

RSS-Feed abonnieren
DOI: 10.4103/ajns.AJNS_130_17
Microsurgical treatment of paraclinoid aneurysms by extradural anterior clinoidectomy: The fujita experience
Authors

Introduction: Paraclinoid aneurysms pose technical difficulty in their approach, mainly because of their close proximity to neurovascular structures, deeper location, and a smaller corridor. Extradural anterior clinoidectomy is a highly beneficial technique in such cases, making more space to deal with these aneurysms. We describe our method of performing extradural anterior clinoidectomy in such patients. Materials and Methods: A total of 33 cases of paraclinoid internal carotid artery aneurysms presenting to Fujita Health University Banbuntane Hospital, Japan, were included. Females comprised the majority with 32 cases; the mean age was 54.8 years (range: 35–74 years). The mean size of the paraclinoid aneurysm was 5.3 mm (range: 3–12 mm). Results: Nine paraclinoid aneurysms were found projecting dorsally, 7 laterally, and 17 medially (Kazuhiko Kyoshim et al's. classification). An immediate complete occlusion rate of 100% was present. Visual disturbance was found in 6.2% of our patients. One of our patients developed permanent loss of vision. Conclusion: Extradural anterior clinoidectomy enables a better exposure to paraclinoid aneurysms. Precise anatomical knowledge along with microsurgical tactics is required to prevent and manage potential complications to achieve good outcomes.
Introduction
The paraclinoid segment of the internal carotid artery (ICA) aneurysms has been named the area from where it exits the cavernous sinus and enters the subarachnoid space to the origin of the posterior communicating artery.[[1]],[[2]],[[3]],[[4]],[[5]] ICA aneurysms present with unique challenges in both diagnosis and microsurgical management because of their unique anatomic location, and these types of aneurysms have been associated with a high morbidity and mortality.[[3]],[[6]],[[7]] Before the development of skull base techniques, the approach for these aneurysms was difficult because the anterior clinoid process (ACP) obstructed the surgical field and restricted the surgeon's working space. The clipping of paraclinoid aneurysms, while attempting to preserve the ophthalmic artery and maintain patency of the ICA, is a technically difficult procedure.
Advances in skull base approaches, especially the extradural anterior clinoidectomy,[[8]],[[9]],[[10]] have greatly improved surgical outcomes for patients with paraclinoid aneurysms. An alternative treatment of paraclinoid aneurysms is endovascular procedure.[[11]],[[12]],[[13]] Microsurgery continues to result in a larger percentage of total occlusions compared to other methods, especially for large and giant aneurysms, because total obliteration with endovascular treatment is not as likely as it is with surgery,[[14]],[[15]] and coiling procedures have been associated with a higher rate of recurrent aneurysms compared with that of surgical treatment.[[16]],[[17]] Although the extradural anterior clinoidectomy was developed specifically to improve outcomes for paraclinoid aneurysms, many authors still report high complication rates resulting from this approach.[[2]],[[3]],[[6]],[[17]]
The purpose of this study was to review our recent experiences using extradural anterior clinoidectomy to surgically clip paraclinoid segment aneurysms.
Materials and Methods
Cerebral aneurysm patients were reviewed between September 2014 and December 2016 at the Banbuntane Hotokukai Hospital, Fujita Health University, Nagoya, Japan. A retrospective analysis of all patients with unruptured paraclinoid ICA aneurysm was performed. Patients' demographic data, site of the aneurysm, operation notes, and postoperative morbidities or mortalities were reviewed and recorded. Institutional ethical clearance and patients' consent for publication were taken. According to our department protocol, all patients diagnosed with unruptured paraclinoid ICA aneurysms who are candidates for treatment are discussed with the neuro-intervention team of our department. If not considered a good candidate for intervention, the patient will be offered surgery. We use reconstructed computed tomography angiography routinely for surgical planning, and in case of any ambiguity, request a digital subtraction angiography. In our hospital, all neurovascular surgeries are performed with OPMI ® Pentero ® Microscope (Carl Zeiss, Oberkochen, Germany) with infra-red 800 camera equipped with FLOW 800 software (Carl Zeiss, Oberkochen, Germany). Upon exposure of aneurysm, we perform indocyanine green-videoangiography to clarify the aneurysm and its relation to all the surrounding vessels. Furthermore, to evaluate any perforating artery or other structures hidden behind the aneurysm, we introduce a rigid endoscope (Machida, Japan) under microscopic guidance. With this technique, we check for the estimated final location of the aneurysm clip tips to be away from any critical structure.
Surgical approach
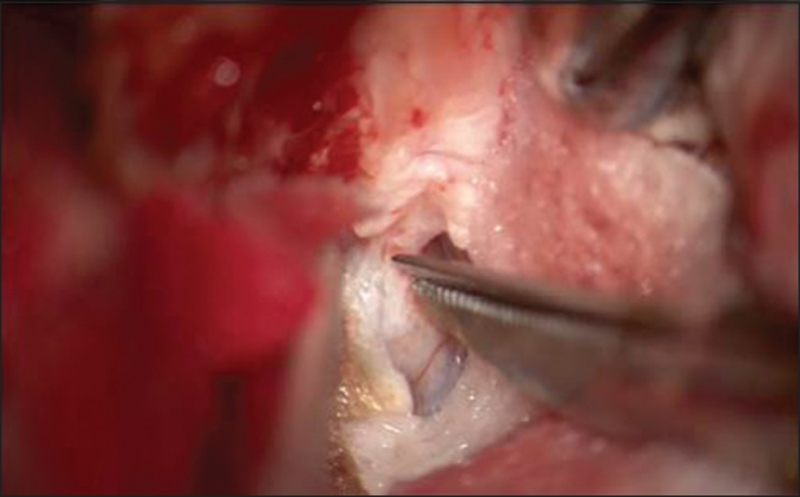
All 33 paraclinoid aneurysms were treated using an ipsilateral pterional approach with an extradural, ACP removal. Head is always rotated by 30° to the contralateral side with slight flexion of the neck to avoid neck vein obstruction from hyperflexion. The level of the head should be higher than the heart to decrease intracranial pressure during surgery. Skin incision is started from the preauricular, zygomatic root area and extends to cover the frontotemporal area and ends at the midline of the frontal area. The temporalis muscle and pericranium layer are dissected with subperiosteal dissection until the zygomatic root is observed. The craniotomy is done with high-speed cutting. The sphenoid ridge is flattened first to make a wide space for exposure. A large rongeur is also used to remove the cortical bone, and then the temporal and frontal dura are elevated from the inner table of the skull by a periosteal elevator or Penfield elevator. The superior orbital fissure and optic nerve are seen at the temporal and frontal sides, respectively. The meningo-orbital band or orbitotemporal periosteal fold is exposed at the temporal side lateral to the ACP. The dural groove is the landmark for the junction of the periorbital and temporal dura. From this point, we start to cut with the blade [[Figure 1]]. The next step is peeling the dura propria to separate it from the temporal side to expose the oculomotor nerve, trochlear nerve, and ophthalmic (V1) branch from the lateral wall of the cavernous sinus. Unroofing of the optic canal is then performed. Following this, removal of ACP using a micro rongeur is done in a piecemeal fashion. The correlation between the direction of the aneurysm and the tip of ACP should be considered because we can punctiliously avoid premature rupture of the aneurysm, especially the medial direction of the aneurysmal dome. Removal of the cortical bone of the ACP allows for improved exposure of the ICA (ophthalmic and clinoid parts), aneurysm, optic nerve, and oculomotor nerve. The distal dural ring is observed and the optic strut is seen in the area of the Dolenc or clinoidal triangle. The bone in this area must be removed with micro-forceps. The dura is incised from the sylvian area for exposure of the sylvian fissure and through the distal part of the ICA. The aim of opening the dura in this step is inspection and confirmation of the location of the aneurysmal sac before the tip of the ACP is removed. An “L-” shaped dural incision was performed along the sylvian fissure and frontal base. The dural incision extended anteriorly over the third cranial nerve and toward the opening of the oculomotor foramen. The distal dural ring was completely or partially released to allow for mobilization of the ICA segment in order to improve access to the aneurysm for clipping [[Figure 2]].

Results
Between September 2014 and December 2016, a total of 93 ICA aneurysms were found. It comprised 37 IC-posterior communicating artery aneurysms (IC-PC), 12 IC-anterior choroidal (IC-Acho), 10 IC top (IC top), 1 IC fusiform, and 33 paraclinoid aneurysms [[Figure 3]].

A total of 33 cases of paraclinoid IC aneurysms were present. Females comprised the majority with 32 cases and only one male in the study. The mean age was 54.8 years, ranging from 35 to 74 years. The mean size of the paraclinoid aneurysm was 5.3 mm (range: 3–12 mm). Paraclinoid aneurysms were classified as per the projection, based on the classification of juxta dural ring aneurysms of ICA by Kyoshima et al. [[Figure 4]].[[18]] Based on it, 9 paraclinoid aneurysms were found projecting dorsally, 7 laterally, and 17 medially. No patient had any other types of vascular malformation [[Figure 5]].


Morbidity
An immediate complete occlusion rate of 100% was achieved in the present series. We noted morbidity in the form of visual disturbances in 6.2% of our patients. One of our patients developed permanent loss of vision. No mortality was seen in our series. No cerebrospinal fluid leakage, unplanned ICA occlusion, and epidural hematoma was seen postoperatively in our patients.
Illustrated case 1
A 68-year-old male with incidental large 12-mm paraclinoid aneurysm was operated by pterional approach and removal of ACP. After cutting the meningo-orbital band, piecemeal removal of ACP and optic strut were performed using a micro rongeur. Dura was divided over distal dural ring to facilitate mobilization of ICA and better exposure of the aneurysm [[Figure 6]]a, [[Figure 6]]b, [[Figure 6]]c. As the aneurysm was a large one, suction decompression method of clipping was used.

Discussion
Various names have been given to the paraclinoid aneurysms, namely, ventral ICA segment [[19]] and the carotid-ophthalmic segment.[[6]],[[20]] These aneurysms are technically challenging because access to the neck of the aneurysm usually requires ACP removal,[[3]],[[6]],[[2]] and their location provides a restricted working space.
Obliteration of the aneurysm with endovascular treatment has a lower success rate for total occlusion.[[14]],[[15]],[[21]] Further, recurrences are more frequent after endovascular treatment, especially in lesions that were incompletely occluded during the initial procedure.[[16]],[[17]] Microsurgery, therefore, remains the primary treatment for paraclinoid segment ICA aneurysms, as it provides a higher long-term success rate,[[17]] although in some cases, combined surgical and endovascular approaches have been a useful treatment strategy.[[1]],[[5]],[[22]]
In 1968, Drake et al.[[23]] reported that only 40% of patients (with 14 paraclinoid aneurysms) achieved good outcomes (Glasgow Outcome Scale score of 4 or 5) following microsurgery, while 60% of patients died. However, subsequent clinical series have shown substantial improvements in outcome. In 1994, Batjer et al.[[2]] reported positive outcomes in 87% of cases from a surgical series of 89 paraclinoid aneurysms, with only a 12% morbidity rate. In 2001, Hoh et al.[[17]] reported that combined surgical and endovascular treatment of paraclinoid aneurysms resulted in good outcomes in 90% of the 145 surgically treated aneurysms. In 2004, Beretta et al.[[24]] reported good outcomes in 81% of the study patients with a 13% morbidity rate. Recently in 2008, Raco et al.[[25]] reported good outcomes in 81% of patients and a long-term morbidity rate of 20%. The current study reports more favorable outcomes with 100% immediate occlusion rates and 6.2% morbidity in terms of visual disturbances, although one patient developed permanent visual loss.
Optic nerve injury is one of the most common complications after surgical treatment of paraclinoid aneurysms. Caution must be exercised when the optic canal is unroofed. The dura overlying the optic canal must not be disrupted. Moreover, the pial vessels of the optic nerve must not be disrupted while the dura is incised. Retraction of the optic nerve must be brief and minimal. Before incising the dura on the distal dural ring and the floor of the optic canal, the ophthalmic artery must be identified to avoid its inadvertent injury. Superior hypophyseal artery occlusion may be accounted as a contributing factor in visual disturbances. The cranial nerve can be injured during ACP removal or clip blade advancement or from excessive retraction or overzealous sinus packing. We experienced transient visual disturbances, which was far lower than other series [[3]],[[17]],[[26]],[[27]] and one case had permanent visual loss. While applying the clip, we were careful to confirm whether the end of clip blade injured a cranial nerve. In order to prevent injury while retracting the temporal lobe, the carotid-oculomotor membrane was opened sharply.
Rizzo [[28]] found two etiologies of worsened vision, including a fulminant orbital syndrome caused by the compromise of large draining veins of the orbit and a retrobulbar optic neuropathy caused either by direct injury or damage to the small dura vessels of the posterior optic nerve. Kumon [[29]] believed that the occurrence of visual disturbances resulted from injury to the ipsilateral optic nerve caused by excessive retraction or by the heat produced by the diamond drill. We did not prefer the use of drill to remove ACP and optic strut. Micro rongeurs were used to remove the ACP piecemeal, which we believe to be a very safe option. Recently, use of ultrasonic bone cutter has also been introduced. The use of this device does not automatically protect the soft tissues and the angle of the tip and the optic canal should be as close to perpendicular as possible.
Hemostasis is a cause of major concern when the outer layer of the lateral dural wall of the cavernous sinus is peeled off to expose the inner layer of deepest inferolateral surface of ACP. Bleeding from the cavernous sinus should be distinguished from bleeding from the dural draining vein, as the former can be well controlled with gentle packing with hemostatic agents (packing appears as “cones” made by the hemostatic agent, while the latter requires bipolar coagulation). Overzealous sinus packing must be avoided owing to potential compressive injuries to the cranial nerves.
Conclusion
The surgical treatment of aneurysms that arise from the paraclinoid segment of the ICA has been a technical challenge for cerebrovascular surgeons. The authors have tried to avoid several complications in extradural anterior clinoidectomy approach to paraclinoid aneurysms using several tactics. Micro scissors were used parallel to the ACP in order to avoid injuring the cranial nerves. The ACP was rongeured instead of drilling in order to minimize any thermal injury to the optic nerve. Precise anatomical knowledge combined with these microsurgical tactics is required to prevent and manage potential complications to achieve good outcomes.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Arnautović KI, Al-Mefty O, Angtuaco E. A combined microsurgical skull-base and endovascular approach to giant and large paraclinoid aneurysms. Surg Neurol 1998;50:504-18.
- 2 Batjer HH, Kopitnik TA, Giller CA, Samson DS. Surgery for paraclinoidal carotid artery aneurysms. J Neurosurg 1994;80:650-8.
- 3 De Jesús O, Sekhar LN, Riedel CJ. Clinoid and paraclinoid aneurysms: Surgical anatomy, operative techniques, and outcome. Surg Neurol 1999;51:477-87.
- 4 Kattner KA, Bailes J, Fukushima T. Direct surgical management of large bulbous and giant aneurysms involving the paraclinoid segment of the internal carotid artery: Report of 29 cases. Surg Neurol 1998;49:471-80.
- 5 Mizoi K, Takahashi A, Yoshimoto T, Fujiwara S, Koshu K. Combined endovascular and neurosurgical approach for paraclinoid internal carotid artery aneurysms. Neurosurgery 1993;33:986-92.
- 6 Dolenc VV. A combined transorbital-transclinoid and transsylvian approach to carotid-ophthalmic aneurysms without retraction of the brain. Acta Neurochir Suppl 1999;72:89-97.
- 7 Tanaka Y, Hongo K, Tada T, Nagashima H, Horiuchi T, Goto T, et al. Radiometric analysis of paraclinoid carotid artery aneurysms. J Neurosurg 2002;96:649-53.
- 8 Coscarella E, Başkaya MK, Morcos JJ. An alternative extradural exposure to the anterior clinoid process: The superior orbital fissure as a surgical corridor. Neurosurgery 2003;53:162-6.
- 9 Froelich SC, Aziz KM, Levine NB, Theodosopoulos PV, van Loveren HR, Keller JT, et al. Refinement of the extradural anterior clinoidectomy: Surgical anatomy of the orbitotemporal periosteal fold. Neurosurgery 2007;61:179-85.
- 10 Krisht AF. Transcavernous approach to diseases of the anterior upper third of the posterior fossa. Neurosurg Focus 2005;19:E2.
- 11 Gurian JH, Viñuela F, Guglielmi G, Gobin YP, Duckwiler GR. Endovascular embolization of superior hypophyseal artery aneurysms. Neurosurgery 1996;39:1150-4.
- 12 Lanzino G, Wakhloo AK, Fessler RD, Hartney ML, Guterman LR, Hopkins LN, et al. Efficacy and current limitations of intravascular stents for intracranial internal carotid, vertebral, and basilar artery aneurysms. J Neurosurg 1999;91:538-46.
- 13 Park HK, Horowitz M, Jungreis C, Kassam A, Koebbe C, Genevro J, et al. Endovascular treatment of paraclinoid aneurysms: Experience with 73 patients. Neurosurgery 2003;53:14-23.
- 14 Fernandez Zubillaga A, Guglielmi G, Viñuela F, Duckwiler GR. Endovascular occlusion of intracranial aneurysms with electrically detachable coils: Correlation of aneurysm neck size and treatment results. AJNR Am J Neuroradiol 1994;15:815-20.
- 15 Hope JK, Byrne JV, Molyneux AJ. Factors influencing successful angiographic occlusion of aneurysms treated by coil embolization. AJNR Am J Neuroradiol 1999;20:391-9.
- 16 Boet R, Wong GK, Poon WS, Lam JM, Yu SC. Aneurysm recurrence after treatment of paraclinoid/ophthalmic segment aneurysms – A treatment-modality assessment. Acta Neurochir (Wien) 2005;147:611-6.
- 17 Hoh BL, Carter BS, Budzik RF, Putman CM, Ogilvy CS. Results after surgical and endovascular treatment of paraclinoid aneurysms by a combined neurovascular team. Neurosurgery 2001;48:78-89.
- 18 Kyoshima K, Oikawa S, Koike G, Hokama M, Toriyama T, Gibo H, et al. A classification of juxta-dural ring aneurysms of internal carotid artery. Surg Cereb Stroke 1997;25:370-7.
- 19 Fox JL. Microsurgical treatment of ventral (paraclinoid) internal carotid artery aneurysms. Neurosurgery 1988;22:32-9.
- 20 Dolenc VV. A combined epi- and subdural direct approach to carotid-ophthalmic artery aneurysms. J Neurosurg 1985;62:667-72.
- 21 Viñuela F, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: Perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475-82.
- 22 Jin SC, Kwon DH, Song Y, Kim HJ, Ahn JS, Kwun BD, et al. Multimodal treatment for complex intracranial aneurysms: Clinical research. J Korean Neurosurg Soc 2008;44:314-9.
- 23 Drake CG, Vanderlinden RG, Amacher AL. Carotid-ophthalmic aneurysms. J Neurosurg 1968;29:24-31.
- 24 Beretta F, Andaluz N, Zuccarello M. Aneurysms of the ophthalmic (C6) segment of the internal carotid artery: Treatment options and strategies based on a clinical series. J Neurosurg Sci 2004;48:149-56.
- 25 Raco A, Frati A, Santoro A, Vangelista T, Salvati M, Delfini R, et al. Long-term surgical results with aneurysms involving the ophthalmic segment of the carotid artery. J Neurosurg 2008;108:1200-10.
- 26 Cawley CM, Zipfel GJ, Day AL. Surgical treatment of paraclinoid and ophthalmic aneurysms. Neurosurg Clin N Am 1998;9:765-83.
- 27 Xu BN, Sun ZH, Jiang JL, Wu C, Zhou DB, Yu XG, et al. Surgical management of large and giant intracavernous and paraclinoid aneurysms. Chin Med J (Engl) 2008;121:1061-4.
- 28 Rizzo JF 3rd. Visual loss after neurosurgical repair of paraclinoid aneurysms. Ophthalmology 1995;102:905-10.
- 29 Kumon Y, Sakaki S, Kohno K, Ohta S, Ohue S, Oka Y, et al. Asymptomatic, unruptured carotid-ophthalmic artery aneurysms: Angiographical differentiation of each type, operative results, and indications. Surg Neurol 1997;48:465-72.
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
09. September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Arnautović KI, Al-Mefty O, Angtuaco E. A combined microsurgical skull-base and endovascular approach to giant and large paraclinoid aneurysms. Surg Neurol 1998;50:504-18.
- 2 Batjer HH, Kopitnik TA, Giller CA, Samson DS. Surgery for paraclinoidal carotid artery aneurysms. J Neurosurg 1994;80:650-8.
- 3 De Jesús O, Sekhar LN, Riedel CJ. Clinoid and paraclinoid aneurysms: Surgical anatomy, operative techniques, and outcome. Surg Neurol 1999;51:477-87.
- 4 Kattner KA, Bailes J, Fukushima T. Direct surgical management of large bulbous and giant aneurysms involving the paraclinoid segment of the internal carotid artery: Report of 29 cases. Surg Neurol 1998;49:471-80.
- 5 Mizoi K, Takahashi A, Yoshimoto T, Fujiwara S, Koshu K. Combined endovascular and neurosurgical approach for paraclinoid internal carotid artery aneurysms. Neurosurgery 1993;33:986-92.
- 6 Dolenc VV. A combined transorbital-transclinoid and transsylvian approach to carotid-ophthalmic aneurysms without retraction of the brain. Acta Neurochir Suppl 1999;72:89-97.
- 7 Tanaka Y, Hongo K, Tada T, Nagashima H, Horiuchi T, Goto T, et al. Radiometric analysis of paraclinoid carotid artery aneurysms. J Neurosurg 2002;96:649-53.
- 8 Coscarella E, Başkaya MK, Morcos JJ. An alternative extradural exposure to the anterior clinoid process: The superior orbital fissure as a surgical corridor. Neurosurgery 2003;53:162-6.
- 9 Froelich SC, Aziz KM, Levine NB, Theodosopoulos PV, van Loveren HR, Keller JT, et al. Refinement of the extradural anterior clinoidectomy: Surgical anatomy of the orbitotemporal periosteal fold. Neurosurgery 2007;61:179-85.
- 10 Krisht AF. Transcavernous approach to diseases of the anterior upper third of the posterior fossa. Neurosurg Focus 2005;19:E2.
- 11 Gurian JH, Viñuela F, Guglielmi G, Gobin YP, Duckwiler GR. Endovascular embolization of superior hypophyseal artery aneurysms. Neurosurgery 1996;39:1150-4.
- 12 Lanzino G, Wakhloo AK, Fessler RD, Hartney ML, Guterman LR, Hopkins LN, et al. Efficacy and current limitations of intravascular stents for intracranial internal carotid, vertebral, and basilar artery aneurysms. J Neurosurg 1999;91:538-46.
- 13 Park HK, Horowitz M, Jungreis C, Kassam A, Koebbe C, Genevro J, et al. Endovascular treatment of paraclinoid aneurysms: Experience with 73 patients. Neurosurgery 2003;53:14-23.
- 14 Fernandez Zubillaga A, Guglielmi G, Viñuela F, Duckwiler GR. Endovascular occlusion of intracranial aneurysms with electrically detachable coils: Correlation of aneurysm neck size and treatment results. AJNR Am J Neuroradiol 1994;15:815-20.
- 15 Hope JK, Byrne JV, Molyneux AJ. Factors influencing successful angiographic occlusion of aneurysms treated by coil embolization. AJNR Am J Neuroradiol 1999;20:391-9.
- 16 Boet R, Wong GK, Poon WS, Lam JM, Yu SC. Aneurysm recurrence after treatment of paraclinoid/ophthalmic segment aneurysms – A treatment-modality assessment. Acta Neurochir (Wien) 2005;147:611-6.
- 17 Hoh BL, Carter BS, Budzik RF, Putman CM, Ogilvy CS. Results after surgical and endovascular treatment of paraclinoid aneurysms by a combined neurovascular team. Neurosurgery 2001;48:78-89.
- 18 Kyoshima K, Oikawa S, Koike G, Hokama M, Toriyama T, Gibo H, et al. A classification of juxta-dural ring aneurysms of internal carotid artery. Surg Cereb Stroke 1997;25:370-7.
- 19 Fox JL. Microsurgical treatment of ventral (paraclinoid) internal carotid artery aneurysms. Neurosurgery 1988;22:32-9.
- 20 Dolenc VV. A combined epi- and subdural direct approach to carotid-ophthalmic artery aneurysms. J Neurosurg 1985;62:667-72.
- 21 Viñuela F, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: Perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475-82.
- 22 Jin SC, Kwon DH, Song Y, Kim HJ, Ahn JS, Kwun BD, et al. Multimodal treatment for complex intracranial aneurysms: Clinical research. J Korean Neurosurg Soc 2008;44:314-9.
- 23 Drake CG, Vanderlinden RG, Amacher AL. Carotid-ophthalmic aneurysms. J Neurosurg 1968;29:24-31.
- 24 Beretta F, Andaluz N, Zuccarello M. Aneurysms of the ophthalmic (C6) segment of the internal carotid artery: Treatment options and strategies based on a clinical series. J Neurosurg Sci 2004;48:149-56.
- 25 Raco A, Frati A, Santoro A, Vangelista T, Salvati M, Delfini R, et al. Long-term surgical results with aneurysms involving the ophthalmic segment of the carotid artery. J Neurosurg 2008;108:1200-10.
- 26 Cawley CM, Zipfel GJ, Day AL. Surgical treatment of paraclinoid and ophthalmic aneurysms. Neurosurg Clin N Am 1998;9:765-83.
- 27 Xu BN, Sun ZH, Jiang JL, Wu C, Zhou DB, Yu XG, et al. Surgical management of large and giant intracavernous and paraclinoid aneurysms. Chin Med J (Engl) 2008;121:1061-4.
- 28 Rizzo JF 3rd. Visual loss after neurosurgical repair of paraclinoid aneurysms. Ophthalmology 1995;102:905-10.
- 29 Kumon Y, Sakaki S, Kohno K, Ohta S, Ohue S, Oka Y, et al. Asymptomatic, unruptured carotid-ophthalmic artery aneurysms: Angiographical differentiation of each type, operative results, and indications. Surg Neurol 1997;48:465-72.