

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_278_18
Hydrocephalus after gamma knife radiosurgery for schwannoma
Authors

Objective: Gamma Knife radiosurgery (GKRS) has been established as an effective and safe treatment for intracranial Schwannoma. However, communicating hydrocephalus can occur after GKRS. The risk factors of this disorder are not yet fully understood. The objective of the study was to assess potential risk factors for hydrocephalus after GKRS. Methods: We retrospectively reviewed the medical radiosurgical records of 92 patients who underwent GKRS to treat intracranial Schwannoma and developed communicating hydrocephalus. The following parameters were analyzed as potential risk factors for hydrocephalus after GKRS: age, sex, target volume, irradiation dose, prior tumor resection, treatment technique, tumor enhancement pattern, and protein level of cerebrospinal fluid (CSF) after GKRS. Results: Of the 92 patients, eight of them developed communicating hydrocephalus. Target volume and tumor enhancement pattern, and protein level of CSF ware associated with the development of hydrocephalus. Conclusion: In particular, patients with intracranial Schwannomas with large tumor size, ring enhancement patterns, and high protein level of CSF should be carefully observed.
Introduction
Intracranial Schwannoma is estimated to account for 5%–9% of all intracranial tumors, most of which are vestibular Schwannoma (VS). Surgical resection is the gold standard treatment method for intracranial Schwannoma. However, intracranial surgery carries the considerable possibility of complications involving cranial nerve injury.[[1]],[[2]] In recent years, many authors have reported that Gamma Knife radiosurgery (GKRS) is effective for tumor control and the preservation of cranial nerve function for intracranial Schwannoma.[[3]],[[4]],[[5]] In contrast to open surgery, GKRS does not require anesthesia and is less invasive. However, patients who undergo GKRS can experience complications such as edema, cyst formation, and hydrocephalus as adverse radiation effects.[[6]] Radiosurgery may aggravate cerebrospinal fluid (CSF) malabsorption by causing radiation necrosis, with elevated CSF protein levels.[[1]],[[5]] In addition, it is unclear whether further surgical intervention is necessary for those patients who develop communicating hydrocephalus. The aim of this retrospective cohort study is to determine the incidence of communicating hydrocephalus developing after two treatment modalities for VS.
Methods
Between February 2000 and December 2015, 92 patients who presented to our institute were diagnosed with VS underwent GRKS. Characteristics of these patients are shown in [[Table 1]]. By examining both the medical records and neuroradiological imaging of these patients, we were able to retrospectively review the presence of newly developed hydrocephalus and potential risk factors for hydrocephalus after GKRS. The diagnosis of hydrocephalus was made from the following established criteria: (1) disproportionate enlargement of the ventricles relative to the degree of sulcal prominence, (2) enlargement of the anterior third ventricle with reduction of the mamillopontine distance, and (3) uniform smooth thinning and elevation of the corpus callosum.[[7]] To distinguish GKRS-related hydrocephalus from senile hydrocephalus, we added to the assessment time of occurrence of hydrocephalus and sudden worsening of the symptom. According to several reports, GKRS-related hydrocephalus developed within 24 months postoperative.[[6]],[[8]],[[9]]

Results
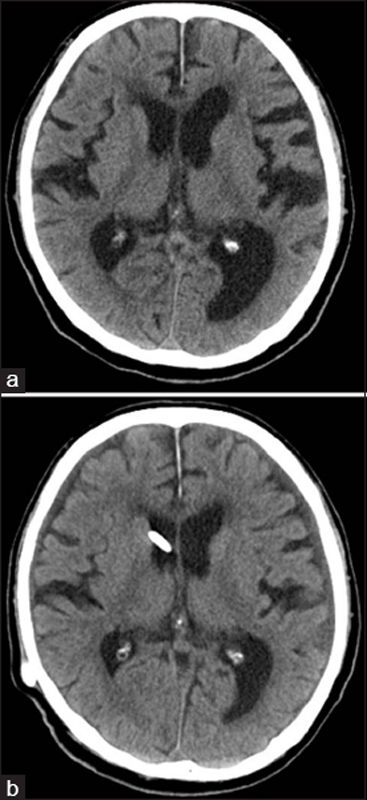
The patient population in total, 92 patients underwent GKRS for intracranial Schwannoma. The mean patient age was 61.3 years (range: 26–82 years); 61 patients were female and 31 patients were male. With respect to tumor enhancement pattern, 36 patients were classified in homogeneously enhanced pattern and 56 patients were classified in ring-enhanced pattern [[Table 1]] and [[Figure 1]]. Hydrocephalus occurred in eight patients after GKRS; all of them had communicating hydrocephalus [[Figure 2]]. Shunt operations were performed for all patients. Of all the patients with communicating hydrocephalus, while three did not present any symptoms, two complained of headache, and three suffered from dizziness. CSF protein levels increased. The time of occurrence of hydrocephalus after GKRS ranged from 3 to 24 months. Most cases of hydrocephalus occurred within 6 months after GKRS [[Table 2]]. Potential risk factors for hydrocephalus ware target volume and tumor enhancement pattern, and protein level of CSF. Univariate analysis revealed that the tumor enhancement pattern had a significant association with the development of communicating hydrocephalus [[Table 3]].



Discussion
Several interventions are available for the treatment of VS.
When compared to radiosurgery, surgical resection results in a high rate of complete tumor removal and a low recurrence rate for large tumors.[[8]],[[10]],[[11]] However, stereotactic radiosurgery is considered to be a less invasive alternative to surgical resection and has been increasingly utilized over the past 20 years for the treatment of VS <3 cm in size.[[12]],[[13]]
Previous studies have shown radiosurgery to have a high control rate of tumor growth and a low morbidity rate, allowing for the preservation of facial and auditory function.[[11]],[[14]] Accordingly, surgical resection and stereotactic radiosurgery are both good treatment options for the management of VS, despite the known complications associated with each of these procedures. Hydrocephalus is a known complication of GKRS treatment for VS, occurring in approximately 4%–14% of patients.[[15]] With an increasing number of patients presenting with VS, and those who are treated using GKS in particular, understanding the pathogenesis of the development of hydrocephalus is crucial for the management of these patients. It has been suggested that communicating hydrocephalus accompanying VS is caused by tumor necrosis with subsequent CSF protein elevation.[[16]] Elevated CSF protein levels may lead to CSF malabsorption at the level of the arachnoid granulations.[[17]] The lumbar CSF protein concentration in all the 92 patients was analyzed, and hydrocephalus was reported to be related to high protein levels in the CSF. Elevated CSF protein was a causative factor for hydrocephalus after GKRS. High protein concentration in the CSF was considered the main contributing factor for HCP, given that several studies showed elevated intraventricular CSF protein concentrations 1.6–15 times above the normal levels in HCP cases.[[18]] Similar to our study, a few investigations indicated a statistical association between the hydrocephalus and the cerebrospinal fluid protein density. In the current study, a low concentration CSF proteins were found to be associated with a lower risk of developing hydrocephalus after GKRS. Nagano et al.[[19]] compared the radiosurgery results of Schwannoma with different enhancement patterns and found that patients with ring enhancement patterns showed an earlier response and were more sensitive to treatment than patients with homogeneous patterns. In the present study, the ring enhancement group was more likely to represent hydrocephalus. The age has also been suggested as another causative factor. Tanaka et al.[[20]] reported that the incidence of hydrocephalus was 12-fold higher in elderly patients (25%) than in younger patients (2.1%). It is also suggested that the increased incidence of communicating hydrocephalus in the elderly population is due to a decrease in the reserve capacity of CSF absorption due to aging. Even a mild increase in the CSF protein released from the Schwannomas may induce the proliferation of arachnoid cells in elderly patients. This is important because the proliferation of arachnoid cells has been hypothesized to drive the pathogenesis of hydrocephalus. In the present study, age was not significantly associated with the development of hydrocephalus, even though the age distribution of our patient population was similar to that in the study by Tanaka et al. An additional difference between the present study and the study is that we considered the period of time post-GKRS that it took for hydrocephalus to develop. One possible explanation for the results is that elderly patients with senile hydrocephalus may have been included because hydrocephalus occurs after long post-GKRS periods. The present study did have a few limitations. We cannot completely exclude the possibility of senile hydrocephalus. Thus, future studies that can distinguish senile hydrocephalus will be.
Conclusion
Communicating hydrocephalus developed in 8 patients (8.7%). In addition, cases of intracranial Schwannoma with large tumor size, ring enhancement patterns, and high protein level of CSF should be closely monitored for the development of hydrocephalus.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Samii M, Matthies C. Management of 1000 vestibular schwannomas (acoustic neuromas): The facial nerve--preservation and restitution of function. Neurosurgery 1997;40:684-94.
- 2 Park CK, Lee SH, Choi MK, Choi SK, Park BJ, Lim YJ, et al. Communicating hydrocephalus associated with intracranial schwannoma treated by gamma knife radiosurgery. World Neurosurg 2016;89:593-600.
- 3 Flickinger JC, Kondziolka D, Niranjan A, Lunsford LD. Results of acoustic neuroma radiosurgery: An analysis of 5 years' experience using current methods. J Neurosurg 2001;94:1-6.
- 4 Hasegawa T, Kida Y, Kobayashi T, Yoshimoto M, Mori Y, Yoshida J, et al. Long-term outcomes in patients with vestibular schwannomas treated using gamma knife surgery: 10-year follow up. J Neurosurg 2005;102:10-6.
- 5 Pollock BE, Foote RL, Stafford SL. Stereotactic radiosurgery: The preferred management for patients with nonvestibular schwannomas? Int J Radiat Oncol Biol Phys 2002;52:1002-7.
- 6 Roche PH, Khalil M, Soumare O, Régis J. Hydrocephalus and vestibular schwannomas: Considerations about the impact of gamma knife radiosurgery. Prog Neurol Surg 2008;21:200-6.
- 7 Rogg JM, Ahn SH, Tung GA, Reinert SE, Norén G. Prevalence of hydrocephalus in 157 patients with vestibular schwannoma. Neuroradiology 2005;47:344-51.
- 8 Jeon CJ, Kong DS, Nam DH, Lee JI, Park K, Kim JH, et al. Communicating hydrocephalus associated with surgery or radiosurgery for vestibular schwannoma. J Clin Neurosci 2010;17:862-4.
- 9 Fukuda M, Oishi M, Kawaguchi T, Watanabe M, Takao T, Tanaka R, et al. Etiopathological factors related to hydrocephalus associated with vestibular schwannoma. Neurosurgery 2007;61:1186-92.
- 10 Pirouzmand F, Tator CH, Rutka J. Management of hydrocephalus associated with vestibular schwannoma and other cerebellopontine angle tumors. Neurosurgery 2001;48:1246-53.
- 11 Pollock BE, Driscoll CL, Foote RL, Link MJ, Gorman DA, Bauch CD, et al. Patient outcomes after vestibular schwannoma management: A prospective comparison of microsurgical resection and stereotactic radiosurgery. Neurosurgery 2006;59:77-85.
- 12 Bloch J, Vernet O, Aubé M, Villemure JG. Non-obstructive hydrocephalus associated with intracranial schwannomas: Hyperproteinorrhachia as an etiopathological factor? Acta Neurochir (Wien) 2003;145:73-8.
- 13 Hasegawa T, Fujitani S, Katsumata S, Kida Y, Yoshimoto M, Koike J, et al. Stereotactic radiosurgery for vestibular schwannomas: Analysis of 317 patients followed more than 5 years. Neurosurgery 2005;57:257-65.
- 14 Régis J, Pellet W, Delsanti C, Dufour H, Roche PH, Thomassin JM, et al. Functional outcome after gamma knife surgery or microsurgery for vestibular schwannomas. J Neurosurg 2002;97:1091-100.
- 15 Norén G. Long-term complications following gamma knife radiosurgery of vestibular schwannomas. Stereotact Funct Neurosurg 1998;70 Suppl 1:65-73.
- 16 Cauley KA, Ratkovits B, Braff SP, Linnell G. Communicating hydrocephalus after gamma knife radiosurgery for vestibular schwannoma: An MR imaging study. AJNR Am J Neuroradiol 2009;30:992-4.
- 17 Sawamura Y, Shirato H, Sakamoto T, Aoyama H, Suzuki K, Onimaru R, et al. Management of vestibular schwannoma by fractionated stereotactic radiotherapy and associated cerebrospinal fluid malabsorption. J Neurosurg 2003;99:685-92.
- 18 Lee S, Seo SW, Hwang J, Seol HJ, Nam DH, Lee JI, et al. Analysis of risk factors to predict communicating hydrocephalus following gamma knife radiosurgery for intracranial schwannoma. Cancer Med 2016;5:3615-21.
- 19 Nagano O, Higuchi Y, Serizawa T, Ono J, Matsuda S, Yamakami I, et al. Transient expansion of vestibular schwannoma following stereotactic radiosurgery. J Neurosurg 2008;109:811-6.
- 20 Tanaka Y, Kobayashi S, Hongo K, Tada T, Sato A, Takasuna H, et al. Clinical and neuroimaging characteristics of hydrocephalus associated with vestibular schwannoma. J Neurosurg 2003;98:1188-93.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Samii M, Matthies C. Management of 1000 vestibular schwannomas (acoustic neuromas): The facial nerve--preservation and restitution of function. Neurosurgery 1997;40:684-94.
- 2 Park CK, Lee SH, Choi MK, Choi SK, Park BJ, Lim YJ, et al. Communicating hydrocephalus associated with intracranial schwannoma treated by gamma knife radiosurgery. World Neurosurg 2016;89:593-600.
- 3 Flickinger JC, Kondziolka D, Niranjan A, Lunsford LD. Results of acoustic neuroma radiosurgery: An analysis of 5 years' experience using current methods. J Neurosurg 2001;94:1-6.
- 4 Hasegawa T, Kida Y, Kobayashi T, Yoshimoto M, Mori Y, Yoshida J, et al. Long-term outcomes in patients with vestibular schwannomas treated using gamma knife surgery: 10-year follow up. J Neurosurg 2005;102:10-6.
- 5 Pollock BE, Foote RL, Stafford SL. Stereotactic radiosurgery: The preferred management for patients with nonvestibular schwannomas? Int J Radiat Oncol Biol Phys 2002;52:1002-7.
- 6 Roche PH, Khalil M, Soumare O, Régis J. Hydrocephalus and vestibular schwannomas: Considerations about the impact of gamma knife radiosurgery. Prog Neurol Surg 2008;21:200-6.
- 7 Rogg JM, Ahn SH, Tung GA, Reinert SE, Norén G. Prevalence of hydrocephalus in 157 patients with vestibular schwannoma. Neuroradiology 2005;47:344-51.
- 8 Jeon CJ, Kong DS, Nam DH, Lee JI, Park K, Kim JH, et al. Communicating hydrocephalus associated with surgery or radiosurgery for vestibular schwannoma. J Clin Neurosci 2010;17:862-4.
- 9 Fukuda M, Oishi M, Kawaguchi T, Watanabe M, Takao T, Tanaka R, et al. Etiopathological factors related to hydrocephalus associated with vestibular schwannoma. Neurosurgery 2007;61:1186-92.
- 10 Pirouzmand F, Tator CH, Rutka J. Management of hydrocephalus associated with vestibular schwannoma and other cerebellopontine angle tumors. Neurosurgery 2001;48:1246-53.
- 11 Pollock BE, Driscoll CL, Foote RL, Link MJ, Gorman DA, Bauch CD, et al. Patient outcomes after vestibular schwannoma management: A prospective comparison of microsurgical resection and stereotactic radiosurgery. Neurosurgery 2006;59:77-85.
- 12 Bloch J, Vernet O, Aubé M, Villemure JG. Non-obstructive hydrocephalus associated with intracranial schwannomas: Hyperproteinorrhachia as an etiopathological factor? Acta Neurochir (Wien) 2003;145:73-8.
- 13 Hasegawa T, Fujitani S, Katsumata S, Kida Y, Yoshimoto M, Koike J, et al. Stereotactic radiosurgery for vestibular schwannomas: Analysis of 317 patients followed more than 5 years. Neurosurgery 2005;57:257-65.
- 14 Régis J, Pellet W, Delsanti C, Dufour H, Roche PH, Thomassin JM, et al. Functional outcome after gamma knife surgery or microsurgery for vestibular schwannomas. J Neurosurg 2002;97:1091-100.
- 15 Norén G. Long-term complications following gamma knife radiosurgery of vestibular schwannomas. Stereotact Funct Neurosurg 1998;70 Suppl 1:65-73.
- 16 Cauley KA, Ratkovits B, Braff SP, Linnell G. Communicating hydrocephalus after gamma knife radiosurgery for vestibular schwannoma: An MR imaging study. AJNR Am J Neuroradiol 2009;30:992-4.
- 17 Sawamura Y, Shirato H, Sakamoto T, Aoyama H, Suzuki K, Onimaru R, et al. Management of vestibular schwannoma by fractionated stereotactic radiotherapy and associated cerebrospinal fluid malabsorption. J Neurosurg 2003;99:685-92.
- 18 Lee S, Seo SW, Hwang J, Seol HJ, Nam DH, Lee JI, et al. Analysis of risk factors to predict communicating hydrocephalus following gamma knife radiosurgery for intracranial schwannoma. Cancer Med 2016;5:3615-21.
- 19 Nagano O, Higuchi Y, Serizawa T, Ono J, Matsuda S, Yamakami I, et al. Transient expansion of vestibular schwannoma following stereotactic radiosurgery. J Neurosurg 2008;109:811-6.
- 20 Tanaka Y, Kobayashi S, Hongo K, Tada T, Sato A, Takasuna H, et al. Clinical and neuroimaging characteristics of hydrocephalus associated with vestibular schwannoma. J Neurosurg 2003;98:1188-93.