
Subscribe to RSS
DOI: 10.4103/ajns.AJNS_317_19
Reversible thalamic dementia caused by venous hypertension of bilateral thalami resulting from multiple intracranial dural arteriovenous fistulas successfully obliterated by endovascular treatment using liquid embolic materials: A case report and literature review

We describe a patient with multiple cranial dural arteriovenous fistulas (DAVFs) presenting with thalamic dementia. A 52-year-old man experienced progressive dementia and behavioral change for 1 month. Cranial computed tomography scan and magnetic resonance imaging (MRI) showed bilateral thalamic edema with subsequent hemorrhagic transformation. Cerebral angiography demonstrated multiple cranial DAVFs at the straight sinus and posterior part of the superior sagittal sinus. The symptomatic fistula was the straight sinus DAVF, Cognard Type II a + b, supplied by meningeal branches of the left superior cerebellar artery, the left ascending pharyngeal artery originating from the left occipital artery, and multiple tiny branches of the left occipital artery with retrograde venous drainage into the straight sinus and vein of Galen. In addition, there was probable thrombosis at the middle part of the straight sinus associated with anatomical variation of the dural venous sinuses at the torcular herophili. The patient underwent successfully endovascular treatments in a two-staged embolization using liquid embolic materials. The patient has gradually recovered and could get back to the activities of daily living at home within 2 months. Follow-up MRI of the brain at 6 months revealed nearly complete resolution of the bilateral thalamic congestion. Cerebral angiography, obtained 1 year after endovascular treatment, confirmed complete obliteration of both DAVFs. We also reviewed the literature of thalamic dementia caused by intracranial DAVFs.
Key-words:
Endovascular treatment - multiple intracranial dural arteriovenous fistulas - tentorial dural arteriovenous fistula - thalamic dementiaIntroduction
Intracranial dural arteriovenous fistulas (DAVFs) are abnormal arteriovenous connections located within the dura matter, commonly near the venous sinuses.[[1]] Symptoms of the patients usually relate to location of the fistulas and venous drainage patterns.[[2]] Multiple intracranial DAVFs account for 7%–8.1% of all cranial DAVFs and are associated with a higher percentage of cortical venous drainage, yielding a high risk for hemorrhage and venous hypertension.[[3]],[[4]] In addition, venous hypertension occurs more often in the deep venous system. They usually run aggressive clinical course with rapidly progression of symptoms following initial onset. It is imperative to distinguish which fistula is the major implicated one, producing neurological symptoms.[[5]] We reported an extremely rare case of thalamic dementia caused by multiple intracranial DAVFs, including tentorial and superior sagittal sinus (SSS) fistulas, which the tentorial DAVF was the major implicated fistula.
Tentorial DAVFs are arteriovenous fistulas located in the tentorial dura matter and classified into six types, including galenic, straight sinus, torcular, tentorial sinus, superior petrosal sinus (SPS), and incisural DAVFs based on the location of fistula, dural base, associated sinus, and direction of venous drainage.[[6]] DAVFs of this location typically manifest with hemorrhage, caused by rupture of cortical veins or venous aneurysm, or progressive neurological deficits caused by venous hypertension.[[7]] Thalamic dementia, progressive cognitive dysfunction, caused by tentorial DAVFs results from venous hypertension in the bilateral thalami. This presenting symptom is uncommon and almost exclusively found in middle- to older-aged men.[[8]] We also reviewed the literature of patients with thalamic dementia caused by venous hypertension of bilateral thalami from intracranial DAVFs.
Case Report
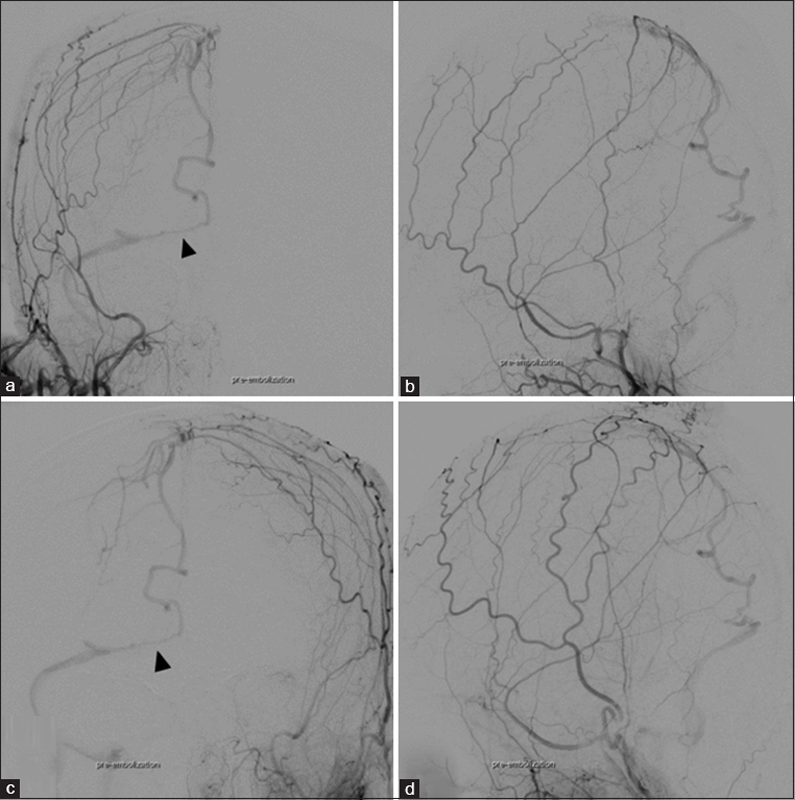
A 52-year-old nonsmoker man, engineer, with a medical history of hypertension, diabetes mellitus, and dyslipidemia was admitted to the local hospital because of progressive dementia and behavioral change for 1 month. There was no history of trauma, headache, or gait abnormality. Three weeks earlier, he was diagnosed with depression and prescribed antidepressant drugs from another local hospital. His spouse told that the patient ignored doing household activities and made mistakes during conversation, particularly naming objects. He also had frequent forgetfulness until disturbing his working performance, resulting in being taken a career break. Sometimes, he reported visual hallucination. Later, he was unable to use the key to unlock the keypad as ever. Finally, he required an assistant to perform activities of daily living. Cranial computed tomography (CT) scan showed diffuse symmetrical hypoattenuation of the bilateral thalami [[Figure 1]]a. Provisional diagnosis was bilateral thalamic infarctions from deep venous sinus thrombosis, and the patient was treated by anticoagulant therapy. One week later, the patient developed sudden onset of headache and obtained another CT scan, revealing acute small hematoma at the right medial occipital lobe [[Figure 1]]b. The patient was transferred to Prasat Neurological Institute for further investigation and proper treatment. Neurological examination revealed apathy, disorientation in time and place, and impairment of recent and recall memory without focal neurological deficits. The other physical findings were unremarkable. Serologic evaluations, including complete blood count, blood sugar, electrolytes, liver function, and kidney function, were all within normal limits. Thrombophilia screen (i.e., protein C, protein S, antithrombin III, anticardiolipin antibodies) was negative. Magnetic resonance imaging (MRI) of the brain showed hyperintense lesions of the bilateral thalami, right greater than left, on fluid-attenuated inversion recovery (FLAIR) and T2-weighted sequences with patchy enhancement on T1-weighted gadolinium-enhanced sequence [[Figure 2]]a, [[Figure 2]]b, [[Figure 2]]c. Three-dimensional (3D) time-of-flight (TOF) MR angiography (MRA) demonstrated the straight sinus and vein of Galen, probably representing arterialized deep venous structure [[Figure 2]]d. There was no restricted diffusion on apparent diffusion coefficient (ADC) map and diffusion-weighted imaging (DWI) of the bilateral thalami [[Figure 3]]a and [[Figure 3]]b. Susceptibility-weighted imaging disclosed numerous hypointense foci at bilateral thalami and basal ganglia regions, probably representing petechial hemorrhages, and abnormal hypersignal intensities of the vein of Galen and straight sinus, corresponding with arterialized blood flow of these venous structures [[Figure 3]]c and [[Figure 3]]d. The most likely diagnosis was bilateral thalamic venous congestion due to DAVF. Cerebral angiography demonstrated multiple cranial DAVFs at the straight sinus and posterior part of the SSS. The straight sinus DAVF, Cognard Type II a + b, supplied by meningeal branches of the left superior cerebellar artery, the left ascending pharyngeal artery originating from the left occipital artery, and multiple tiny branches of the left occipital artery with draining into the dilated straight sinus and vein of Galen. Subsequently, the drainage ran into bilateral basal veins of Rosenthal. On the right side, further drainage empties into the lateral mesencephalic vein, superior petrosal vein, SPS, and right transverse-sigmoid sinus. On the left side, further drainage empties into the tentorial sinus and left transverse-sigmoid sinus [[Figure 4]]. Another DAVF at the right-sided of posterior part of SSS, Cognard Type III, supplied by bilateral middle meningeal arteries with draining into the dilated right posteromedial parietal vein, right occipitobasal vein, lateral tentorial sinus, and right transverse-sigmoid sinus [[Figure 5]]. In addition, there was an anatomical variation of the dural venous sinuses at the torcular herophili. Corresponding with 3D maximum intensity projection (MIP) obtained from contrast-enhanced (CE) MR venography (MRV), the venous phase of the cerebral angiography illustrated the oblique occipital sinus communicated between the deviated SSS bifurcation cranially and the right distal sigmoid sinus/jugular bulb caudally. The straight sinus drained into the left transverse sinus located at the torcular herophili. The late venous phase of both internal carotid arteries revealed the venous drainage into the oblique occipital sinus without drainage into the straight sinus. Furthermore, the middle part of straight sinus was not visualized on 3D CE-MRV MIP images, probably representing partially thrombosis of the straight sinus [[Figure 6]]. The straight sinus DAVF was considered as a symptomatic fistula in our case. Then, transarterial embolization with precipitating hydrophobic injectable liquid (PHIL; MicroVention, Tustin, CA, USA) through the branch of the left occipital artery was successfully performed to complete obliteration of this fistula [[Figure 7]]a and [[Figure 7]]b. The patient has gradually recovered and could get back to the activities of daily living at home within 2 months. Follow-up cerebral angiography revealed complete occlusion of the straight sinus DAVF and persistence of another fistula at the SSS. Due to cortical venous drainage in SSS DAVF, transarterial embolization with ethylene-vinyl alcohol (EVOH) copolymer (Onyx; eV3, Medtronic Inc, Dublin, Ireland) through the posterior branch of the right middle meningeal artery was successfully performed [[Figure 7]]c and d]. Follow-up MRI of the brain at 6 months following endovascular treatments revealed nearly complete resolution of the bilateral thalamic infarctions without enhancing area [[Figure 8]]. Follow-up angiography obtained 1 year following endovascular treatments confirmed no recurrent of both DAVFs at the straight sinus and SSS [[Figure 9]]. The patient has remained clinically asymptomatic 2 years after endovascular treatment. In addition, he can still play golf every month.








Discussion
Cortical dementia caused by cranial DAVFs may result from widespread venous hypertension or congestion, leading to diffuse ischemia and impairment of parenchymal venous drainage, resulting in progressive dysfunction of the brain parenchyma or venous hypertensive encephalopathy. The pattern of MRI findings usually reveals diffuse FLAIR hyperintensity in the cerebral hemispheric white matter. In addition, the common finding on cerebral angiography is delayed venous emptying.[[9]] Similarly, thalamic dementia may cause by cranial DAVFs producing the venous reflux to the straight sinus, vein of Galen, and internal cerebral veins, causing in venous congestion of bilateral thalami.[[10]]
However, the bilateral thalamic hyperintensity on FLAIR or T2-weighted image may be found in other common conditions, including top of the basilar syndrome, occlusion of the artery of Percheron, deep cerebral venous system thrombosis, high-grade glioma, or intracranial DAVF.[[11]] Due to subacute onset of symptoms in our case, either deep cerebral venous thrombosis or DAVF was considered as the possible cause of thalamic dementia. Deep cerebral vein thrombosis, defined as thrombosis internal cerebral vein(s) and/or the vein of Galen, commonly presented with headache, nausea/vomiting, and/or change in mental status and occurs more frequently in women.[[12]] Unexplained rapidly progressive dementia should be evaluated with MRI, MRA, and likely subsequent cerebral angiography. Bilateral thalamic edema caused by DAVFs usually shows no restricted diffusion or normal DWI and ADC, as shown in our case. In addition, SWI and 3D TOF MRA demonstrated arterialized blood flow in the straight sinus and vein of Galen, supporting definite diagnosis of a DAVF. Cerebral angiography may be indicated when the diagnosis is still uncertain. In addition, to avoid unnecessary biopsy or misusing medical therapy, a diagnostic angiography should be performed due to its ability to definite a DAVF and for detailed anatomical evaluation.[[13]],[[14]]
We reviewed the literature of patients with thalamic dementia caused by venous hypertension of bilateral thalami from cranial DAVFs and found 28 cases, including our present case, with 30 fistulas due to bilateral lesions in two cases [[Table 1]].[[8]],[[10]],[[13]],[[14]],[[15]],[[16]],[[17]],[[18]],[[19]],[[20]],[[21]],[[22]],[[23]],[[24]],[[25]],[[26]],[[27]],[[28]],[[29]],[[30]],[[31]],[[32]] The collected data in this review included demographic data (i.e., gender and age of patient), location and arterial supply of the fistulas, symptoms and signs of the patients, angiographic occlusion of the straight sinus, presence of intracerebral hemorrhage, treatment of the fistulas, and neurological outcome after treatment. From the literature review, there were 25 men (89.3%) and 3 women (10.7%) with median age of 59.5 years, ranging from 43 to 77 years. All patients except one with thalamic dementia had fistulas located in the posterior fossa. Most fistulas (80%) were located at tentorium, including straight sinus, torcula, SPS, and unspecified location. Other location of the fistulas (20%) included SSS, transverse sinus, and transverse-sigmoid sinus. The fistulas supplied by middle meningeal artery, occipital artery, posterior meningeal branch of vertebral artery, ascending pharyngeal artery, superficial temporal artery, meningohypophyseal trunk, and/or tentorial branch of superior cerebellar artery. The patients presented with progressive dementia, disorientation, gait ataxia, hypersomnolence, Parkinsonism, abnormal speech, neurological deficits, and/or deterioration of conscious. Intracerebral hemorrhage, including petechial hemorrhage and intracerebral hematoma, occurred in eight patients (28.6%). Angiographic occlusion of the straight sinus was detected in 21 patients (75%). Eighteen patients (64.3%) were treated with endovascular treatment alone, three (10.7%) with surgery alone, six (21.4%) with combination of endovascular and surgical treatments, and one (3.6%) left untreated. Twenty-one patients (75%) had good recovery or improvement of neurological symptoms.


Hemorrhagic transformation, including intracerebral hematoma, microhemorrhage, or petechial hemorrhage, within the thalami, basal ganglia, or deep brain structures, may represent that the lesion was left untreated for a long time or from chronic venous congestion.[[14]],[[19]],[[25]],[[27]],[[29]] In our case, small hematoma at the right medial occipital lobe may result from venous congestion of the internal occipital vein receiving drainage from the basal vein of Rosenthal. Further, there were petechial hemorrhages at bilateral thalami and basal ganglia.
The presence of the occluded or thrombosed straight sinus may cause the formation of the tentorial DAVF, indicative of this acquired lesion.[[25]],[[27]],[[29]] Most patients harboring tentorial DAVFs including our case had angiographic occlusion of the straight sinus.[[8]],[[14]],[[15]],[[16]],[[18]],[[21]],[[22]],[[24]],[[25]],[[27]],[[29]],[[30]],[[32]] Interestingly, Iwasawa et al.[[28]] reported a patient with DAVF at transverse-sigmoid sinus without thrombosed straight sinus and speculated that an anatomical variation, i.e., noncommunication between the right and left transverse sinuses, may play a major role in producing thalamic dementia by increasing drainage into the deep venous structure. Tanaka et al.[[17]] reported a patient with tentorial DAVF associated with occlusion of bilateral transverse sinuses compromising hemodynamics into bilateral thalami. In addition, DAVFs at torcula, transverse, or transverse-sigmoid sinus with occlusion or thrombosis of transverse, sigmoid, and/or sagittal sinuses may cause retrograde flow into the straight sinus and its branches, leading to venous hypertension and secondary ischemia.[[20]],[[23]],[[26]] However, it is uncertain that an anatomical variation of the dural venous sinuses at the torcular herophili in our case may affect the hemodynamic through the straight sinus, inducing thrombosis of the middle part of the straight sinus.
Multiple fistulas can be described as fistulas that are distinct anatomically in relation to arterial inflow, location of the fistula, and venous drainage.[[3]] Multiple DAVFs may be divided into two types, including synchronous and metachronous. Synchronous type refers to multiple fistulas that occur simultaneously, whereas independent fistulas in metachronous type develop over time. The exact pathogenesis remains unclear. The potential causes include venous sinus thrombosis, angiogenic factor, disturbed hemodynamics, and congenital factors.[[5]] All fistulas of multiple intracranial DAVFs may not contribute to venous hypertension. The priority of treatment is target fistulas with cortical venous reflux. Multiple stages of treatment may be required.[[13]] Indication for treatment of second incidentally identified DAVF is the fistula having high-risk factor for hemorrhage, i.e., cortical venous drainage.[[3]] Our case was synchronously diagnosed as multiple cranial DAVFs which the tentorial DAVF, i.e., the straight sinus DAVF, was the symptomatic fistula producing thalamic dysfunction caused by increased venous back pressure bypassing the occluded straight sinus to the proximal straight sinus with retrograde flow through the vein of Galen and internal cerebral veins.
DAVF-induced thalamic dementia should be treated promptly due to the possibility of rapid neurological decline in the days following initial diagnosis of DAVF.[[8]] Tentorial DAVFs can be treated by surgery, endovascular treatment, or both depending on institution's preference.[[6]],[[7]],[[8]],[[22]] Lawton et al.[[6]] preferred to treat all types of tentorial DAVFs by simple microsurgical interruption of the draining vein. Due to multiplicity of small feeding vessels, cortical venous drainage, and deep location, tentorial DAVFs are difficult to obliterate. Thus, Lewis et al.[[7]] have developed a treatment protocol using transarterial embolization with adhesive glue (N-butyl-2-cyanoacrylate) combined with radiosurgery or direct microsurgical obliteration from arterial side. Our literature review found that endovascular treatment with one or multiple stages was the first choice of treatment in patients harboring tentorial DAVFs causing thalamic dementia.[[8]],[[10]],[[13]],[[17]],[[19]],[[25]],[[28]],[[29]],[[30]],[[32]] Surgical option was considered in the fistula with unsuccessful endovascular attempt.[[8]],[[15]],[[27]]
Until currently, the new generation nonadhesive liquid embolic agents (EVOH copolymer), including Onyx and PHIL, have revolutionized the treatment of intracranial DAVFs, changing the therapeutic trend toward a predominantly endovascular treatment alone.[[33]],[[34]],[[35]] Both tantalum-based Onyx and iodine-based PHIL were available in our institute and successfully used for complete obliteration of multiple cranial DAVFs in the present case.
Cerebral edema following occlusion of the cerebral veins can be divided into two different types, i.e., cytotoxic edema and vasogenic edema. Cytotoxic edema is caused by ischemia, damaging the energy-dependent cellular membrane pumps, resulting in intracellular swelling. Vasogenic edema, resulting from disruption in the blood–brain barrier and leakage of blood plasma into interstitial space, can be reversible after successful treatment of underlying condition.[[36]] The patients with hemorrhagic venous infarction caused by deep cerebral vein thrombosis tend to end up with death or long-term severe sequelae.[[12]] In contrast, most patients including our case suffering from hemorrhagic venous infarction caused by DAVFs usually recover dramatically following prompt treatment. Reversible thalamic dementia and MR appearance may reflect thalamic edema from venous hypertension rather than infarction.[[9]],[[18]] However, patients may end up with poor neurological outcome or die, if left untreated or delayed treatment.[[16]],[[26]]
Conclusion
We reported an extremely rare case of thalamic dementia secondary to multiple intracranial DAVFs, including the straight sinus and SSS. The straight sinus DAVF was the most likely symptomatic fistula. Bilateral thalamic venous edema with subsequent hemorrhagic transformation resulted from DAVF draining retrogradely into the proximal straight sinus, vein of Galen, and internal cerebral veins. The cause of this condition may relate to thrombosed straight sinus. Neurologically and radiologically, the hemorrhagic venous infarction has nearly completely resolved following obliteration of the fistula by two-staged endovascular treatment using PHIL and Onyx. Thalamic dementia, aggressive neurologic dysfunction, caused by DAVFs may be reversible following timely treatment. Prompt diagnosis and treatment could be the key to achieve good outcome.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Lasjaunias P, Berenstein A, Ter Brugge KG. Surgical Neuroangiography. Vol. 2.2. New York: Springer-Verlag; 2004.
- 2 Lasjaunias P, Chiu M, ter Brugge K, Tolia A, Hurth M, Bernstein M. Neurological manifestations of intracranial dural arteriovenous malformations. J Neurosurg 1986;64:724-30.
- 3 Barnwell SL, Halbach VV, Dowd CF, Higashida RT, Hieshima GB, Wilson CB. Multiple dural arteriovenous fistulas of the cranium and spine. AJNR Am J Neuroradiol 1991;12:441-5.
- 4 van Dijk JM, TerBrugge KG, Willinsky RA, Wallace MC. Multiplicity of dural arteriovenous fistulas. J Neurosurg 2002;96:76-8.
- 5 Guo Y, Yu J, Zhao Y, Yu J. Progress in research on intracranial multiple dural arteriovenous fistulas. Biomed Rep 2018;8:17-25.
- 6 Lawton MT, Sanchez-Mejia RO, Pham D, Tan J, Halbach VV. Tentorial dural arteriovenous fistulae: Operative strategies and microsurgical results for six types. Neurosurgery 2008;62:110-24.
- 7 Lewis AI, Tomsick TA, Tew JM Jr. Management of tentorial dural arteriovenous malformations: Transarterial embolization combined with stereotactic radiation or surgery. J Neurosurg 1994;81:851-9.
- 8 Holekamp TF, Mollman ME, Murphy RK, Kolar GR, Kramer NM, Derdeyn CP, et al. Dural arteriovenous fistula-induced thalamic dementia: Report of 4 cases. J Neurosurg 2016;124:1752-65.
- 9 Hurst RW, Bagley LJ, Galetta S, Glosser G, Lieberman AP, Trojanowski J, et al. Dementia resulting from dural arteriovenous fistulas: The pathologic findings of venous hypertensive encephalopathy. AJNR Am J Neuroradiol 1998;19:1267-73.
- 10 Gonçalves MB, Maia O Jr., Correa JL, Siqueira SB, Christoph Dde H, Landeiro JA. Dural arteriovenous fistula presenting as thalamic dementia. Arq Neuropsiquiatr 2008;66:264-7.
- 11 de Medeiros FC, de Albuquerque LA. Differential diagnosis in bilateral thalamic infarct: Clinical and radiological aspects. Acta Neurol Belg 2015;115:367-9.
- 12 Crawford SC, Digre KB, Palmer CA, Bell DA, Osborn AG. Thrombosis of the deep venous drainage of the brain in adults. Analysis of seven cases with review of the literature. Arch Neurol 1995;52:1101-8.
- 13 Sugrue PA, Hurley MC, Bendok BR, Surdell DL, Gottardi-Littell N, Futterer SF, et al. High-grade dural arteriovenous fistula simulating a bilateral thalamic neoplasm. Clin Neurol Neurosurg 2009;111:629-32.
- 14 Nakada T, Kwee IL, Ellis WG, St John JN. Subacute diencephalic necrosis and dural arteriovenous malformation. Neurosurgery 1985;17:653-6.
- 15 Ito M, Sonokawa T, Mishina H, Sato K. Reversible dural arteriovenous malformation-induced venous ischemia as a cause of dementia: Treatment by surgical occlusion of draining dural sinus: Case report. Neurosurgery 1995;37:1187-91.
- 16 Iwama T, Hashimoto N, Takagi Y, Tanaka M, Yamamoto S, Nishi S, et al. Hemodynamic and metabolic disturbances in patients with intracranial dural arteriovenous fistulas: Positron emission tomography evaluation before and after treatment. J Neurosurg 1997;86:806-11.
- 17 Tanaka K, Morooka Y, Nakagawa Y, Shimizu S. Dural arteriovenous malformation manifesting as dementia due to ischemia in bilateral thalami. A case report. Surg Neurol 1999;51:489-93.
- 18 Greenough GP, Mamourian A, Harbaugh RE. Venous hypertension associated with a posterior fossa dural arteriovenous fistula: Another cause of bithalamic lesions on MR images. AJNR Am J Neuroradiol 1999;20:145-7.
- 19 Tamamoto F, Nakanishi A, Takanashi T, Ishizaki H, Nagasawa H, Maehara T, et al. Unexpected accumulation of thallium-201 in bilateral thalamic venous infarction induced by arteriovenous fistula in the posterior fossa: Report of a case. Ann Nucl Med 2003;17:239-43.
- 20 Tominaga T, Shamoto H, Shimizu H, Watanabe M, Yoshimoto T. Selective loss of Purkinje cells in transverse and sigmoid dural arteriovenous fistulas. Report of two cases. J Neurosurg 2003;98:617-20.
- 21 Matsumura A, Oda M, Hozuki T, Imai T, Shimohama S. Dural arteriovenous fistula in a case of dementia with bithalamic MR lesions. Neurology 2008;71:1553.
- 22 Racine CA, Lawton MT, Hetts SW, Josephson SA. Neuropyschological profile of reversible cognitive impairment in a patient with a dural arteriovenous fistula. Neurocase 2008;14:231-8.
- 23 Wilson M, Enevoldson P, Menezes B. Intracranial dural arterio-venous fistula. Pract Neurol 2008;8:362-9.
- 24 Yamamoto T, Watanabe M, Miura A, Hirahara T, Hirano T, Uchino M. A case of dural arteriovenous fistula associated with bilateral thalamic lesions. Rinsho Shinkeigaku 2010;50:718-24.
- 25 Santillan A, Safdieh JE, Gobin YP, Patsalides A. Neurological picture. Bilateral thalamic venous hypertension caused by a tentorial dural arteriovenous fistula: Endovascular treatment. J Neurol Neurosurg Psychiatry 2011;82:749-50.
- 26 Geraldes R, Albuquerque L, Ferro JM, Sousa R, Sequeira P, Campos J. Rapidly progressive cognitive impairment, ataxia, and myoclonus: An unusual presentation of a dural arteriovenous fistula. J Stroke Cerebrovasc Dis 2012;21:619.e3-5.
- 27 Morparia N, Miller G, Rabinstein A, Lanzino G, Kumar N. Cognitive decline and hypersomnolence: Thalamic manifestations of a tentorial dural arteriovenous fistula (dAVF). Neurocrit Care 2012;17:429-33.
- 28 Iwasawa E, Ishibashi S, Miki K, Yoshino Y, Nemoto S, Mizusawa H. Teaching NeuroImages: Reversible cognitive impairment with bithalamic lesions caused by a dural arteriovenous fistula. Neurology 2013;81:e38-9.
- 29 Borja MJ, Schaefer PW, Boulter DJ. Case of the season: Dural arteriovenous fistula mimicking a bithalamic neoplasm or viral encephalitis. Semin Roentgenol 2014;49:4-9.
- 30 Honig A, Eliahou R, Eichel R, Shemesh AA, Ben-Hur T, Auriel E. Acute bithalamic infarct manifesting as sleep-like coma: A diagnostic challenge. J Clin Neurosci 2016;34:81-5.
- 31 Hwang H, La YK, Baek MS, Baik K, Suh SH, Kim WJ. Dural arteriovenous fistula manifested as rapid progressive dementia successfully treated by endovascular embolization only. Neurointervention 2017;12:50-3.
- 32 Colorado RA, Matiello M, Yang HS, Rabinov JD, Patel A, Hirsch JA, et al. Progressive neurological decline with deep bilateral imaging changes: A protean presentation of dural arteriovenous fistulae. Interv Neurol 2018;7:256-64.
- 33 Cannizzaro D, Brinjikji W, Rammos S, Murad MH, Lanzino G. Changing clinical and therapeutic trends in tentorial dural arteriovenous fistulas: A systematic review. AJNR Am J Neuroradiol 2015;36:1905-11.
- 34 Cognard C, Januel AC, Silva NA Jr, Tall P. Endovascular treatment of intracranial dural arteriovenous fistulas with cortical venous drainage: New management using Onyx. AJNR Am J Neuroradiol 2008;29:235-41.
- 35 Lamin S, Chew HS, Chavda S, Thomas A, Piano M, Quilici L, et al. Embolization of intracranial dural arteriovenous fistulas using PHIL liquid embolic agent in 26 patients: A multicenter study. AJNR Am J Neuroradiol 2017;38:127-31.
- 36 Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med 2005;352:1791-8.
Address for correspondence
Publication History
Received: 27 October 2019
Accepted: 11 December 2019
Article published online:
16 August 2022
© 2020. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Lasjaunias P, Berenstein A, Ter Brugge KG. Surgical Neuroangiography. Vol. 2.2. New York: Springer-Verlag; 2004.
- 2 Lasjaunias P, Chiu M, ter Brugge K, Tolia A, Hurth M, Bernstein M. Neurological manifestations of intracranial dural arteriovenous malformations. J Neurosurg 1986;64:724-30.
- 3 Barnwell SL, Halbach VV, Dowd CF, Higashida RT, Hieshima GB, Wilson CB. Multiple dural arteriovenous fistulas of the cranium and spine. AJNR Am J Neuroradiol 1991;12:441-5.
- 4 van Dijk JM, TerBrugge KG, Willinsky RA, Wallace MC. Multiplicity of dural arteriovenous fistulas. J Neurosurg 2002;96:76-8.
- 5 Guo Y, Yu J, Zhao Y, Yu J. Progress in research on intracranial multiple dural arteriovenous fistulas. Biomed Rep 2018;8:17-25.
- 6 Lawton MT, Sanchez-Mejia RO, Pham D, Tan J, Halbach VV. Tentorial dural arteriovenous fistulae: Operative strategies and microsurgical results for six types. Neurosurgery 2008;62:110-24.
- 7 Lewis AI, Tomsick TA, Tew JM Jr. Management of tentorial dural arteriovenous malformations: Transarterial embolization combined with stereotactic radiation or surgery. J Neurosurg 1994;81:851-9.
- 8 Holekamp TF, Mollman ME, Murphy RK, Kolar GR, Kramer NM, Derdeyn CP, et al. Dural arteriovenous fistula-induced thalamic dementia: Report of 4 cases. J Neurosurg 2016;124:1752-65.
- 9 Hurst RW, Bagley LJ, Galetta S, Glosser G, Lieberman AP, Trojanowski J, et al. Dementia resulting from dural arteriovenous fistulas: The pathologic findings of venous hypertensive encephalopathy. AJNR Am J Neuroradiol 1998;19:1267-73.
- 10 Gonçalves MB, Maia O Jr., Correa JL, Siqueira SB, Christoph Dde H, Landeiro JA. Dural arteriovenous fistula presenting as thalamic dementia. Arq Neuropsiquiatr 2008;66:264-7.
- 11 de Medeiros FC, de Albuquerque LA. Differential diagnosis in bilateral thalamic infarct: Clinical and radiological aspects. Acta Neurol Belg 2015;115:367-9.
- 12 Crawford SC, Digre KB, Palmer CA, Bell DA, Osborn AG. Thrombosis of the deep venous drainage of the brain in adults. Analysis of seven cases with review of the literature. Arch Neurol 1995;52:1101-8.
- 13 Sugrue PA, Hurley MC, Bendok BR, Surdell DL, Gottardi-Littell N, Futterer SF, et al. High-grade dural arteriovenous fistula simulating a bilateral thalamic neoplasm. Clin Neurol Neurosurg 2009;111:629-32.
- 14 Nakada T, Kwee IL, Ellis WG, St John JN. Subacute diencephalic necrosis and dural arteriovenous malformation. Neurosurgery 1985;17:653-6.
- 15 Ito M, Sonokawa T, Mishina H, Sato K. Reversible dural arteriovenous malformation-induced venous ischemia as a cause of dementia: Treatment by surgical occlusion of draining dural sinus: Case report. Neurosurgery 1995;37:1187-91.
- 16 Iwama T, Hashimoto N, Takagi Y, Tanaka M, Yamamoto S, Nishi S, et al. Hemodynamic and metabolic disturbances in patients with intracranial dural arteriovenous fistulas: Positron emission tomography evaluation before and after treatment. J Neurosurg 1997;86:806-11.
- 17 Tanaka K, Morooka Y, Nakagawa Y, Shimizu S. Dural arteriovenous malformation manifesting as dementia due to ischemia in bilateral thalami. A case report. Surg Neurol 1999;51:489-93.
- 18 Greenough GP, Mamourian A, Harbaugh RE. Venous hypertension associated with a posterior fossa dural arteriovenous fistula: Another cause of bithalamic lesions on MR images. AJNR Am J Neuroradiol 1999;20:145-7.
- 19 Tamamoto F, Nakanishi A, Takanashi T, Ishizaki H, Nagasawa H, Maehara T, et al. Unexpected accumulation of thallium-201 in bilateral thalamic venous infarction induced by arteriovenous fistula in the posterior fossa: Report of a case. Ann Nucl Med 2003;17:239-43.
- 20 Tominaga T, Shamoto H, Shimizu H, Watanabe M, Yoshimoto T. Selective loss of Purkinje cells in transverse and sigmoid dural arteriovenous fistulas. Report of two cases. J Neurosurg 2003;98:617-20.
- 21 Matsumura A, Oda M, Hozuki T, Imai T, Shimohama S. Dural arteriovenous fistula in a case of dementia with bithalamic MR lesions. Neurology 2008;71:1553.
- 22 Racine CA, Lawton MT, Hetts SW, Josephson SA. Neuropyschological profile of reversible cognitive impairment in a patient with a dural arteriovenous fistula. Neurocase 2008;14:231-8.
- 23 Wilson M, Enevoldson P, Menezes B. Intracranial dural arterio-venous fistula. Pract Neurol 2008;8:362-9.
- 24 Yamamoto T, Watanabe M, Miura A, Hirahara T, Hirano T, Uchino M. A case of dural arteriovenous fistula associated with bilateral thalamic lesions. Rinsho Shinkeigaku 2010;50:718-24.
- 25 Santillan A, Safdieh JE, Gobin YP, Patsalides A. Neurological picture. Bilateral thalamic venous hypertension caused by a tentorial dural arteriovenous fistula: Endovascular treatment. J Neurol Neurosurg Psychiatry 2011;82:749-50.
- 26 Geraldes R, Albuquerque L, Ferro JM, Sousa R, Sequeira P, Campos J. Rapidly progressive cognitive impairment, ataxia, and myoclonus: An unusual presentation of a dural arteriovenous fistula. J Stroke Cerebrovasc Dis 2012;21:619.e3-5.
- 27 Morparia N, Miller G, Rabinstein A, Lanzino G, Kumar N. Cognitive decline and hypersomnolence: Thalamic manifestations of a tentorial dural arteriovenous fistula (dAVF). Neurocrit Care 2012;17:429-33.
- 28 Iwasawa E, Ishibashi S, Miki K, Yoshino Y, Nemoto S, Mizusawa H. Teaching NeuroImages: Reversible cognitive impairment with bithalamic lesions caused by a dural arteriovenous fistula. Neurology 2013;81:e38-9.
- 29 Borja MJ, Schaefer PW, Boulter DJ. Case of the season: Dural arteriovenous fistula mimicking a bithalamic neoplasm or viral encephalitis. Semin Roentgenol 2014;49:4-9.
- 30 Honig A, Eliahou R, Eichel R, Shemesh AA, Ben-Hur T, Auriel E. Acute bithalamic infarct manifesting as sleep-like coma: A diagnostic challenge. J Clin Neurosci 2016;34:81-5.
- 31 Hwang H, La YK, Baek MS, Baik K, Suh SH, Kim WJ. Dural arteriovenous fistula manifested as rapid progressive dementia successfully treated by endovascular embolization only. Neurointervention 2017;12:50-3.
- 32 Colorado RA, Matiello M, Yang HS, Rabinov JD, Patel A, Hirsch JA, et al. Progressive neurological decline with deep bilateral imaging changes: A protean presentation of dural arteriovenous fistulae. Interv Neurol 2018;7:256-64.
- 33 Cannizzaro D, Brinjikji W, Rammos S, Murad MH, Lanzino G. Changing clinical and therapeutic trends in tentorial dural arteriovenous fistulas: A systematic review. AJNR Am J Neuroradiol 2015;36:1905-11.
- 34 Cognard C, Januel AC, Silva NA Jr, Tall P. Endovascular treatment of intracranial dural arteriovenous fistulas with cortical venous drainage: New management using Onyx. AJNR Am J Neuroradiol 2008;29:235-41.
- 35 Lamin S, Chew HS, Chavda S, Thomas A, Piano M, Quilici L, et al. Embolization of intracranial dural arteriovenous fistulas using PHIL liquid embolic agent in 26 patients: A multicenter study. AJNR Am J Neuroradiol 2017;38:127-31.
- 36 Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med 2005;352:1791-8.