Key-words:
Anterior cervical discectomy - fusion - outcome - stand alone
Introduction
Since its introduction in the 1950s, anterior cervical discectomy with fusion (ACDF)
has been established as the gold standard technique for the treatment of symptomatic
degenerative cervical disease (DCD), providing excellent results in most patients.[[1]] The use of anterior plating is typically suggested in multilevel discectomies to
provide better stability. The necessity, however, of this technique has been questioned
over the years since similar results can be achieved employing the stand-alone technique,
especially in one- or two-level surgery.[[2]],[[3]] The article aims to assess the fusion rates (FRs) and long-term outcomes following
three-level ACDF without the use of an anterior plate.
Materials and Methods
Patients
Data were retrospectively collected from the medical records of 78 patients primary
operated on for symptomatic DCD at three-cervical spine levels due to electromyographic
and radiographic magnetic resonance imaging (MRI) evidence of compressed cervical
nerve roots or spinal cord by ossified bony elements or herniated disc, with concordant
radiculopathy and/or myelopathy symptoms. No trauma patients were included in this
study. Due to lack of set norms in the literature, regarding the time of eligibility
of these patients for a surgical procedure, our department's protocol was followed,
offering surgery to patients with persistent neck and/or upper extremity pain and/or
neurological deficits, without previous physical therapy treatment.
Surgical technique
All patients were treated with three-level ACDF, by a single surgical team, employing
the standard Smith–Robinson approach.[[4]] The cartilaginous disc end plate was removed, while excessive care was taken to
avoid any damage of the bony end plate, followed by osteophytectomy and foraminotomy
in the vast majority of cases. Radiographic-guided trials were employed in the size
selection process of the polyether ether ketone (PEEK) cages. Autologous local decompression
bone as well as synthesized hydroxyapatite–collagen artificial bone was used to fill
the cages thus promotingfusion.
Outcome assessment
Clinical assessment (visual analog scale [VAS] of the neck and arm,[[5]] and neck disability index [NDI][[6]]) and radiological assessment (plain radiograph) were performed once per month until
fusion was accomplished as a part of the surgical team's follow-up protocol. Postsurgery
MRI was conducted in patients that presented with radiographic signs of myelopathy
(high signal on T2 sequence) on the preoperative imaging. FR was evaluated employing
the <1 mm motion between the spinous processes system.[[7]] Subsidence was defined as a more than 2 mm decrease of the interbody height.[[8]] Plain radiograph measurements were compered to MRI to define magnification by an
experienced independent radiologist. Patient follow-up was 69.47 ± 11.45 months. All
data management and analysis were performed using the IBM SPSS v. 21 software (SPSS
Inc., Chicago, IL, USA). Normality was assessed employing the Shapiro-Wilk test. Descriptive
data were presented as Mean and Standard Deviation. Qualitative data were tested employing
chi-squared test, while quantitative were assessed by a t-test. A statistically significant
difference between comparative groups was considered at the 95% confidence interval
(P ≤ 0.05).
Results
Clinical and radiological characteristics
A total of 234 treated levels on 78 patients, 43 (55.2%) male and 35 (44.8%) female,
with a mean age of 50.73 ± 8.88 (minimum: 30; maximum: 71) years were assessed after
treated with three-level ACDF. The mean presurgery NDI score was 23.07 ± 4.86 (minimum:
13; maximum: 34), with a mean disability of 46.03% ± 9.64 [[Table 1]]. The mean presurgery VAS score of the neck was 7.58 ± 0.85 (minimum: 6; maximum:
9), while VAS of the arm was 7.75 ± 1.008 (minimum: 6; maximum: 9) [[Table 2]] and [[Table 3]].
 Table 1: Neck Disability Index patient scores
Table 1: Neck Disability Index patient scores
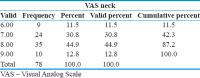 Table 2: Self-reported isual analog scale - neck pain level
Table 2: Self-reported isual analog scale - neck pain level
 Table 3: Self-reported Visual analog scale - arm pain level
Table 3: Self-reported Visual analog scale - arm pain level
During the presurgery evaluation, 12 (15.38%) patients manifested a high T2 sequence
signal. MRI screening detected 31 (39.24%) patients with coexisting cervical and lumbar
radiographical findings.
Surgical data
The surgical time was approximately. 3.16 h ± 0.29. Hospitalization extended for 2.22
± 0.42 days.
Complications
Post surgery, transient dysphagia was reported by 1 patient (1.28%), while from the
total number of operated levels subsidence was registered in 15 (6.41%) situated in
12 patients (15.38%), most often at C6-7 level (66.6%) [[Table 4]].
 Table 4: Subsidence incidence per level employing the more than 2 mm decrease of the interbody
height Subsidence
Table 4: Subsidence incidence per level employing the more than 2 mm decrease of the interbody
height Subsidence
Outcome
Post surgery, NDI stated no disability (1.93 ± 0.87; minimum: 1 and maximum: 3), as
shown in [[Table 5]], while VAS score of the neck and arm showed no presence of pain (neck: 0.10 ± 0.30;
minimum: 0 and maximum: 1, arm: 0.19 ± 0.53; minimum: 0 and maximum: 3) as manifested
in [[Table 6]] and [[Table 7]]. The mean FR was 19.50 ± 21.71 levels per month (minimum: 0; maximum: 51), with
a maximum peak from 3rd to 6th month [[Figure 2]]. Post surgery, high signal resolved in 8 (66.6%) at 12-month follow-up.
 Table 5: Neck Disability Index scores on first post surgery follow-up
Table 5: Neck Disability Index scores on first post surgery follow-up
 Table 6: Self-reported Visual Analog Scale grade for neck pain on first post-surgery follow-up
Table 6: Self-reported Visual Analog Scale grade for neck pain on first post-surgery follow-up
 Table 7: Self-reported Visual Analog Scale grade for arm pain on first post-surgery follow-up
Table 7: Self-reported Visual Analog Scale grade for arm pain on first post-surgery follow-up
Discussion
To our knowledge, there are scarce mentions of three or more level ACDF without anterior
plating in the literature. Anterior cervical plating was popularized in the early
1980s and remains a widely used technique, especially in the treatment of three and
more levels, as it is believed to positively influence alignment and outcome.[[9]] However, the necessity of plating is controversial if Wolff's law of biomechanics
is taken into consideration, according to which bone formation is stimulated by mechanical
loading, a law on which the superior results of dynamic plating were attributed.[[10]] Based on the aforementioned results, we could conclude that taking the plate out
of the occasion would result in even higher FRs in a shorter period of time as supported
further, by the results of this study. Literature also shows good postsurgery results
in patients who were treated with only interbody spacers for up to four levels, with
one case report advocating the safety of employing this technique for up to five levels.[[11]],[[12]] Bagby advocate the use of stand-alone cages in ACDF based on the distraction–compression
principle.[[13]] The results of this study support the aforementioned theory.
The assessment was performed employing NDI and VAS scoring systems, as well as clinical
neurological evaluation. Most of the patients presented with moderate disability (46.03%
± 9.64%; NDI 23.07 ± 4.86) and reported VAS pain of the neck: 7.58 ± 0.85/arm: 7.75
± 1.008. Post surgery, none of the patients reported any disability or pain (NDI:
0–3; VAS neck: 0–1; VAS arm: 0–3) (P < 0.001 – NDI; P = 0.004 – VAS neck; P = 0.002
– VAS arm). Our good results support the literature, showing up a 90% likelihood of
relief of radicular pain and stabilization.[[14]]
Some researchers advocate the use of a low focal T1 and/or high T2 signal as a negative
prognostic factor regarding posttreatment outcome, while others defy this.[[15]],[[16]],[[17]],[[18]],[[19]],[[20]],[[21]] Our results support the last as during presurgery evaluation, 12 (15.38%) of the
patients manifested a high intense T2 signal, without compromising the results. The
aforementioned results, however, could be associated with a higher NDI score (ranging
from 27 to 34). No association with VAS was observed. We support the use of diffusion
tensor imaging, a relatively new promising technique which detects the random motion
of water molecules, providing information about cellular integrity/pathology, thus
detecting white matter damage before a high T2 signal appears, presenting a great
tool in the presurgery evaluation. Our patients were also MRI screened for degenerative
lumbar syndrome (DLS) resulting in 31 (39.24%) patients, having coexisting cervical
and lumbar manifestations, some of who were operated on for both in one act. Literature
suggests that coexisting lumbar stenosis is a fairly common (up to 28%) finding in
these patients and one may mask the symptoms of the other; therefore, patients with
lumbar stenosis should also be evaluated for DCD and vice versa.[[22]],[[23]],[[24]]
The goal of operative treatment is the decompression of the spinal cord without compromising
alignment and stability. All of our patients received stand-alone PEEK interbody spacers
embedded with local decompression bone and/or hydroxyapatite–collagen artificial bone,
a widely used technique providing superior FRs, while avoiding the donor site morbidity
associated with iliac crest harvesting.[[25]],[[26]]
Recent literature suggests numerous available methods to assess fusion and thus diagnose
pseudoarthrosis, resulting often in a disagreement between surgeons and reviewers.
Oshina et al. in their extensive review found 10 fusion criteria and concluded that
the presence of trabecular bone between the end plates was the most commonly used
definition. However, the authors found the particular classification highly subjective
and recommended the use of the <1 mm of motion between spinous processes on the extension
and flexion system to confirm fusion [[7]] [[Figure 1]]. Furthermore, FRs were reported as 90.2% at 1 year and 94.7% at 2 years.[[7]] Based on the aforementioned results, the second criteria system was employed in
the evaluation process. The 1st year FR was 100%, with a significant peak registered
between months 3 and 6, as shown in [[Figure 2]]. Moreover, there is a common belief that fusion is not possible during the 1st
month postsurgery; however, 7.70% of the treated levels fulfilled the criteria for
being classified as fused, thus manifesting that early fusion is possible.
 Figure 1: Postsurgery plain radiograph in hyperextension and hyperflexion, used in fusion rate
evaluation employing the <1 mm movement between the spinal processes system
Figure 1: Postsurgery plain radiograph in hyperextension and hyperflexion, used in fusion rate
evaluation employing the <1 mm movement between the spinal processes system
 Figure 2: Fusion Rate per month assessed employing the <1 mm of motion between the spinous
processes criteria
Figure 2: Fusion Rate per month assessed employing the <1 mm of motion between the spinous
processes criteria
Adjacent segment disease (ASD) is a broad term describing new postsurgery findings,
such as intervertebral disc herniation, hypertrophic facet arthritis, listhesis, instability,
scoliosis, and vertebral compression fracture in patients treated with fusion techniques,
especially in those with single-level arthrodesis involving the C5-6 vertebrae and
preexisting radiographic evidence of adjacent level degeneration.[[27]] The leading opinion is that altered biomechanical status of the cervical spine
due to arthrodesis as well as the disruption of anatomical structures including even
soft-tissue damage results in an increase of intradiscal pressure, leading to the
degeneration of the adjacent segment intervertebral discs (evidence level III).[[28]],[[29]],[[30]] Literature advocates that in case the surgeon uses the cervical plating technique,
the plate-to-disc distance can contribute at a great extend in the progression of
ASD if the plate is positioned <3 mm from the adjacent disc and as a result, a gap
of at least 5 mm should be used.[[31]],[[32]] The avoidance of plating should diminish the incidence of ASD, as shown in this
study, as none of the patients presented with the same in the long term.
Dysphagia and dysphonia are the most common complications, with rates 1%–79%.[[33]],[[34]] Dysphagia presents a controversial entity associated with soft-tissue swelling,
recurrent laryngeal nerve (RLN) palsy, pharyngeal plexus denervation, direct injury,
and regional esophageal ischemia. Likewise, dysphonia is associated with RLN palsy,
while it can also present due to the direct trauma of the vocal cords during intubation.
One patient presented with self-reported dysphagia (1.28%) subsiding a month postsurgery.
None of our patients presented with dysphonia. The aforementioned results may be associated
with the absence of an anterior plate, application of retraction with periodic pressure
release, and fine soft-tissue handling.
Subsidence presents an important radiographic finding, resulting in a long-term foraminal
reduction. The literature reports an incidence of 8.1%–44.77%.[[25]],[[29]] We registered 15 (6.41%) subsidence in 234 operated interbody spaces, without compromising
clinical outcome. Subsidence is a multifactorial radiographic finding and it does
not depend solely on the presence or absence of a plate. The literature suggests that
greater distance between anterior cage rim and vertebral body and less contact surface
between cage and end plate are significant risk factors due to increased stress applied
on the surface of the end plate.[[35]] Low bone mineral density, excessive distraction during interbody-spacer application,
and intraoperative end-plate damage can also increase the incidence. The good results
demonstrated in this study may be associated with proper preparation of patients and
fine manipulation, thus reduction of bone damage and selection of proper cage height
and AP diameter. A very interesting finding was that the most common level of subsidence
was the C6-7, registered in as many as 66.6% of the cases, a finding in accordance
with the literature.[[36]] However, none of the patients' outcome or FR was affected despite negative radiological
measurements in our study or in recently published papers.
Last but not least, we have to take into consideration the surgical time which is
shorter in the employment of our technique (our mean surgical time was approximately
3 h 16 m), as well as the socioeconomical gain as less materials are introduced (Greece's
lowest price found according to the National Health System Observatory for anterior
plate 536€), thus decreasing surgical team fee due to less procedures performed (National
Insurance Program per ICD for ACDF with plating 6000€ including 7 hospitalization
days).[[37]],[[38]] As a result, a sum of 41.808€ was saved from the National Insurance System, Private
Sector Insurance System, and Personal Funds of the Health Services Users, without
introducing into the equation the fee difference of the surgical team.
Conclusion
ACDF without the use of an anterior plate in three levels is a safe, cost-effective
technique providing good short, intermediate, and long-term clinical results with
a minimal incidence of complications. The use of stand-alone cages can provide similar
or better FRs compared to plating. Subsidence can occur, but it is clinically insignificant.
Correct cage size selection and positioning may lower its incidence. Patients presenting
with DCD should be also screened for DLS as a significant incidence of coexistence
can be detected, thus providing the opportunity of dual treatment in one act that
could result in even better outcomes.





