
Subscribe to RSS
DOI: 10.4103/ajns.AJNS_312_19
Morphometry of the C2 pedicle and lamina in thai patients

Background: Traumatic upper cervical spine leads to instability and neurological deficit. At present, C2 (axis) pedicle or lamina screws for fixation are popular because further external immobilization is not needed. However, these techniques demand experience inserting the screws and carry the risk of vertebral artery or spinal cord injury. In some patients, the C2 screws cannot be inserted because of limited C2 size. Objective: To determine the width, length, height, and angle in the C2 pedicle and lamina in the Thai population. Materials and Methods: Patient data were collected from the Picture Archiving and Communication System at the Faculty of Medicine, Prince of Songkla University from January 2016 to December 2017. The C2 parameters, i.e., width, length, height, and angle of the pedicle and lamina were recorded. Results: The CT C-spine scans of 270 patients were enrolled. The mean Thai C2 pedicle dimensions were width 5.51 mm, length 23.78 mm, angle 39.04°, and height 8.64 mm. The mean C2 lamina dimensions were width 5.88 mm, length 32.17 mm, angle 49.46°, and height 12.27 mm. Twenty-four patients from the 270 patients (8.8%) had a pedicle width <3.5 mm but all patients had a lamina width ≥3.5 mm. Conclusion: In the Thai samples, 8.8% had a C2 pedicle width <3.5 mm which would not allow insertion of screws; however, they could be replaced with lamina screws since the lamina width was ≥3.5 mm. In this study, all of the patients who could not be inserted pedicle can be replaced with lamina screws inserted.
Introduction
Traumatic upper cervical spine leads to instability in weightbearing and movement. The results of upper cervical spine injury are neck pain, neurological deficit, vertebral deformity, and movement disorder. Patients with these injuries cannot live normally. Multiple surgical management of upper cervical spine injury was developed for a higher chance of successful fusion and higher fixation rate.
C1–C2 wiring with a bone graft entails a wire between the C1 and C2 cervical spine and the addition of bone at the posterior part of the C1–C2 for fusion. This method has a failure rate of about 30%.[[1]]
In C1–C2 transarticular[[2]],[[3]] screw fixation, the screws are inserted from the posterior part of the C2 to the C1 for fixation. A meta-analysis for this technique had a higher rate of fusion in 94.6% but a highly experienced surgeon is needed due to the risk of vertebral artery injury in 3.1%.[[4]]
C1 lateral mass–C2 pedicle screws,[[5]] is a technique that starts with screws inserted from the posterior C2 to the pedicle and vertebral body. The next step is to insert the screws into the lateral mass of C1 and apply rods for fixation between C1 and C2. A meta-analysis revealed a 97.5% rate of fusion that required less surgical skill than the C1–C2 transarticular screw technique. Vertebral injury in this technique was <2% which was lower than C1–C2 transarticular screw fixation.[[6]]
The newer technique is C1 lateral mass–C2 lamina screw fixation. In this method the screw is applied at the contralateral posterior spinolaminar junction to the ipsilateral lamina and C1 lateral mass screws with rods. The C2 lamina screws do not present a risk for vertebral artery injury but they remain a risk for spinal cord injury. This alternative method can be used when the C1–C2 transarticular screws or pedicle screws cannot be used due to the inappropriate size or high-riding vertebral artery that occurs in 16.5%.[[7]] Parker et al.[[8]] found that intraoperative breach occurred more frequently with C2 pedicle screws than C2 lamina screws. Even though the 1-year durability of C2 laminar screws might be inferior to C2 pedicle screws for subaxial fusions, they are equally effective for axial cervical fusions. From the literature review, lack of evidence determine intraoperative breach and durability in the C1 lateralmass-C2 lamina screw fixation technique.
Before C2 pedicle or lamina screw fixation, the surgeon needs to evaluate the C2 morphology, i.e., width, length, and angle, especially the width which is the most important limitation for screw fixation because around the screws are important structures near the pedicle (medially the spinal cord and laterally the vertebral artery) and lamina (medially the spinal cord). In Thailand, the diameter of the smallest screw is 3.5 mm. Therefore, the screws cannot be inserted if the width of the pedicle or lamina is smaller than 3.5 mm.
In Thai patients, knowledge on the morphology of the C2 pedicle and lamina is limited. A previous study in 54 Thai patients reported the morphology of the C2 pedicle but there is no study on the C2 lamina.[[9]] The purpose of this study was to assess the size and angle of the C2 pedicle and lamina morphology. The data are vital for the planning of screw fixation to decrease the risk of injury to the vertebral artery and spinal cord. Furthermore, this information can be used to develop medical instruments in the future.
Materials and Methods
The study was performed in patients over 15 years old who underwent a computed tomography (CT) scan of the cervical spine. Data were collected at the Faculty of Medicine, Prince of Songkla University using the Picture Archiving and Communication System (PACS) by searching the words “CT_C-spine” from January 1, 2016, to December 31, 2017. A cervical spine CT scan was performed in all patients using a Toshiba Aquilion Prime Model TSX-303A. The cervical spine CT scan image cuts were at a maximum of 1 mm intervals in the axial plane and at a maximum of 3 mm intervals in the sagittal plane. The information collected included demographic data, i.e., gender, age, weight, height, and the parameters from the cervical spine CT images. Patients with congenital anomalies or injuries to the C2 spine or artifacts that affected the evaluation of the cortex border of the pedicle and lamina were excluded.
Measurements
Measurements of the C2 spine parameters, including width, height, length, and angle of the pedicle and lamina, were performed using the PACS program (Synapse Workstation FUJIFILM Medical Systems Stamford Connecticut USA, Inc., version 4.3.221). The measurements were recorded as millimeters and degrees by a single author. The measurements were repeated two times.
Pedicle parameters
Axial plane
Width – The axial and sagittal planes were opened at the same time to find the mid-portion of the pedicle. The measurements were performed at the narrowest portion between the outer cortex of the medial and lateral pedicle at both sides [[Figure 1]]a.

Length of screws – The length was determined from the anterior outer vertebral body cortex, pedicle to the posterior outer cortex of the facet that was perpendicular to the mid-portion of the pedicle width. The length must not exceed two hemivertebrae body line [[Figure 1]]b.
Angle – The angle was measured from the length line and the two hemivertebrae body line [[Figure 1]]c.
Sagittal plane
Height – The height was measured from the superior to the inferior outer cortex perpendicular to the pedicle isthmus [[Figure 1]]d.
Lamina parameters
Axial plane
Width – The axial and sagittal planes were opened at the same time to find the mid-portion of the lamina. The measurement was determined at the narrowest portion between the outer cortex of the medial and lateral lamina at both sides [[Figure 1]]e.
Length of screws – The length was determined from the posterior outer cortex of the contralateral spinolaminar junction to the anterior outer cortex of the facet joint that was perpendicular to the mid-portion of the lamina width [[Figure 1]]f.
Angle – The angle was measured from the length line and the two hemivertebrae body line [[Figure 1]]g.
Sagittal plane
Height – The height was measured from the superior to the inferior outer cortex at the midline of the spinous process [[Figure 1]]h.
Results
From the 847 patients who consecutively had a CT C-spine exam at Songklanagarind Hospital from 2016 to 2017, 349 patients had a 1 mm axial plane CT C-spine. Finally, 270 patients were enrolled into the study after applying the inclusion and exclusion criteria [[Figure 2]].

The 270 patients included 188 (69.6%) males and 82 (30.4%) females. The median age of all patients was 45 years of age. The body mass index data revealed 107 (39.6%) patients were normal weight (<23 kg/m2), 122 (45.1%) were overweight (≥23 kg/m2), and 41 patients had missing data [[Table 1]].

The C2 pedicle width ranged from 1.46 to 8.72 mm with a mean ± standard deviation (SD) of 5.51 ± 1.42 mm, the C2 pedicle length ranged from 15.87 to 31.93 mm with a mean ± SD of 23.78 ± 3.10 mm, the C2 pedicle angle from midline ranged from 13.0° to 57.0° with a mean ± SD of 39.04° ± 7.31°, and the C2 pedicle height ranged from 4.96 to 12.34 mm with a mean ± SD of 8.65 ± 1.04 mm [[Table 2]].

The C2 lamina width ranged from 2.24 to 0.13 mm with a mean ± SD of 5.88 ± 1.30 mm, the C2 lamina length ranged from 22.39 to 43.77 mm with a mean ± SD of 32.17 ± 3.95 mm, the C2 lamina angle from the midline ranged from 33.0° to 63.5° with a mean ± SD of 49.46° ± 5.36°, and the C2 lamina height ranged from 7.19 to 59.88 mm with a mean ± SD of 12.27 ± 3.33 mm [[Table 3]].

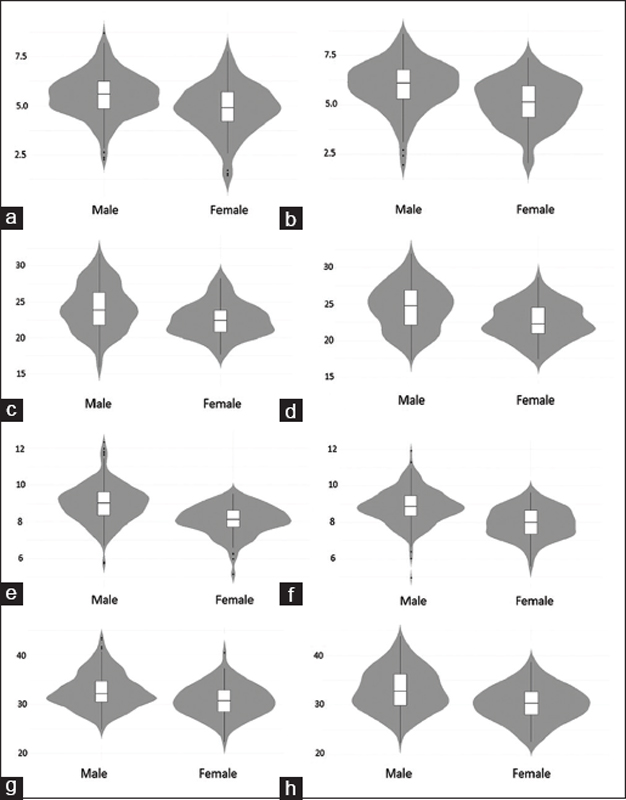
A subgroup analysis in gender revealed mean ± SD values of the C2 pedicle width of 5.74 ± 1.19 mm in males and 4.97 ± 1.20 mm in females, C2 pedicle length of 24.33 ± 3.21 mm in males and 22.53 ± 2.39 mm in females, C2 pedicle height of 8.92 ± 1.01 mm in males and 8.03 ± 0.82 mm in females, and C2 lamina length of 32.92 ± 3.98 mm in males and 30.52 ± 3.37 mm in females. The mean pedicle width, length, height, and lamina length were greater in males than in females. The differences were statistically significant (t-test, P < 0.05) [[Figure 3]]. A subgroup analysis in age revealed mean differences that were significant (P < 0.05). The mean ± SD C2 pedicle left length in patients ≥45 years of age was 24.43 ± 3.17 mm which was longer than in patients <45 years of age which was 23.47 ± 2.92 mm. The mean ± SD C2 lamina left length in patients ≥45 years of age was 31.60 ± 4.31 mm which was shorter than in patients <45 years of age which was 32.79 ± 4.12 mm. A subgroup analysis in body mass index indicated no association in the pedicle and lamina sizes.
Twenty-four patients (8.8%) had a pedicle width <3.5 mm (bilateral four patients and unilateral 20 patients) that would not be safe for placement of pedicle screws. However, they could be replaced with laminar screws since the lamina width was ≥3.5 mm [[Figure 4]].

Discussion
Two methods are used to measure the sizes of the pedicle and lamina. The first uses measurements from a CT scan and the second uses measurements directly from a cadaver. From 33 studies, no statistical differences were observed in measuring the cervical pedicle by either radiography or directly.[[10]]
In Thai patients, the present study found that the mean values for the C2 pedicle were width 5.51 mm, length screw 23.78 mm, height 8.65 mm, and angulation medially 39.04° which were similar to a previous study by Bunmaprasert et al.[[9]] They measured the C2 pedicle using CT scans in 53 Thai patients. The results revealed that the mean values were pedicle width 5.47 mm, height 7.54 mm, and angulation medially 38.95°. In Asian people, Yusof et al.[[11]] used CT scans in 80 Malay patients to measure the C2 pedicle. In 40 male patients and in 40 female patients the overall mean pedicle width was 4.57 mm. Liu J et al.[[10]] reported the C2 pedicle parameters using CT scanners of European and USA manufacturers from 3 studies and reported the means of width, length, and angle as 7.04 mm, 28.12 mm, and 38.66° [[Table 4]], respectively. Although a systematic review of C1‒7 by Liu J et al.[[10]] reported a comparison of races, statistically significant differences were found between the Asian and European/USA populations only in the pedicle axis length at C3 and C4 but the study included only 40 patients in the C2 pedicle group.

Comparisons in gender of the pedicle width, length, and height in males tended to be larger than females in both the Asian[[9]],[[11]] and European/USA populations.[[10]] The angles for the inserted pedicle screws in all studies were similar (38°‒ 39° medially).[[9]],[[10]]
To date, morphology of the C2 lamina has not been reported in Thai people. This is the first study on lamina morphology to reveal the mean values of laminar width 5.88 mm, screw length 32.18 mm, height 12.27 mm, and angulation laterally 49.46°. Kim et al.[[12]] measured the C2 lamina in 102 Korean patients from CT scans and the mean ± SD results were width 5.66 ± 0.22 mm, screw length 33.30 ± 2.53 mm, and angulation laterally 43.20° ± 3.00°. Ma et al.[[13]] in China measured the C2 lamina from 120 cadaveric specimens and the mean ± SD results of the width, length, height, and angulation laterally were 5.87 mm, 26.68 mm, 12.68 mm, and 48.85°, respectively. Cassinelli et al.[[1]] in the USA measured 420 cadaveric specimens and the mean results were width –5.77 mm, length –24.6 mm, and angulation laterally –48.59° [[Table 5]].

This is the first study in lamina morphometry in Thai patients to reveal the mean width of 5.89 mm; however, compared with previous studies in China, Korea, and the USA, the results were similar –5.87 mm,[[13]] 5.66 mm,[[12]] and 5.77 mm,[[1]] respectively. However, the trend in the size of the lamina in width, height, and length in males was larger than in females in all studies.[[1]],[[12]],[[13]]
Conclusion
In the Thai samples, 8.8% had a C2 pedicle width <3.5 mm which would not allow insertion of screws; however, they could be replaced with laminar screws since the width was ≥3.5 mm. In this study, all of the patients who could not be inserted pedicle can be replaced with lamina screws inserted. The C2 pedicle and lamina of the males tended to be larger than in the females.
Conflict of Interest
There are no conflicts of interest.
Acknowledgment
Manuscript Editing by Glenn Shingledecker (International Affairs Office Faculty of Medicine Prince of Songkla University).
Financial support and sponsorship
Nil.
-
References
- 1 Cassinelli EH, Lee M, Skalak A, Ahn NU, Wright NM. Anatomic considerations for the placement of C2 laminar screws. Spine (Phila Pa 1976) 2006;31:2767-71.
- 2 Jeanneret B, Magerl F. Primary posterior fusion C1/2 in odontoid fractures: Indications, technique, and results of transarticular screw fixation. J Spinal Disord 1992;5:464-75.
- 3 Grob D, Jeanneret B, Aebi M, Markwalder TM. Atlanto-axial fusion with transarticular screw fixation. J Bone Joint Surg Br 1991;73:972-6.
- 4 Elliott RE, Tanweer O, Boah A, Morsi A, Ma T, Frempong-Boadu A, et al. Atlantoaxial fusion with transarticular screws: Meta-analysis and review of the literature. World Neurosurg 2013;80:627-41.
- 5 Harms J, Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine (Phila Pa 1976) 2001;26:2467-71.
- 6 Elliott RE, Tanweer O, Boah A, Morsi A, Ma T, Frempong-Boadu A, et al. Outcome comparison of atlantoaxial fusion with transarticular screws and screw-rod constructs: Meta-analysis and review of literature. J Spinal Disord Tech 2014;27:11-28.
- 7 Wajanavisit W, Lertudomphonwanit T, Fuangfa P, Chanplakorn P, Kraiwattanapong C, Jaovisidha S. Prevalence of high-riding vertebral artery and morphometry of C2 pedicles using a novel computed tomography reconstruction technique. Asian Spine J 2016;10:1141-8.
- 8 Parker SL, McGirt MJ, Garcés-Ambrossi GL, Mehta VA, Sciubba DM, Witham TF, et al. Translaminar versus pedicle screw fixation of C2: Comparison of surgical morbidity and accuracy of 313 consecutive screws. Neurosurgery 2009;64:343-8.
- 9 Bunmaprasert T, Treenarong N, Khamkhad A. Appropriate size and angulation for axis screw placement. J Med Assoc Thai 2015;98:188-95.
- 10 Liu J, Napolitano JT, Ebraheim NA. Systematic review of cervical pedicle dimensions and projections. Spine (Phila Pa 1976) 2010;35:E1373-80.
- 11 Yusof MI, Ming LK, Abdullah MS. Computed tomographic measurement of cervical pedicles for transpedicular fixation in a Malay population. J Orthop Surg (Hong Kong) 2007;15:187-90.
- 12 Kim YJ, Rhee WT, Lee SB, You SH, Lee SY. Computerized tomographic measurements of morphometric parameters of the C2 for the feasibility of laminar screw fixation in Korean population. J Korean Neurosurg Soc 2008;44:15-8.
- 13 Ma XY, Yin QS, Wu ZH, Xia H, Riew KD, Liu JF. C2 anatomy and dimensions relative to translaminar screw placement in an Asian population. Spine (Phila Pa 1976) 2010;35:704-8.
Address for correspondence
Publication History
Received: 18 October 2019
Accepted: 13 November 2019
Article published online:
16 August 2022
© 2020. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Cassinelli EH, Lee M, Skalak A, Ahn NU, Wright NM. Anatomic considerations for the placement of C2 laminar screws. Spine (Phila Pa 1976) 2006;31:2767-71.
- 2 Jeanneret B, Magerl F. Primary posterior fusion C1/2 in odontoid fractures: Indications, technique, and results of transarticular screw fixation. J Spinal Disord 1992;5:464-75.
- 3 Grob D, Jeanneret B, Aebi M, Markwalder TM. Atlanto-axial fusion with transarticular screw fixation. J Bone Joint Surg Br 1991;73:972-6.
- 4 Elliott RE, Tanweer O, Boah A, Morsi A, Ma T, Frempong-Boadu A, et al. Atlantoaxial fusion with transarticular screws: Meta-analysis and review of the literature. World Neurosurg 2013;80:627-41.
- 5 Harms J, Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine (Phila Pa 1976) 2001;26:2467-71.
- 6 Elliott RE, Tanweer O, Boah A, Morsi A, Ma T, Frempong-Boadu A, et al. Outcome comparison of atlantoaxial fusion with transarticular screws and screw-rod constructs: Meta-analysis and review of literature. J Spinal Disord Tech 2014;27:11-28.
- 7 Wajanavisit W, Lertudomphonwanit T, Fuangfa P, Chanplakorn P, Kraiwattanapong C, Jaovisidha S. Prevalence of high-riding vertebral artery and morphometry of C2 pedicles using a novel computed tomography reconstruction technique. Asian Spine J 2016;10:1141-8.
- 8 Parker SL, McGirt MJ, Garcés-Ambrossi GL, Mehta VA, Sciubba DM, Witham TF, et al. Translaminar versus pedicle screw fixation of C2: Comparison of surgical morbidity and accuracy of 313 consecutive screws. Neurosurgery 2009;64:343-8.
- 9 Bunmaprasert T, Treenarong N, Khamkhad A. Appropriate size and angulation for axis screw placement. J Med Assoc Thai 2015;98:188-95.
- 10 Liu J, Napolitano JT, Ebraheim NA. Systematic review of cervical pedicle dimensions and projections. Spine (Phila Pa 1976) 2010;35:E1373-80.
- 11 Yusof MI, Ming LK, Abdullah MS. Computed tomographic measurement of cervical pedicles for transpedicular fixation in a Malay population. J Orthop Surg (Hong Kong) 2007;15:187-90.
- 12 Kim YJ, Rhee WT, Lee SB, You SH, Lee SY. Computerized tomographic measurements of morphometric parameters of the C2 for the feasibility of laminar screw fixation in Korean population. J Korean Neurosurg Soc 2008;44:15-8.
- 13 Ma XY, Yin QS, Wu ZH, Xia H, Riew KD, Liu JF. C2 anatomy and dimensions relative to translaminar screw placement in an Asian population. Spine (Phila Pa 1976) 2010;35:704-8.