous Sys Surgery 2016;6:47-51.
- 55 Kokkalis P, Chamilos C, Sgouros S. Epidermoid cyst of the fourth ventricle in a child. Childs Nerv Syst 2018;34:29-30.
- 56 Veretennikoff K, Coyne T, Biggs V, Robinson GA. Executive dysfunction after fourth-ventricle epidermoid cyst resection. Cogn Behav Neurol 2018;31:207-13.
- 57 Kaba DI, Maati A, Dianka MB, Camara AM, Bocco AF, Chellaoui A, et al. The fourth ventricle epidermoid cyst: About two cases. J Med Res 2019;5:165-8.
- 58 Kumar S, Sharma S, Misra R, Kumar K. Epidermoid cyst of the fourth ventricle: A case report. Indian J Neurosurg 2019;8:191-2.
- 59 Hossini A, Lakhdar F, Gana R, Maaqili MR, Saïdi A, Jiddane M, et al. Epidermoid cyst of the cisterna magna and the fourth ventricle: Report of four cases. Neurochirurgie 2012;58:358-63.
- 60 El Saqui A, Aggouri M, Benzagmout M, Chakour K, Chaoui ME. Fourth ventricule epidermoid cyst: About a case. Pan Afr Med J 2017;26:239.
- 61 Fiume D, Gazzeri G, Spallone A, Santucci N. Epidermoid cysts of the fourth ventricle. Surg Neurol 1988;29:178-82.
Address for correspondence
Publikationsverlauf
Eingereicht: 12. November 2020
Angenommen: 14. September 2021
Artikel online veröffentlicht:
16. August 2022
© 2021. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Tancredi A, Fiume D, Gazzeri G. Epidermoid cysts of the fourth ventricle: Very long follow up in 9 cases and review of the literature. Acta Neurochir (Wien) 2003;145:905-10.
- 2 Kambe A, Anno Y, Oda N, Shiomi Y, Aoki H, Sasaki A. Reversible bilateral vestibular impairment caused by fourth ventricle epidermoid tumor. Neurol Med Chir (Tokyo) 2003;43:201-3.
- 3 Cardoso AC, Lemos LE, Marques MA. Epidermoid cyst located in the fourth ventricle: Case report and review. Braz Neurosurg 2016;35:174-7.
- 4 Cantu RC, Ojemann RG. Glucosteroid treatment of keratin meningitis following removal of a fourth ventricle epidermoid tumour. J Neurol Neurosurg Psychiatry 1968;31:73-5.
- 5 Forghani R, Farb RI, Kiehl TR, Bernstein M. Fourth ventricle epidermoid tumor: Radiologic, intraoperative, and pathologic findings. Radiographics 2007;27:1489-94.
- 6 Bryl M, Czapiga B, Gosztyla MK, Halon A. Fourth ventricle epidermoid cyst – A cases report. Aktulan Neurol 2018;18:177-82.
- 7 Bini W, Sepehmia A, Dündar M, Samii M. Epidermoid tumors of the IV ventricle: Report of 3 cases. Neurocirugía 1993;4:205-10.
- 8 Bohara M, Yonezawa H, Hanaya R, Takeshita S, Sumida M, Arita K. Posterior fossa epidermoid cysts presenting with unusual radiological appearances – Two case reports. Neurol Med Chir (Tokyo) 2011;51:85-8.
- 9 Nassar SI, Haddad FS, Abdo A. Epidermoid tumors of the fourth ventricle. Surg Neurol 1995;43:246-51.
- 10 Pepus M, Hutcheson JB, Tamayo JL. Pearly tumor of the fourth ventricle. South Med J 1968;61:487-90.
- 11 Alpers BJ. The cerebral epidermoids (cholesteatomas). Am J Surg 1939;43:55-65.
- 12 Gopalakrishnan CV, Ansari KA, Nair S, Menon G. Long term outcome in surgically treated posterior fossa epidermoids. Clin Neurol Neurosurg 2014;117:93-9.
- 13 Gellad F, Rao KC, Arora S, Chiantella N, Salcman M. Epidermoid tumor of the fourth ventricle: Use of metrizamide-computed tomography. J Comput Tomogr 1982;6:231-5.
- 14 Isla A, Alvarez F, Higueras AP, Blázquez MG. Quistes epidermoides intracraneales: Revision de 16 casos [Intracranial epidermoid cyst: Review of 16 cases]. Neurocirugia 1990;1:209-17.
- 15 Taguchi Y, Yamaguchi Y, Sekino H, Sakurai T, Hayashi T, Sakamoto T. Epidermoid tumor of the forth ventricle: Clinical features and surgical treatment. Jpn J Neurosurg 1997;6:513-19.
- 16 Hila H, Bouhaouala MH, Darmol M, Jelassi H, Yedeas M. Kyste épidermoïde vermien révélé par un traumatisme crânien [Vermian epidermoid cyst revealed by head injury]. Neurochirurgie 2006;52:63-6.
- 17 Trijolet JP, Pondaven-Letourmy S, Robier A, Morinière S. Vertige positionnel paroxystique découvrant un kyste épidermoïde du quatrième ventricule [Epidermoid cysts of the fourth ventricle mimicking benign paroxysmal positional vertigo]. Ann Otolaryngol Chir Cervicofac 2008;125:146-50.
- 18 Aggouri M, Moussaoui A, Benzagmout M, Chakour K, Chaoui ME. Kyste epidermoïde du quatrieme ventricule: A propos d'un cas [Epidermoid cyst of the fourth ventricle: Case report]. Afr J Neurol Sci 2010;29:64-8.
- 19 Moumen N, Maroudi AE, Hassani RE, Chakir N, Jiddane M. Kystes épidermoïdes de la grande citerne et du quatrième ventricule [Epidermoid cysts of the cisterna magna and fourth ventricle]. Feuill Radiol 2010;50:313-8.
- 20 Oulali N, Moufid F, Ghailan MR, Hosni B. Kyste epidermoïde de la grande citerne et du quatrieme ventricule [Epidermoid cyst of the cisterna magna and fourth ventricle]. Pan Afr Med J 2012;13:19.
- 21 Chung LK, Beckett JS, Ong V, Lagman C, Nagasawa DT, Yang I, et al. Predictors of outcomes in fourth ventricular epidermoid cysts: A case report and a review of literature. World Neurosurg 2017;105:689-96.
- 22 Rosario M, Becker DH, Conley FK. Epidermoid tumors involving the fourth ventricle. Neurosurgery 1981;9:9-13.
- 23 Sabin HI, Bordi LT, Symon L. Epidermoid cysts and cholesterol granulomas centered on the posterior fossa: Twenty years of diagnosis and management. Neurosurgery 1987;21:798-805.
- 24 Lunardi P, Missori P, Gagliardi FM, Fortuna A. Epidermoid tumors of the 4th ventricle: Report of seven cases. Neurosurgery 1990;27:532-4.
- 25 Talacchi A, Sala F, Alessandrini F, Turazzi S, Bricolo A. Assessment and surgical management of posterior fossa epidermoid tumors: Report of 28 cases. Neurosurgery 1998;42:242-51.
- 26 Meng L, Yuguang L, Shugan Z, Xingang L, Chengyuan W. Intraventricular epidermoids. J Clin Neurosci 2006;13:428-30.
- 27 Raghunath A, Devi BI, Bhat DI, Somanna S. Unusual complications of a benign tumour-Our experience with midline posterior fossa epidermoids. Br J Neurosurg 2013;27:69-73.
- 28 Scott M. Epidermoid tumour (tumor perlée, cholesteatoma) of the fourth ventricle: Case report and review of literature. J Neurol Neurosurg Psychiatry 1974;37:1329-32.
- 29 Davis KR, Roberson GH, Taveras JM, New PF, Trevor R. Diagnosis of epidermoid tumor by computed tomography. Analysis and evaluation of findings. Radiology 1976;119:347-53.
- 30 Fawcitt RA, Isherwood I. Radiodiagnosis of intracranial pearly tumours with particular reference to the value of computer tomography. Neuroradiology 1976;11:235-42.
- 31 Hanamura T, Amano K, Hatanaka H, Tsukagoshi H. A case of epidermoid of the fourth ventricle. J Neurol 1978;219:145-9.
- 32 Schraeder PL, Cohen MM, Goldman W. Bilateral internuclear ophthalmoplegia associated with fourth ventricular epidermoid tumor. Case report. J Neurosurg 1981;54:403-5.
- 33 Dubois PJ, Sage M, Luther JS, Burger PC, Heinz ER, Drayer BP. Case report. Malignant change in an intracranial epidermoid cyst. J Comput Assist Tomogr 1981;5:433-5.
- 34 Imamura Y, Ninchoji T, Nakajima S, Uemura K. Epidermoid tumor in the fourth ventricle, with particular reference to metrizamide CT cisternography findings. Surg Neurol 1982;18:444-7.
- 35 Salazar J, Vaquero J, Saucedo G, Bravo G. Posterior fossa epidermoid cysts. Acta Neurochir (Wien) 1987;85:34-9.
- 36 Bret P, Remond J, Fischer C, Fischer G, Kzaiz M. Epidermoid cyst of the fourth ventricle. Br J Neurosurg 1988;2:109-13.
- 37 Yuh WT, Barloon TJ, Jacoby CG, Schultz DH. MR of fourth-ventricular epidermoid tumors. AJNR Am J Neuroradiol 1988;9:794-6.
- 38 Iihara K, Kikuchi H, Ishikawa M, Nagasawa S. Epidermoid cyst traversing the pons into the fourth ventricle. Case report. Surg Neurol 1989;32:377-81.
- 39 Yamakawa K, Shitara N, Genka S, Manaka S, Takakura K. Clinical course and surgical prognosis of 33 cases of intracranial epidermoid tumors. Neurosurgery 1989;24:568-73.
- 40 Sakamoto M, Seo Y, Fukami T, Matsumoto K. A case of epidermoid in the fourth ventricle associated with bronchial asthma-like symptom. No Shinkei Geka 1989;17:663-8.
- 41 Wagle WA, Jaufmann B, Mincy JE. Magnetic resonance imaging of fourth ventricular epidermoid tumors. Arch Neurol 1991;48:438-40.
- 42 Misra AK, Mishra SK, Ortiz W. Differential involvement of brainstem pathways due to fourth ventricular epidermoid cyst: A case study. Clin Neurol Neurosurg 1994;96:170-3.
- 43 Jeon JY, Kim JM, Cheong JH, Kim CH. Epidermoid cyst of the forth ventricle. J Korean Neurosurg Soc 2005;38:478-80.
- 44 Cekic PY, Evlice AO, Sener RN. Epidermoid tumor in the fourth ventricle. J Pediatr Neurol 2005;03:195-6.
- 45 Lauvin-Gaillard MA, Legeais M, Velut S, François P, Bergemer-Fouquet AM, Bibi R, et al. Epidermoid cyst of the fourth ventricle. J Radiol 2009;90:618-21.
- 46 Agrawal A, Borle RM, Bhola N, Daga A, Bora S, Sachdeva S. Multiple fractures involving the orbit and incidental finding of large fourth ventricular epidermoid. J Craniofac Surg 2009;20:261-2.
- 47 Su CH, Young YH. Disorders affecting the fourth ventricle: Etiology and clinical correlates. Otol Neurotol 2011;32:1329-35.
- 48 Mathai KI, Bhatia K, Hashim PI. Epidermoid tumour of 4th ventricle: A case report and review of literature. J Marine Med Soc 2013;15:121-2.
- 49 Chowdhury FH, Haque MR, Sarker MH. Intracranial epidermoid tumor; microneurosurgical management: An experience of 23 cases. Asian J Neurosurg 2013;8:21-8.
- 50 Sengupta SK, Singh P. Cerebellar vermian epidermal cyst. Med J Armed Forces India 2015;71:S166-8.
- 51 Tuchman A, Platt A, Winer J, Pham M, Giannotta S, Zada G. Endoscopic-assisted resection of intracranial epidermoid tumors. World Neurosurg 2014;82:450-4.
- 52 Taschner CA, Erny D, Weyerbrock A, Urbach H, Maurer C, Prinz M. Freiburg neuropathology case conference. A mass lesion of the fourth ventricle. Clin Neuroradiol 2015;25:439-43.
- 53 Patil A, Kulkarni V, Singh G, Sehrawat P. Fourth ventricle epidermoid tumor: Radiologic findings. Med J DY Patil Univ 2016;9:136-9.
- 54 Akcakaya MO, Altunrende ME, Navruz Y, Ozlu HM, Canpolat A, Akdemir O. Epidermoid tumor of the forth ventricle with accompanying congenital posterior arch effect of the atlas. J Nervous Sys Surgery 2016;6:47-51.
- 55 Kokkalis P, Chamilos C, Sgouros S. Epidermoid cyst of the fourth ventricle in a child. Childs Nerv Syst 2018;34:29-30.
- 56 Veretennikoff K, Coyne T, Biggs V, Robinson GA. Executive dysfunction after fourth-ventricle epidermoid cyst resection. Cogn Behav Neurol 2018;31:207-13.
- 57 Kaba DI, Maati A, Dianka MB, Camara AM, Bocco AF, Chellaoui A, et al. The fourth ventricle epidermoid cyst: About two cases. J Med Res 2019;5:165-8.
- 58 Kumar S, Sharma S, Misra R, Kumar K. Epidermoid cyst of the fourth ventricle: A case report. Indian J Neurosurg 2019;8:191-2.
- 59 Hossini A, Lakhdar F, Gana R, Maaqili MR, Saïdi A, Jiddane M, et al. Epidermoid cyst of the cisterna magna and the fourth ventricle: Report of four cases. Neurochirurgie 2012;58:358-63.
- 60 El Saqui A, Aggouri M, Benzagmout M, Chakour K, Chaoui ME. Fourth ventricule epidermoid cyst: About a case. Pan Afr Med J 2017;26:239.
- 61 Fiume D, Gazzeri G, Spallone A, Santucci N. Epidermoid cysts of the fourth ventricle. Surg Neurol 1988;29:178-82.