

RSS-Feed abonnieren
DOI: 10.4103/ajns.AJNS_155_18
Outcome analysis of surgical clipping for incidental internal carotid posterior communicating and anterior choroidal artery aneurysms
Autor*innen

Introduction: Surgical outcome and ischemic complications of Internal carotid Posterior Communicating (IC PC) and anterior choroidal aneurysms have been questionable due to frequent occlusion of the anterior choroid artery and also due to low incidence of true anterior choroid artery aneurysms. The present series describes the postoperative outcome after clipping of such aneurysms at a single centre. Methods: A retrospective analysis of 73 cases with IC PC and Anterior choroidal aneurysms performed at a Fujita Health University, Banbuntane Hotokukai Hospital, Nagoya, Aichi, Japan from 2014 to 2018 have been studied and emphasis is made on the demography and ischemic complications. Results: A total of 73 patients with IC PC and anterior choroidal aneurysms were studied, out of which 57 patient had a true IC PC aneurysm, 14 patients had aneurysms involving the anterior choroidal artery and only 2 patients had aneurysms which involved both the IC PC and the anterior choroidal arteries. None of the patients had a permanent Anterior Choroidal Artery syndrome, whereas only 2 out of the 73 patients had postoperative complications in the form of transient hemiparesis. Conclusion: Ischemic complications following surgical clipping of IC PC and anterior choroidal aneurysms can be minimised by meticulous micro dissection to identify the anterior choroidal artery thus preserving the patency of the same.
Key-words:
Anterior choroidal artery - anterior choroidal artery syndrome - incidental aneurysms internal carotid-posterior communicatingIntroduction
Internal carotid-posterior communicating (IC PC) aneurysms are the second-most common intracranial aneurysms seen in neurosurgical practice amounting to about 25% of all aneurysms and about 50% of internal carotid aneurysms.[[1]] They usually present with either a typical subarachnoid hemorrhage (SAH) or oculomotor nerve (OcM) palsy. However, due to variable anatomy of these aneurysms, they are considered to be the easiest and also the trickiest ones to operate on. On the other hand, anterior choroidal artery (ACho artery) aneurysms are rare comprising about 2%–5% of all intracranial aneurysms and there are very few case reports involving the microsurgical management of the same.[[2]] The present study aims at the results of a series of IC PC and ACho artery aneurysms operated at a tertiary referral center.
Surgical anatomy
Posterior communicating artery
The posterior communicating artery (PComA) arises from the posterolateral wall of the communicating segment of the internal carotid artery (ICA) within the carotid cistern [[Figure 1]]. Within this cistern, the artery is encased by an arachnoid membrane throughout its course. It enters the interpeduncular cistern by piercing the Liliequist membrane, which is the thick arachnoid membrane between the interpeduncular cistern inferiorly and the chiasmatic and carotid cisterns superiorly. Sometimes, the PComA might be attached to the posterior clinoid process while it passes the dura of the same. Rarely, it might run along a sulcus in the posterior clinoid process. The artery usually runs medial to the OcM [[Figure 1]] which enters the dura lateral to the posterior clinoid process and medial to the dural band passing from the tentorium toward the anterior clinoid process. The PComA then takes a posteromedial course toward the interpeduncular fossa and joins the posterior cerebral artery, thus forming the beginning of the P2 segment[[3]] [[Figure 1]].

Gibo et al. reported a superolateral course of the artery toward the OcM when the fetal configuration is present.[[4]] However, Avci and Baskaya[[5]] reported that the PComA always lies medial to the third nerve in all configurations. Children are found to have larger PComA (39%–75%) than in adults (8%–29%),[[6]] which supports the evidence that the caliber of this vessel diminishes with age. Yasargil reported that the size of the PComA is smaller than the corresponding posterior cerebral artery in 67.5% of the cases and its size is equal to or larger than the posterior cerebral artery in 32.5% of the cases, based on his observation on 400 cadaveric cerebral hemispheres.[[7]] In such situations, the PComA fails to regress, leaving the corresponding P1 segment hypoplastic and the posterior circulation fed by the ICA through this “fetal PComA,” the incidence of which was found to be 28%.[[6]]
About 2–3 mm from the origin of the PComA, 2–10 branches arise, the largest and most constant of which is the premaxillary artery or the thalamotuberal artery.[[7]],[[8]] These branches almost always arise from the superior medial aspect of the PcomA and courses towards the paramedian perforating substance. Avci and Baskaya confirmed that despite the caliber of the PComA, the number of its perforating branches and their diameter is relatively constant.[[5]]
Anterior choroidal artery
The ACho artery arises from the posterolateral wall of the ICA, almost always lateral to the optic tract. 2–5 mm distal to the PComA [[Figure 1]] and may occasionally arise from the PComA or ICA bifurcation. It usually arises as a single trunk,[[9]] however, duplicate or even multiple ACho artery have been reported in 30% of the cases.[[7]] After originating, the artery crosses the optic tract from lateral to medial direction and courses along the optic tract to reach the lateral margin of the cerebral peduncle. Just anterior to the lateral geniculate body, the ACho artery again crosses the optic tract from medial to lateral direction to enter the crural cistern, where it reaches the choroid plexus of the temporal horn of the lateral ventricle through the choroidal fissure. Rhoton et al.[[9]] stated that the ACho artery terminates in the choroid plexus of the lateral ventricle. However, Erdem et al.[[10]] reported that in 16% of the specimens studied, the plexal segment of the ACho artery passes through the choroid fissure as a single trunk and then divides into the lateral plexal and medial perforating branches within the choroid plexus. This is of clinical importance as occlusion of the artery by surgical or endovascular means after ventricular penetration may carry a significant risk.
The ACho artery gives two segments throughout its course as originally proposed by Rhoton and Goldberg:[[9]],[[11]] The first, cisternal segment arising from origin and ending at the point where the artery reaches to the choroidal fissure (choroidal or plexal point). The second segment, plexal segment, consists of one or more branches, which pass through the choroidal fissure and enter the choroid plexus.[[9]] It may give a few small recurrent perforating branches that exit the temporal lobe through the choroidal fissure to supply the optic tract, the cerebral peduncle, and the thalamus.
The first branch that takes off from the ACho artery in the cisternal segment is the unco-hippocampal branch, which supplies the head of the hippocampus. The other branches are “the superior branches” that pass to the anterior and posterior perforated substances and the optic tract, “the lateral and inferior branches” that pass to the temporal lobe and the uncus, and “the medial branches” that penetrate the cerebral peduncle and lateral geniculate body.[[10]]
The ACho artery supplies the optic tract, lateral geniculate body, posterior limb of the internal capsule, globus pallidus, the origin of the optic radiation, middle one-third of the cerebral peduncle, pyriform cortex, uncus, part of the amygdaloid nucleus, substantia nigra, and ventrolateral nucleus of the thalamus. Occlusion of the ACho artery in the cisternal segment may result in contralateral hemiparesis, hemihypesthesia, homonymous hemianopia, and depressed level of consciousness, whereas its occlusion at the level of choroid fissure may be better tolerated because of rich anastomoses between the ACho artery and the posterior lateral choroidal artery.
Interchangeability of the brain regions supplied by the ACho artery may occur. This is particularly important when considering the internal capsule because if the PComA is small, the ACho artery may take over its area and supply the genu and anterior one-third of the internal capsule. If the ACho artery is small, the PComA may supply the posterior limb of the internal capsule. This type of interchangeability may also occur between the ACho artery and the branches of the posterior cerebral artery that supply the cerebral peduncle, substantia nigra, optic tract and lateral geniculate body. This variability accounts for the unpredictability of the consequences of intended or accidental ACho artery occlusion which might lead to hemiplegia and hemianopsia.
Computational flow dynamics in aneurysms
The natural history of any intracranial aneurysms includes three stages: genesis, enlargement, and rupture. The factors that decide the growth of any aneurysm and its ultimate rupture depends upon two theories: high flow effects and low flow effects. The theory supporting high flow effects lies on the effects of elevation of wall shear stress (WSS), which can cause endothelial injury, further leading to wall remodeling and potential degeneration. Unlike the former, the low flow theory states that low flows within aneurysm precipitates localized stagnation of blood in the dome causing a dysfunction of flow-induced nitric oxide synthase, thus leading to wall degradation secondary to inflammatory processes.[[10]]
The use of image-based computational fluid dynamics (CFDs) techniques helps to assess blood flows in patient-specific geometries. Various studies have focused on the analysis of the hemodynamic environment at locations where cerebral aneurysms commonly form.[[12]],[[13]],[[14]]
Any CFD analysis requires the volumetric knowledge of the fluid traversed (i.e., aneurysm per se including the surrounding vasculature) plus velocity and pressure of the fluid at the boundaries of the aneurysm.[[13]] The factors measured in any CFD are as follows:
-
The hydrostatic pressure at the wall – When high leads water hammer effect over the wall of the vessel
-
Wall sheer vector – Flow direction of the fluid along the vessel or the aneurysm
-
Wall sheer stress – When high leads to increased production of Matrix Metalloproteinases-13 which in turn causes vessel wall damage. When decreased increases Inducible Nitrous oxide synthase production suggesting no induced damage to vessel wall. However, low WSS increases the risk of endothelial proliferation and apoptosis
-
Streamline or Jet of blood stream-shows the flow pattern and causes endothelial cell injury.[[13]]
Methods
Data were collected retrospectively from all patients with incidental IC PC and ACho aneurysms who presented to the Department of Neurosurgery at Fujita Health University, Banbuntane Hotokukai Hospital, Nagoya, Aichi, Japan, from 2014 to 2018.
In the Department of Neurosurgery at Banbuntane Hotokukai Hospital, Nagoya, Japan, the management strategy for ACho artery aneurysms has evolved over time. Initially, surgical clipping was the preferred method for all cases with ACho artery aneurysms, irrespective of whether they are incidental or ruptured. Later, with the invent of endovascular coiling devices, most cases were subjected to the recent procedure instead of open surgery. At present, after the introduction of the Indocyanine Green Video angiography (ICG-VAG) and motor evoked potentials (MEP) to the neurosurgical armamentary, the preferred mode of treatment depends on the preoperative status of individual patient and whether the aneurysm is incidental or ruptured. Endovascular coiling is reserved as the first choice for patients with ruptured AChA aneurysms with poor grade SAH (Hunt and Hess Grades III and IV and/or small neck aneurysm) and with an inappropriate neck-to-dome ratio (<1.5).
A total of 73 patients who underwent surgery for incidental IC PC and ACho artery aneurysms were included in the study. All patients were thoroughly studied with the demographic data and preoperative computed tomography (CT) angiography and three-dimensional (3D) CT angiography.
CFD study for complete preoperative evaluation of the aneurysm and its flow rate was done for all the patients included in the study. The CFD software used was Hemoscope 2 (Ziosoft corporation, Minato Ward, Tokyo, Japan).[[14]]
All the patients underwent surgical clipping electively by a lateral frontotemporobasal transsylvian approach. Perioperatively all the patients were monitored with MEP for an acute change in the velocities during dissection as well as during clipping. Soon after the identification of the aneurysm, intraoperative ICG-VAG was done to identify the vascular anatomy of individual patients, and it was repeated to confirm the patency of the main artery as well as their perforators.
All the patients were examined postoperatively for fresh neurological deficits and evaluated with radiological imaging and angiography. Fresh neurological deficits were defined as new deficits that appeared postoperatively lasting for 24 h or more. Patients who developed fresh neurological deficits were studied in detail and followed up with serial imaging to document transient or permanent brain damage.
Results
Out of a total of 73 patients, most of them belonged to the elderly age group with an average age of 62.4 years. It was predominantly seen in the females (85%) than the males. About 78% of the patients had true IC PC aneurysms, and 14 patients had true ACho artery aneurysms, and there were only two patients with combined IC PC and ACho artery aneurysms [[Figure 2]].

It was commonly observed to be on the left side in about 54% of patients. The average size of the aneurysm was 5.58 mm with a range from 2.5 to 20 mm. The commonest projection of the aneurysm was noted to be posterior followed by the posteromedial group, later followed by the lateral and posterolateral group [[Figure 3]]. ICG-VAG and MEP were done for all patients for identify the arterial anatomy of individual case and for early identification of fresh neurological deficits.

Among the 73 patients duly consented and studied, only 2 patients had postoperative complications in the form of transient hemiparesis, and none had a permanent ACho syndrome. Both the patients belonged to the elderly age group and had right-sided IC PC aneurysms. In these two subjects, the aneurysm sac was found to be either posteriorly or posteromedially and none of the patients who had their aneurysmal sacs projecting in the lateral or posterolateral direction had any postoperative complications.
Both the patients with complications have been discussed below as illustrative cases:
Illustrative case 1
A 72-year-old female who presented with incidental right IC PC aneurysm diagnosed with CT angiography, 3D-CT angiography [[Figure 4]] and CFD studies. The characteristics of the aneurysm were noted according to the CFD were as follows [[Figure 5]]:

– Length of the aneurysm
– 2.6 mmDepth of the aneurysm
– 4.5 mmSurface area of the aneurysm
– 61.2 mm2Volume of the aneurysm
– 48.6 mm3Flow rate within the aneurysm
– 3 ml/minHigh hydrostatic pressure at the wall of the aneurysm 75
– 99 mm HgConvergent wall vectors over the neck of aneurysmLow wall shear stress magnitudeAnd a flow streamline showing a curved pattern with low velocity.
The aneurysm was projecting posterolaterally with a neck measuring about 7 mm. She underwent surgery by lateral frontotemporobasal transsylvian approach. Intraoperatively, the aneurysm was lying close to the ACho, and its perforators and a 9 mm straight clip was applied to the neck after dissecting off the perforators away from the neck of aneurysm. Continuous perioperative MEP monitoring was done, and ICG-VAG was performed before and after application of the aneurysm clip.
However, the patient developed a fresh onset of the left hemiparesis postoperatively. This was further evaluated with a magnetic resonance imaging (MRI) which showed an acute infarct in the posterior limb of the right internal capsule and the globus pallidus [[Figure 6]]. She was managed conservatively for the same and was followed up regularly. The hemiparesis improved over a month and there were no fresh deficits. The patient also had a distal right ACho aneurysm for which she underwent a surgery by anterior interhemispheric approach at a later date.

Illustrative case 2
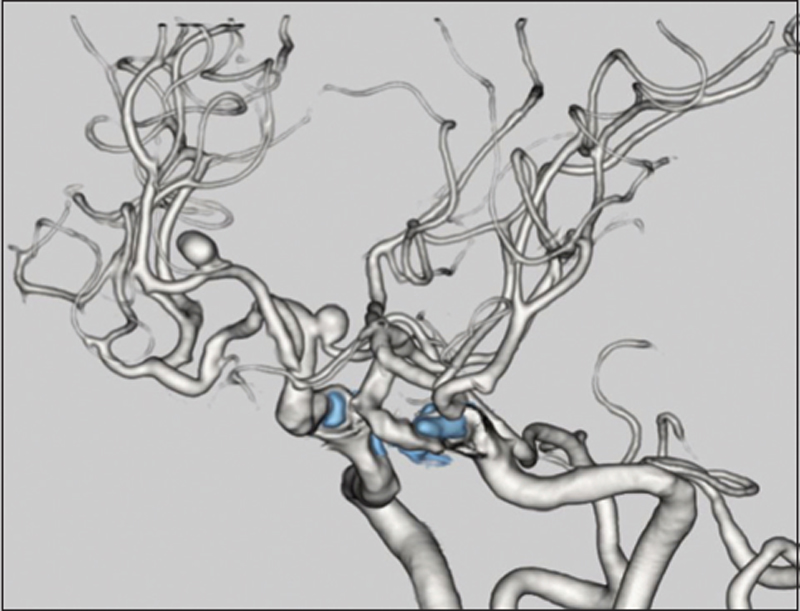
A 64-year-old female diagnosed to have an incidental right-sided IC PC aneurysm, confirmed by CT angiography, 3D-CT angiography [[Figure 7]] and CFD for a complete evaluation of the aneurysm. The results of the CFD are as follows [[Figure 8]]:


– Length of the aneurysm
– 5.6 mmDepth of the aneurysm
– 7.5 mmSurface area of the aneurysm
– 188.1 mm2Volume of the aneurysm
– 280.2 mm3Flow rate within the aneurysm
– 17 ml/min
– High hydrostatic pressure along the length of the aneurysm measuring around 99 mm Hg
– Convergent wall vectors over the neck of aneurysm
– Low wall shear stress magnitude
– And a flow streamline showing a curved pattern with low velocity.
There was a large posteriorly projecting aneurysm arising from the origin of the right PCom A with a neck measuring about 10 mm in size. The patient underwent surgery by a right lateral frontotemporobasal transsylvian approach and an 11 mm straight clip was applied to the neck of aneurysm. The patient was monitored preoperatively with MEP, and an ICG-VAG was performed in the preclipping as well as the postclipping phase.
The patient had an onset of the left hemiparesis in the immediate postoperative period for which an MRI was done. Diffusion-weighted MRI showed an acute infarct in the posterior limb of right internal capsule and right thalamus [[Figure 9]]. She was subjected to extensive physiotherapy and was managed with anticoagulant therapy for the ischemic complication. She showed gradual improvement in her neurological status, and the hemiparesis improved over 2 months with no fresh deficits.

Discussion
Surgery for clipping of incidental IC PC and ACho aneurysms can be catastrophic leading to serious postoperative morbidity in case the identification of the actual individual anatomy is not studied preoperatively and perioperatively. Very few studies mention the ischemic complications associated with the same.[[15]],[[16]],[[17]],[[18]],[[19]],[[20]]
Aoki et al.[[2]] reported a favorable outcome of 79% in the form of no fresh deficits in a retrospective study of 50 patients in Japan who underwent surgical clipping or coiling for incidental IC PC aneurysms.
In 2003, Cha et al.[[21]] from China retrospectively studied 51 patients who underwent surgical clipping for incidental IC PC aneurysms and observed postoperative complications in only six patients and reported a good outcome in 88.3% of their patients.
In a recent study done by Lee and Park[[22]] in South Korea, 62 patients with both incidental and ruptured IC PC aneurysms with variable grades of SAH, who were subjected to surgical clipping were analyzed for their surgical outcomes. They reported an overall good outcome, defined as no fresh deficits, in 95.8% of their patients with only three subjects developing transient Ach Artery syndrome postoperatively.
In this retrospective study, we analyze the outcome of incidental IC PC and ACho artery aneurysms after surgical clipping and emphasis was made on the proper identification of the surgical anatomy and avoidance of permanent postoperative complications. None of the patients in the study suffered a permanent ACho syndrome which is comparable to similar studies conducted elsewhere in Japan, South Korea, and China[[2]],[[22]],[[21]] [[Table 1]].

However, two patients with right IC PC aneurysms had postoperative complications in the form of transient hemiparesis. Both the patients had right-sided true IC PC aneurysms with the sacs projecting posteromedially and posteriorly, respectively. This is a finding observed in all the previously compared studies who confirmed the projection of the aneurysm posteriorly in cases who had postoperative complications.[[2]],[[16]],[[22]],[[21]]
The positive surgical outcome indicated by no fresh postoperative deficits after surgical clipping in the present study was noted to be 97.2% which is comparable to the Chinese study [[Table 2]]. Right-sided IC PC aneurysms carried more risk of developing a postoperative complication due to difficulty in visualizing the ACho artery perioperatively.

The use of perioperative adjuncts such as MEP and ICG-VAG aids in identifying the vascular anatomy at the site of aneurysm thus minimizing inclusion of crucial perforators while clipping the neck of aneurysm.[[2]]
Conclusions
IC PC and ACho artery aneurysms are the most accessible yet most risky to clip surgically due to the high incidence of surgical pitfalls in the form of postoperative ACho syndrome. A thorough preoperative evaluation and careful intraoperative observation for identification of small perforators and fetal Pcom artery helps in avoiding major postoperative complications.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Golshani K, Ferrell A, Zomorodi A, Smith TP, Britz GW. A review of the management of posterior communicating artery aneurysms in the modern era. Surg Neurol Int 2010;1:88.
- 2 Aoki T, Hirohata M, Noguchi K, Komaki S, Orito K, Morioka M, et al. Comparative outcome analysis of anterior choroidal artery aneurysms treated with endovascular coiling or surgical clipping. Surg Neurol Int 2016;7:S504-9.
- 3 Rhoton AL Jr. The supratentorial arteries. Neurosurgery 2002;51:S53-120.
- 4 Gibo H, Lenkey C, Rhoton AL Jr. Microsurgical anatomy of the supraclinoid portion of the internal carotid artery. J Neurosurg 1981;55:560-74.
- 5 Avci E, Baskaya MK. The surgical anatomy of the anomalous posterior communicating artery. In: Watanabe K, Ito Y, Katayama S, Goto H, editors. Proceedings of the 3rd International Mt. Bandai Symposium for Neuroscience and the 4th Pan-Pacific Neurosurgery Congress; 2003. p. 3-10.
- 6 Padget DH. The circle of Willis. Its embryology and anatomy. In: Dandy WE, editor. Intracranial Arterial Aneurysms. Ithaca, NY: Comstock; 1944.
- 7 Yasargil MG. Microneurosurgery. Vol. 1. New York: Thieme- Stratton; 1984.
- 8 Zeal AA, Rhoton AL Jr. Microsurgical anatomy of the posterior cerebral artery. J Neurosurg 1978;48:534-59.
- 9 Rhoton AL Jr., Fujii K, Fradd B. Microsurgical anatomy of the anterior choroidal artery. Surg Neurol 1979;12:171-87.
- 10 Erdem A, Yaşargil G, Roth P. Microsurgical anatomy of the hippocampal arteries. J Neurosurg 1993;79:256-65.
- 11 Goldberg HL. The anterior choroidal artery, Book 2. In: Newton TH, Potts DG, editors. Radiology of the Skull and Brain. Vol. 2. St. Louis: CV. Mosby; 1974.
- 12 Sforza DM, Putman CM, Cebral JR. Computational fluid dynamics in brain aneurysms. Int J Numer Method Biomed Eng 2012;28:801-8.
- 13 Singh PK, Marzo A, Coley SC, Berti G, Bijlenga P, Lawford PV, et al. The role of computational fluid dynamics in the management of unruptured intracranial aneurysms: A clinicians' view. Comput Intell Neurosci 2009;760364.
- 14 Talari S, Kato Y, Shang H, Yamada Y, Yamashiro K, Suyama D, et al. Comparison of computational fluid dynamics findings with intraoperative microscopy findings in unruptured intracranial aneurysms- an initial analysis. Asian J Neurosurg 2016;11:356-60.
- 15 Shi L, Yu J, Zhao Y, Xu K, Yu J. Clipping treatment of posterior communicating artery aneurysms associated with arteriosclerosis and calcification: A single center study of 136 cases. Exp Ther Med 2018;15:1647-53.
- 16 Fukuda H, Hayashi K, Yoshino K, Koyama T, Lo B, Kurosaki Y, et al. Impact of aneurysm projection on intraoperative complications during surgical clipping of ruptured posterior communicating artery aneurysms. Neurosurgery 2016;78:381-90.
- 17 Sharma M, Brown B, Madhugiri V, Cuellar-Saenz H, Sonig A, Ambekar S, et al. Unruptured intracranial aneurysms: Comparison of perioperative complications, discharge disposition, outcome, and effect of calcification, between clipping and coiling: A single institution experience. Neurol India 2013;61:270-6.
- 18 Furtado SV, Venkatesh PK, Hegde AS. Neurological complications and surgical outcome in patients with anterior choroidal segment aneurysms. Int J Neurosci 2010;120:291-7.
- 19 Li J, Mukherjee R, Lan Z, Liu Y, He M. Microneurosurgical management of anterior choroidal artery aneurysms: A 16-year institutional experience of 102 patients. Neurol Res 2012;34:272-80.
- 20 Friedman JA, Pichelmann MA, Piepgras DG, Atkinson JL, Maher CO, Meyer FB, et al. Ischemic complications of surgery for anterior choroidal artery aneurysms. J Neurosurg 2001;94:565-72.
- 21 Cha JH, Park IS, Yi J, Kim KJ, Hwang SH, Han JW. Ischemic complications after surgery for posterior communicating aneurysm. J Korean Neurosurg Soc 2003;33:137-41.
- 22 Lee YS, Park J. Anterior choroidal artery aneurysm surgery: Ischemic complications and clinical outcomes revisited. J Korean Neurosurg Soc 2013;54:86-92.
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
09. September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Golshani K, Ferrell A, Zomorodi A, Smith TP, Britz GW. A review of the management of posterior communicating artery aneurysms in the modern era. Surg Neurol Int 2010;1:88.
- 2 Aoki T, Hirohata M, Noguchi K, Komaki S, Orito K, Morioka M, et al. Comparative outcome analysis of anterior choroidal artery aneurysms treated with endovascular coiling or surgical clipping. Surg Neurol Int 2016;7:S504-9.
- 3 Rhoton AL Jr. The supratentorial arteries. Neurosurgery 2002;51:S53-120.
- 4 Gibo H, Lenkey C, Rhoton AL Jr. Microsurgical anatomy of the supraclinoid portion of the internal carotid artery. J Neurosurg 1981;55:560-74.
- 5 Avci E, Baskaya MK. The surgical anatomy of the anomalous posterior communicating artery. In: Watanabe K, Ito Y, Katayama S, Goto H, editors. Proceedings of the 3rd International Mt. Bandai Symposium for Neuroscience and the 4th Pan-Pacific Neurosurgery Congress; 2003. p. 3-10.
- 6 Padget DH. The circle of Willis. Its embryology and anatomy. In: Dandy WE, editor. Intracranial Arterial Aneurysms. Ithaca, NY: Comstock; 1944.
- 7 Yasargil MG. Microneurosurgery. Vol. 1. New York: Thieme- Stratton; 1984.
- 8 Zeal AA, Rhoton AL Jr. Microsurgical anatomy of the posterior cerebral artery. J Neurosurg 1978;48:534-59.
- 9 Rhoton AL Jr., Fujii K, Fradd B. Microsurgical anatomy of the anterior choroidal artery. Surg Neurol 1979;12:171-87.
- 10 Erdem A, Yaşargil G, Roth P. Microsurgical anatomy of the hippocampal arteries. J Neurosurg 1993;79:256-65.
- 11 Goldberg HL. The anterior choroidal artery, Book 2. In: Newton TH, Potts DG, editors. Radiology of the Skull and Brain. Vol. 2. St. Louis: CV. Mosby; 1974.
- 12 Sforza DM, Putman CM, Cebral JR. Computational fluid dynamics in brain aneurysms. Int J Numer Method Biomed Eng 2012;28:801-8.
- 13 Singh PK, Marzo A, Coley SC, Berti G, Bijlenga P, Lawford PV, et al. The role of computational fluid dynamics in the management of unruptured intracranial aneurysms: A clinicians' view. Comput Intell Neurosci 2009;760364.
- 14 Talari S, Kato Y, Shang H, Yamada Y, Yamashiro K, Suyama D, et al. Comparison of computational fluid dynamics findings with intraoperative microscopy findings in unruptured intracranial aneurysms- an initial analysis. Asian J Neurosurg 2016;11:356-60.
- 15 Shi L, Yu J, Zhao Y, Xu K, Yu J. Clipping treatment of posterior communicating artery aneurysms associated with arteriosclerosis and calcification: A single center study of 136 cases. Exp Ther Med 2018;15:1647-53.
- 16 Fukuda H, Hayashi K, Yoshino K, Koyama T, Lo B, Kurosaki Y, et al. Impact of aneurysm projection on intraoperative complications during surgical clipping of ruptured posterior communicating artery aneurysms. Neurosurgery 2016;78:381-90.
- 17 Sharma M, Brown B, Madhugiri V, Cuellar-Saenz H, Sonig A, Ambekar S, et al. Unruptured intracranial aneurysms: Comparison of perioperative complications, discharge disposition, outcome, and effect of calcification, between clipping and coiling: A single institution experience. Neurol India 2013;61:270-6.
- 18 Furtado SV, Venkatesh PK, Hegde AS. Neurological complications and surgical outcome in patients with anterior choroidal segment aneurysms. Int J Neurosci 2010;120:291-7.
- 19 Li J, Mukherjee R, Lan Z, Liu Y, He M. Microneurosurgical management of anterior choroidal artery aneurysms: A 16-year institutional experience of 102 patients. Neurol Res 2012;34:272-80.
- 20 Friedman JA, Pichelmann MA, Piepgras DG, Atkinson JL, Maher CO, Meyer FB, et al. Ischemic complications of surgery for anterior choroidal artery aneurysms. J Neurosurg 2001;94:565-72.
- 21 Cha JH, Park IS, Yi J, Kim KJ, Hwang SH, Han JW. Ischemic complications after surgery for posterior communicating aneurysm. J Korean Neurosurg Soc 2003;33:137-41.
- 22 Lee YS, Park J. Anterior choroidal artery aneurysm surgery: Ischemic complications and clinical outcomes revisited. J Korean Neurosurg Soc 2013;54:86-92.