

Subscribe to RSS
DOI: 10.3766/jaaa.19014
Access to Hearing Health Care, Geographical Residency, and Quality of Life in Adults with and without Hearing Loss
Authors

Abstract
Background There is an increased interest in the impact that hearing loss has on general well-being, including overall quality of life (QOL), to improve and expand care that is provided to individuals with hearing loss.
Purpose To evaluate QOL in adults with and without access to hearing health care (HHC).
Research Design A cross-sectional study examined QOL across groups of individuals with and without hearing loss.
Study Sample One hundred eight participants from West Central and South Alabama received pure-tone hearing evaluations. Thirty-two adults had hearing within normal limits and 76 had at least a mild hearing loss in one ear.
Data Collection and Analysis The Quality of Life Inventory (QOLI), the Charlson Comorbidity Index, and an Accessibility to Health Care questionnaire were administered to all participants. The QOLI outcomes were used as the dependent variable for the analysis of covariance (ANCOVA) statistical procedures.
Results For adults with hearing loss who did not have access to HHC, lower QOL scores were reported compared with those with access to HHC, but this finding was not significant. Although ANCOVA results did not suggest QOL differences across geographical regions, effect size calculations indicated that adults with hearing loss who lived in the most rural regions of Alabama had lower reported QOL scores than their counterparts who had hearing within normal limits. Finally, those with higher incomes, who were older, and who had fewer physical disorders reported higher QOL than those with lower incomes, who were younger, and who had more physical ailments.
Conclusions Adults with hearing loss who live in regions without access to HHC might be at risk for decreased QOL. A number of models for improving access to HHC will be necessary to decrease this potential risk.
Introduction
Recently, there has been an increase in the assessment of general well-being or quality of life (QOL) in adults with hearing loss (Nordvik et al[23]). In fact, the first of twelve goals outlined in ‘‘Hearing Health Care for Adults: Priorities for Improving Access and Affordability” by the Committee on Accessible and Affordable Hearing Health Care for Adults is to conduct studies that examine the impact of hearing loss and its treatment on QOL, in diverse and underserved populations (National Academies of Sciences Engineering Medicine[21]). A broader understanding of the impact hearing loss has on general well-being will ultimately lead to improvements in the care provided to individuals with hearing loss. To begin to address these issues, we conducted a preliminary study that explored how hearing loss impacts general QOL, in addition to examining how accessibility to hearing health care (HHC) and geographical residence influenced the outcomes.
Previous studies examining general QOL in the presence of hearing loss have generated mixed results (Chia et al;[6] Chew and Yeak;[5] Mondelli and de Souza[20]). General QOL has broadly been defined by the World Health Organization as ‘‘an individual's perception of their position in life'' in the context of their culture and value system (World Health Organization[31]). Some studies have suggested that hearing loss is associated with decreased QOL, whereas others have suggested that hearing loss does not affect QOL (Dalton et al;[9] Helvik et al[14]). Nordvik et al[23] in their review of 13 articles addressing QOL in adults with hearing loss found that two studies demonstrated a significant association between hearing loss and QOL, six found a weak association, and five showed no association at all. Findings generally suggested poorer QOL for older adults with hearing loss than younger adults with hearing loss. Although this review article addressed other intrinsic factors that could lead to decreased QOL such as anxiety and depression, external factors such as geographical residency or access to HHC were not addressed.
Outcomes have demonstrated that for adults living in rural areas, poor health-related QOL does not necessarily occur for all (Farquhar;[11] Cleary and Howell;[7] Howell and Cleary[15]). Generally, older adults reported that if they had a degree of autonomy and social support networks to rely on in their rural communities, they could live very satisfying lives (Farquhar;[11] Cleary and Howell[7]). However, if adults reported that they were physically inactive, poor QOL could result (Hart[13]).
A number of studies have also demonstrated that low income can affect health-related QOL (Robert et al;[27] Lemos et al;[18] Lamu and Olsen;[17] Ward et al[30]). These population-based studies used a number of measures for health-related QOL and generally found that poor health had a significant impact on QOL. Furthermore, for those with poor health and low household income, they reported poorer health-related QOL than those with higher incomes.
For this study, we assessed how overall QOL was affected by access to HHC, and additionally, how specific contextual and individual characteristics affected the outcomes. We explored how access to hearing health care and geographical residency (i.e., contextual characteristics) and individual characteristics, including general health, age, income, and race affected a measure of overall QOL. Our specific questions included the following.
-
Does access to hearing health care affect QOL?
-
Does geographical residency affect QOL?
-
Can individual factors such as general health, age, income, and race help explain the outcomes associated with QOL?
This study, preliminary in nature, will provide data to our ongoing projects that focus on understanding the needs of those living with hearing loss in the rural regions of Alabama. It is hoped that these efforts will help improve access to and affordability of HHC for these individuals.
Methods
Participants
One hundred eight study participants, 79 females and 29 males, were recruited for this study. They consented to participate in this study based on the Internal Review Board guidelines of the University of Alabama. The mean age of the adults was 60 years old with a range of 20–89 years. Residency of study participants was determined using the Rural-Urban Continuum Codes (RUCC) from the United States Department of Agriculture (USDA), Economic Research Service (USDA[28]). These nine codes and their definitions are provided in [Table 1]. This classification scheme distinguishes counties by the degree of urbanization and their adjacency to metro areas. There are three metropolitan codes and six non-metropolitan codes. Four codes were used for classification of the 108 study participants and are provided in [Table 2]. Other demographic information including income, race, and gender also is included in [Table 2].
Note: Fourteen people did not provide income information, 21 adults who completed the accessibility questionnaire did not have hearing loss and were not included in the accessibility to hearing health care data, 29 adults did not complete the accessibility questionnaire, one adult completed the accessibility questionnaire but did not answer the questions related to access to HHC.
Materials
Three questionnaires were used to obtain data, the Quality of Life Inventory (QOLI) (Frisch[12]), the Charlson Comorbidity Index (Charlson et al[4]), and an Accessibility to Health Care questionnaire developed in-house and based on guidelines from the Department of Health and Human Services (DHHS) (DHHS[10]), Penchansky and Thomas[24] and the Access to Care Section from the Agency for Healthcare Research and Quality (AHRQ) (AHRQ[1]).
QOLI
The QOLI (Frisch[12]) is a measure of life satisfaction that includes sixteen aspects of life, including love, health, friends, and community to name a few. For each area, participants were asked to rate how important the item was on a scale from 0 (not important) to 2 (extremely important). Participants also rated how satisfied they were with each life domain on a scale from −3 (very dissatisfied) to +3 (very satisfied). A raw score was obtained and used to derive a percentile and a T-score. T-scores for very low QOL range from 0 to 36, for low QOL range from 37 to 42, for average QOL range from 43 to 57, and for high QOL range from 58 to 77.
This measure was chosen because it has been used widely in clinical psychology for assessments of social interaction anxiety and for the assessments of feelings of hope and optimism, among others (Lindner et al[19]). Current research in hearing loss has suggested that this sensory decline affects emotional well-being (Pronk et al[25]) and consequently, the use of a QOL measure commonly used in clinical psychology settings is warranted.
Charlson Comorbidity Index
General health was assessed using the Charlson Comorbidity Index (Charlson et al[4]). Serious health conditions were tracked with this questionnaire, such as heart disease, cancer, liver disease, kidney disorders, ulcers, and diabetes. With this screener, points were assigned for 19 different diseases (e.g., 1 point for congestive heart failure and 6 points for liver disease). A ten-year probability mortality score (Charlson 10) was calculated from the total points and subsequently used in our statistical analyses. A higher probability score indicated better life expectancy over a ten-year period.
Accessibility to Routine and Hearing Health Care
A Health Care Accessibility Questionnaire was developed in-house to determine accessibility to medical and hearing health care based on guidelines from DHHS[10] and Penchansky and Thomas[24] (See Appendix). Specifically, we developed questions based on availability, accessibility, affordability, and acceptability of access to health care professionals, family physicians (FPs), otolaryngologists, and audiologists. Our criteria for inaccessible FP health care was a travel time of >30 minutes to routine and urgent care facilities. Our criteria for inaccessible hearing health care was a travel time of >60 minutes to an otolaryngologist or an audiologist. In addition, we classified someone as not having access to FP care or hearing health care if because of personal factors, including affordability and acceptability of health care, the participant was not able to access health care, or chose not to access health care. Study participants were classified as having access to both general health care and HHC. The number of participants in each accessibility category is provided in [Table 2].
For our accessibility questionnaire, seventeen questions were created using sample questions from the Medical Expenditure Panel Survey Access to Care Section from AHRQ.[1] Participants responded to the questions using provided options, including travel time selections and reasons for not accessing care such as ‘‘don't know where to go for care,'' ‘‘no health insurance,'' or ‘‘can't afford care for my hearing loss,'' to name a few.
Procedures
Study participants were recruited from four metropolitan and non-metropolitan regions in West Central and South Alabama. The number of participants from each geographical region is provided in [Table 2]. Participants completed a demographic form, which asked questions related to race, ethnicity, income, and hearing aid use.
Before conducting the hearing evaluation, participants were asked about their general physical health using the Charlson Comorbidity Index. Pure-tone air- and bone conduction thresholds were obtained in a sound booth of the Hear Here Alabama mobile audiology clinic (hearing.ua.edu) in each community setting. Thresholds were obtained using the Carhart and Jerger[3] modification of the Hughson and Westlake[16] ascending/descending technique. Insert earphones (3M Auditory Systems EAR Tone 3A insert earphones, Indianapolis, IN), a mastoid-placed bone transducer, and an Otometrics Madsen Astera audiometer (Audiology Systems, Schaumburg, IL) were used to conduct behavioral threshold testing in the sound booth. Bilateral air conduction thresholds were obtained at 250, 500, 1000, 2000, 4000, and 8000 Hz, and bilateral bone conduction thresholds were obtained at 250, 500, 1000, 2000, and 4000 Hz. Six-frequency pure-tone averages (6F-PTA) were calculated for each ear and used for statistical analyses. Following the administration of the hearing evaluation, the QOLI was completed.
Statistical Analyses
Analysis of covariance (ANCOVA) statistical procedures were conducted using QOLI T-score as the dependent variable. A Shapiro-Wilk normality test revealed that the QOLI T-scores, rather than the QOLI percentile scores, were normally distributed and consequently used as the dependent variable in the statistical model. Accessibility to HHC, age, better hearing ear, outcomes from the Charlson Comorbidity Index, residential region, income, and race were used as independent variables. The following equation was used for the ANCOVA:
QOLI T Score = β 0 + β 1 × AccessHearingHealth + β 2 × Age + β 2 × BetterHearingEar + β 4
× Charlson 10 + β 5 × ResidentialRegion + β 6
× Income + β 7 × Race,
where AccessHearingHealth was access to HHC for adults with hearing loss (‘‘yes,'' ‘‘no,'' and ‘‘not applicable''); BetterHearingEar was the 6F-PTA of the better hearing ear; Charlson10 is the ten-year mortality rate calculated from the Charlson Comorbidity Index; ResidentialRegion was the RUCC (‘‘Metro 3,'' ‘‘Non-Metro 7,'' ‘‘Non-Metro 8,'' and ‘‘Non-Metro 9''); income is the household income levels (‘‘< $30,000,'' ‘‘$30,000–49,999,'' ‘‘$50,000-$74,999," ‘‘$75,000-$99,000,'' ‘‘ > $100,000,'' and ‘‘Would prefer not to provide this information''); and race was the participants' racial status (‘‘White,'' ‘‘Black,'' or “African American''). A variance inflation factor analysis revealed that multi-collinearity was not introduced into the analyses.
Results
Thirty-two adults had hearing within normal limits (i.e., 6F-PTA <25 dB at both ears) and 76 had 6F-PTA >25 dB at one ear or both ears. Sixteen adults with hearing loss used at least one hearing aid. Seven adults with hearing loss had a conductive component to their loss where the bone conduction thresholds were ≥ 15 dB better than the air conduction thresholds bilaterally for one or more pure tones. Of the 27 people who reported on our Accessibility Questionnaire that they did not think they had a hearing loss, 14 of them did have hearing loss. Eleven of these 14 participants had a bilateral mild hearing loss and three of them had a mild hearing loss in one ear and a moderate hearing loss in the opposite ear. We also examined individual responses on the accessibility questionnaire related to HHC. Twenty-four people reported that they thought they had a hearing loss but did not access HHC. The reasons for not accessing HHC were ‘‘can't afford care for my hearing loss'' (N = 9), ‘‘insurance doesn't cover HHC'' (N = 5), ‘‘don't know a professional who can provide hearing health care'' (N = 3), and ‘‘other'' (N = 7). Those who reported ‘‘other'' reasons for not accessing hearing health care stated that they believed their hearing loss was only a minor problem and did not need hearing aids or because of “procrastination.” Note that an additional 16 participants with hearing loss were classified as not having access to HHC because they lived >60 minutes by car from a professional. All participants with hearing loss who did not see an otolaryngologist or an audiologist were provided with a list of resources. These resources, however, ranged from a 30-minute to two-hour drive away from their homes.
Right- and left-ear audiograms for the 76 participants with hearing loss are provided in [Figure 1]. The solid line shows the mean thresholds for the left ear at each tested frequency and the dashed line shows the mean thresholds for the right ear. The means 6F-PTA for the left and right ears were 43.2 and 42.8 dB HL, respectively. Very few participants had hearing loss that ranged from moderate to severe or profound. Most hearing losses ranged from mild to moderate.

Box plots of the QOLI T-scores for participants and their place of residency are provided in [Figure 2]. Four residential areas are represented, Metro 3, Non-Metro 7, Non-Metro 8, and Non-Metro 9. The top and bottom panels show the data for adults with hearing loss and adults who had hearing within normal limits, respectively. The number of participants representing each residential region are shown in the plots. The mean QOLI T-scores obtained from participants living in the four different regional settings are provided in [Table 3]. In addition, considering that 73% of our study population was female, a one-way ANOVA was conducted using the QOLI T-scores and gender as a variable to determine if there were differences in reporting QOL between males and females. For this analysis, no significant differences in QOLI T-scores was found (F = 0.64, df = 1, p = 0.42).

For the ANCOVA analyses, although no significant findings for geographical residency were found, effect size calculations suggested medium to large effect sizes when comparing those with and without hearing loss for the four different residential regions. Hedges' g effect sizes comparing the QOLI T-scores for adults with and without hearing loss are provided in [Table 3]. Effect sizes range from 0.33 to 0.67, with three of the four comparisons showing medium effect sizes (i.e., ≥0.5). Generally, trends indicated that adults who had hearing within normal limits reported higher QOL if they lived in more rural regions (i.e., Non-Metro 7, 8, and 9) than the QOL reported for adults living in the Metro 3 region. The opposite trend was found for adults with hearing loss, that is, for adults with hearing loss, the mean QOLI T-scores were poorer for adults who lived in Non-Metro 7, 8, and 9 regions than adults with hearing loss who lived in Metro 3 region.
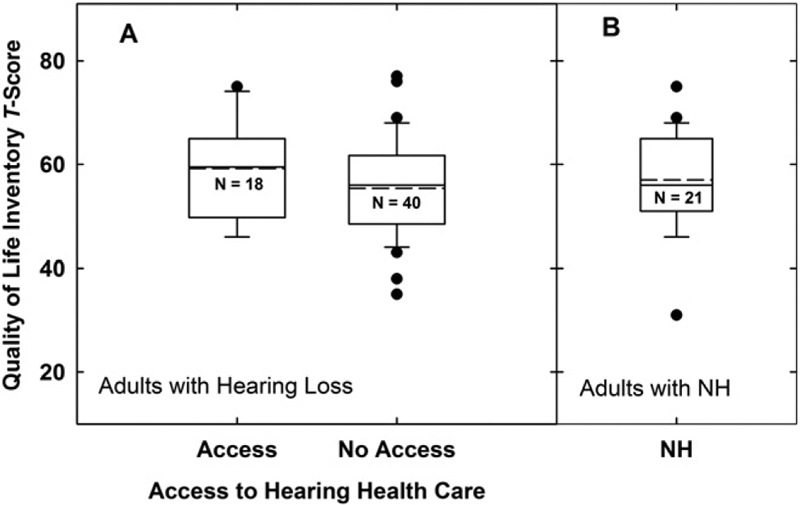
Panel A of [Figure 3] shows the QOLI T-scores for adults with hearing loss who did and did not have access to HHC and Panel B shows the T-scores for adults who had hearing within normal limits. Forty adults with hearing loss did not have access to HHC and eighteen adults did have access. The mean QOLI T-score for adults without access was 55.4 (i.e., average QOL) and for those with access, it was 59.2 (i.e., high QOL). ANCOVA analyses approached but did not reach significance for the differences in QOLI T-scores for those with and without access to HHC (F = 2.59, df = 2, p = 0.08, power = 0.5). A pairwise comparison between adults without access and those with hearing within normal limits approached but did not reach significance (t = −2.3, p = 0.07).
The scatter plots of [Figure 4] display the degree of hearing loss (6F-PTA in dB HL) and QOL outcomes for adults with and without access to HHC and an FP. Panel A displays data for adults who had access to an FP but did not have access to HHC. Panel B shows data for adults who did not have access to an FP or to HHC. Not shown in this figure are the data from the eighteen adults with hearing loss who had access to hearing health care. Also provided in [Figure 4] are the Pearson coefficients and p-values. Overall, there is no apparent correlation between degree of hearing loss and access to HHC or an FP.

In addition to examining the effect of access to HHC and residency on QOL measures, other variables, including age, the presence of other diseases (Charlson 10), income, and race were examined. These outcomes are provided in [Table 4]. Significant outcomes were found for age, race, and income. Although the findings from the Charlson 10 were close to being significant, they were not found to have significantly affected the outcomes (F = 3.77, df = 1, p = 0.06). The results from this index suggested that those with more physical health ailments had poorer QOL (t = 1.94, p = 0.06). Closer examination of 27 adults with Charlson scores ≤0.53 (i.e., a 53% chance of living another ten years) revealed that they all had hearing loss. Only three of them did not have access to an FP and 11 of them did not have access to HHC. They had multiple comorbidities, including cardiovascular, cerebrovascular, cancer, or kidney issues. These physical health issues in combination with advancing age resulted in low Charlson 10 probability scores. Surprising though, these 27 adults with poor physical health all reported average to high QOL. Other statistical outcomes indicated better QOL for increasing age (t = 2.88, p < 0.01) and for household income. That is, adults who reported yearly household income between $50,000 and $74,999 (t = 3.37, p = 0.001) or >$100,000 (t = 4.67, p < 0.001) reported better QOL than those who reported yearly household income than $30,000. Race also was found to be a significant variable with Black or African Americans (N = 47) reporting higher QOL than white participants (N = 59) (t = −2.19, p = 0.03).
Note: Charlson 10 is the ten-year mortality rate from the Charlson, Comorbidity Index. An asterisk indicates significant findings.
Discussion
The goals of this study were to determine how access to HHC and geographical residency affected outcomes on a general QOL questionnaire. Although significant findings related to QOL and residency were not found, the trend was that adults with hearing loss living in more rural areas of the state (i.e., Non-Metro regions 7, 8, and 9) reported poorer QOL than those with hearing loss who lived in a metro region of the state (i.e., Metro 3). In addition, those with hearing loss who did not have access to HHC reported poorer QOL than those with hearing loss who did have access to HHC. Again, this finding approached, but did not reach significance. Other findings were that income and age affected reported QOL. That is, those with higher incomes and increasing age reported higher QOL than those with lower incomes and younger age. In addition, although only approaching significance, those who had more physical conditions reported poorer QOL than those with fewer physical disorders.
Access to HHC, Geographical Residency, and Quality of Life
Similar to the studies demonstrating that hearing loss can affect QOL, our findings have suggested that overall QOL can be affected in those with limited access to HHC and for those living in communities with populations <2,500 (Dalton et al;[9] Helvik et al;[14] Nordvik et al[23]). However, to our knowledge, these findings are the first suggesting that QOL for adults with hearing loss is affected in the presence of limited access to HHC or when residing in very rural communities. Prior studies examining hearing loss and QOL did not specifically report findings associated with residency or access to HHC. It could have been that the variability in findings, with some studies demonstrating that QOL was affected for those with hearing loss and others demonstrating no association between hearing loss and QOL, could have been partially explained by both geographical residency and access to HHC issues. The articles reviewed by Nordvik et al[23] did not specifically discuss how geographical residency or access to HHC might have affected the outcomes related to hearing loss and QOL. It has been reported though that access to audiological care in specific geographical regions of the country is extremely limited or nonexistent, but our understanding of access to HHC across the county and its impact on QOL is still emerging (Coco et al[8]). Future work with a larger population of participants is needed to examine how QOL can be altered for those with hearing loss who do and do not have access to HHC. Removing barriers to HHC will most likely be paramount to address QOL issues.
Advocacy and HHC
Our results also suggest that a large proportion of adults with hearing loss were not aware of their loss. Fourteen of the 27 adults who reported that they did not have a hearing loss actually had bilateral hearing losses, the majority of them being mild in degree. An additional 24 adults reported that they thought they had a hearing loss but did not see a professional to address the loss. The reasons for not accessing HHC mainly focused on financial constraints associated with HHC, not knowing how to find an HHC professional or believing that their hearing loss was not affecting their lives. Similar findings were reported in the review article by Barnett et al.[2]
If, as a profession, we are to improve audiological care to adults with hearing loss, it will be crucial to manage the barriers to HHC. Improving access will most likely involve a number of delivery models working separately or in tandem with each other. These models could include, as others have suggested, increases in the use of teleaudiology practices, the use of mobile audiology clinics, community health workers, mobile phone technology, or internet services (National Academies of Sciences Engineering Medicine;[21] Nieman and Lin;[22] van Zyl et al;[29] Ratanjee-Vanmali et al[26]). In addition, considering that financial constraints were one of the main factors for not visiting an HHC professional, changes in the affordability of HHC should be a priority for local and national public and private agencies. On a final note, a large proportion of participants in this study were not aware that they had hearing loss, and consequently, improvements in the awareness of the general decline of hearing are needed. As suggested in ‘‘HHC for Adults: Priorities for Improving Access and Affordability,'' increased awareness of the consequences of hearing loss could be provided in general wellness visits with physicians or through national public relations initiatives (National Academies of Sciences Engineering Medicine[21]).
Study Limitations
Two main limitations of this study require mentioning. First, the degree of hearing loss for most participants ranged from mild to moderate or moderately severe and did not include large numbers of participants with more severe hearing losses. It is possible that our findings would have been more convincing if larger numbers of adults with moderate to severe or moderate to profound hearing losses were included. In fact, Dalton et al[9] demonstrated that with increasing hearing loss, QOL decreased. Second, although the data suggested that poor access to HHC can lead to lower overall QOL, statistical significance was not reached most likely because of the limited number of participants. Further work should be conducted to verify the outcomes of this study.
Conclusions
Evidence from this study have suggested that individuals with hearing loss who do not have access to HHC or who live in very rural regions may have lower QOL than adults with access to HHC or who live in more metropolitan regions. In addition, outcomes from this study suggested that a number of adults with mild hearing loss could be unaware of their hearing loss. It is suggested that access to HHC be improved by addressing financial barriers to HHC and by increasing awareness of the impact a hearing loss could have on overall QOL.
-
Do you have a doctor you see for medical care? Yes__________ No__________
-
If yes, who is your doctor?
-
Family doctor: name____________________
-
Internal medicine doctor: name____________________
-
Other:______________________________
-
-
How do you get to your doctor?
-
By walking
-
By taxi
-
By bus
-
Own car
-
Other:____________________
-
-
How long does it take you to get there?
-
Less than 15 minutes
-
15 to 30 minutes
-
31 to 60 minutes (one hour)
-
61 to 90 minutes
-
91 to 120 minutes (two hours)
-
More than 120 minutes (two hours)
-
-
If you do not have a doctor, what is the main reason?
-
Seldom or never get sick
-
Recently moved to the area
-
Don't know where to go for care
-
My doctor is no longer available in my area
-
Just changed insurance plans
-
Don't use doctors
-
No health insurance
-
Medical care is too expensive
-
Other reason:______________________________
-
-
If you do have a doctor, how difficult is it to contact them during regular business hours over the telephone about a health problem?
-
Very difficult
-
Somewhat difficult
-
Not too difficult
-
Not difficult at all
-
-
Do you have difficulty going to your doctor when you need to? Yes__________ No__________
-
If yes, what is the main reason you have difficulty getting to the doctor?
-
Can't afford care
-
Insurance company doesn't approve to pay for the care
-
Doctor doesn't accept insurance plan
-
I have a problem getting to the doctor's office
-
Can't get time off work
-
Don't know a doctor who can provide medical care
-
Was refused services
-
Can't get child care
-
Don't have time or it takes too long
-
Other:______________________________
-
-
Where do you usually go if you are sick?
-
Hospital
-
Clinic
-
Doctor's office
-
Other professional
-
-
How do you get there?
-
By walking
-
By taxi
-
By bus
-
Own car
-
-
How long does it take you to get there?
-
Less than 15 minutes
-
15 minutes to 30 minutes
-
31 minutes to 60 minutes (one hour)
-
61 to 90 minutes
-
91 to 120 minutes (two hours)
-
More than 120 minutes (two hours)
-
-
Do you have difficulty going to the hospital when you need to? Yes__________ No__________
-
If yes, what is the main reason you have difficulty getting to the hospital?
-
Can't afford care
-
Insurance company doesn't approve to pay for the care
-
Doctor doesn't accept insurance plan
-
I have a problem getting to the hospital
-
Can't get time off work
-
Don't know where the hospital is
-
Was refused services
-
Can't get child care
-
Don't have time or it takes too long
-
Other:______________________________
-
-
Do you think you have a hearing loss? Yes__________ No__________
-
If you think you have a hearing loss, do you see a professional who provides care for your hearing loss? Yes__________ No__________
-
If you do see a hearing specialist, how long does it take you to get there?
-
Less than 15 minutes
-
15 to 30 minutes
-
31 to 60 minutes (one hour)
-
61 to 90 minutes
-
91 to 120 minutes (two hours)
-
More than 120 minutes (two hours)
-
-
If you think you have a hearing loss but do not see a hearing specialist, what is the main reason?
-
Can't afford care for my hearing loss
-
Insurance doesn't cover HHC
-
I have a problem getting to the professional
-
Can't get time off work
-
Don't know a professional who can provide HHC
-
Was refused services
-
Can't get child care
-
Don't have time or it takes too long
-
Other: ______________________________
-
Abbreviations
Conflict of Interest
None declared.
Acknowledgments
We are very appreciative of the funding provided by The University of Alabama's College of Arts and Sciences, the Office of Research and Economic Development and Academic Affairs for this project. We are also greatly indebted to the undergraduate students in the Department of Communicative Disorders, who provided help with data collection, including Emily Casson, Asia Crenshaw, Kristyn Conrad, Jenna Dworak, Leah LeCroy, Hayden Mills, Reagan Sandoz, and Marissa Williamson.
Notes
Portions of this paper were presented at the 46th Annual Scientific and Technology Conference of the American Auditory Society in Scottsdale, AZ, February 28-March 2, 2019.
-
References
- 1 AHRQ. Access to Care (AC) Section. 2005 https://meps.ahrq.gov/survey_comp/hc_survey/2005/AC95.htm . Accessed October 2, 2018
- 2 Barnett M, Hixon B, Okwiri N, Irungu C, Ayugi J, Thompson R, Shinn JB, Bush ML. Factors involved in access and utilization of adult hearing healthcare: a systematic review. Laryngoscope 2017; 127 (05) 1187-1194
- 3 Carhart R, Jerger J. A preferred method for the clinical determination of pure tone thresholds. J Speech Hear Disord 1959; 24: 330-345
- 4 Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40: 373-383
- 5 Chew H, Yeak S. Quality of life in patients with untreated age-related hearing loss. J Laryngol Otol 2010; 124 (08) 835-841
- 6 Chia E-M, Wang JJ, Rochtchina E, Cumming RR, Newall P, Mitchell P. Hearing impairment and health-related quality of life: the Blue Mountains hearing study. Ear Hear 2007; 28 (02) 187-195
- 7 Cleary KK, Howell DM. Using the SF-36 to determine perceived health-related quality of life in rural Idaho seniors. J Allied Health 2006; 35 (03) 156-161
- 8 Coco L, Titlow KS, Marrone N. Geographic distribution of the hearing aid dispensing workforce: a teleaudiology plan- ning assessment for Arizona. Am J Audiol 2018; 27 (3, Suppl): 462-473
- 9 Dalton DS, Cruickshanks KJ, Klein BE, Klein R, Wiley TL, Nondahl DM. The impact of hearing loss on quality of life in older adults. Gerontologist 2003; 43 (05) 661-668
- 10 DHHS. State Standards for Access to Care in Medicaid Managed Care. 2014 https://oig.hhs.gov/oei/reports/oei-02-11-00320.pdf . Accessed June 1, 2017
- 11 Farquhar M. Elderly people's definitions of quality of life. Soc Sci Med 1995; 41 (10) 1439-1446
- 12 Frisch MB. Quality of Life Inventory. Minneapolis, MN: National Computer Systems; 1994
- 13 Hart PD. Sex differences in the physical inactivity and health-related quality of life relationship among rural adults. Health Promot Perspect 2016; 6 (04) 185-189
- 14 Helvik A-S, Jacobsen G, Halberg LR. Psychological well-being of adults with acquired hearing impairment. Disabil Rehabil 2006; 28 (09) 535-545
- 15 Howell DM, Cleary KK. Rural seniors' perceptions of quality of life. Phys Occup Ther Geriatr 2007; 25 (04) 55-71
- 16 Hughson W, Westlake H. Manual for program outline for rehabilitation of aural casualties both military and civilian. Trans Am Acad Ophthalmol Otolaryngol 1944; 48: 1-15
- 17 Lamu AN, Olsen JA. The relative importance of health, income and social relations for subjective well-being: an integrative analysis. Soc Sci Med 2016; 152: 176-185
- 18 Lemos CF, Rodrigues MP, Veiga JR. Family income is associated with quality of life in patients with chronic kidney disease in the pre-dialysis phase: a cross sectional study. Health Qual Life Outcomes 2015; 13: 202
- 19 Lindner P, Andersson G, Ost LG, Carlbring P. Validation of the internet-administered Quality of Life Inventory (QOLI) in different psychiatric conditions. Cogn Behav Ther 2013; 42 (04) 315-327
- 20 Mondelli MFCG, de Souza PJS. Quality of life in elderly adults before and after hearing aid fitting. Braz J Otorhinolaryngol 2012; 78 (03) 49-56
- 21 National Academies of Sciences Engineering Medicine. Hearing Health Care for Adults: Priorities for Improving Access and Affordability. Washington, DC: The National Academies Press; 2016
- 22 Nieman CL, Lin FR. Increasing access to hearing rehabilitation for older adults. Curr Opin Otolaryngol Head Neck Surg 2017; 25 (05) 342-346
- 23 Nordvik O, Laugen Heggdal PO, Brannstrom J, Vassbotn F, Aarstad AK, Aarstad HJ. Generic quality of life in persons with hearing loss: a systematic literature review. BMC Ear Nose Throat Disord 2018; 18: 1
- 24 Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care 1981; 19: 127-140
- 25 Pronk M, Deeg DJ, Kramer SE. Hearing status in older persons: a significant determinant of depression and loneliness? Results from the longitudinal aging study Amsterdam. Am J Audiol 2013; 22 (02) 316-320
- 26 Ratanjee-Vanmali H, Swanepoel W, Laplante-Levesque A. Characteristics, behaviours and readiness of persons seeking hearing healthcare online. Int J Audiol 2019; 58: 107-115
- 27 Robert SA, Cherepanov D, Palta M, Dunham NC, Feeny D, Fryback DG. Socioeconomic status and age variations in health-related quality of life: results from the national health measurement study. J Gerontol Ser B Psychol Sci Soc Sci 2009; 64B (03) 378-389
- 28 USDA. Rural-Urban Continuum Codes. 2017 https://www.ers.usda.gov/data-products/rural-urban-continuum-codes/documentation/ . Accessed September 25, 2018
- 29 van Zyl M, Swanepoel W, Myburgh HC. Modernising speech audiometry: using a smartphone application to test word recognition. Int J Audiol 2018; 57 (08) 561-569
- 30 Ward M, McGarrigle CA, Kenny RA. More than health: quality of life trajectories among older adults-findings from the Irish Longi- tudinal Study of Ageing (TILDA). Qual Life Res 2019; 28 (02) 429-439
- 31 World Health Organization. WHOQOL: Measuring Quality of Life. 2018 http://www.who.int/healthinfo/survey/whoqol-qualityoflife/en/ . Accessed November 16, 2018
Address for correspondence
Publication History
Article published online:
02 September 2020
© 2020. Copyright © 2020 by the American Academy of Audiology. All rights reserved.
Thieme Medical Publishers
333 Seventh Avenue, New York, NY 10001, USA.
-
References
- 1 AHRQ. Access to Care (AC) Section. 2005 https://meps.ahrq.gov/survey_comp/hc_survey/2005/AC95.htm . Accessed October 2, 2018
- 2 Barnett M, Hixon B, Okwiri N, Irungu C, Ayugi J, Thompson R, Shinn JB, Bush ML. Factors involved in access and utilization of adult hearing healthcare: a systematic review. Laryngoscope 2017; 127 (05) 1187-1194
- 3 Carhart R, Jerger J. A preferred method for the clinical determination of pure tone thresholds. J Speech Hear Disord 1959; 24: 330-345
- 4 Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40: 373-383
- 5 Chew H, Yeak S. Quality of life in patients with untreated age-related hearing loss. J Laryngol Otol 2010; 124 (08) 835-841
- 6 Chia E-M, Wang JJ, Rochtchina E, Cumming RR, Newall P, Mitchell P. Hearing impairment and health-related quality of life: the Blue Mountains hearing study. Ear Hear 2007; 28 (02) 187-195
- 7 Cleary KK, Howell DM. Using the SF-36 to determine perceived health-related quality of life in rural Idaho seniors. J Allied Health 2006; 35 (03) 156-161
- 8 Coco L, Titlow KS, Marrone N. Geographic distribution of the hearing aid dispensing workforce: a teleaudiology plan- ning assessment for Arizona. Am J Audiol 2018; 27 (3, Suppl): 462-473
- 9 Dalton DS, Cruickshanks KJ, Klein BE, Klein R, Wiley TL, Nondahl DM. The impact of hearing loss on quality of life in older adults. Gerontologist 2003; 43 (05) 661-668
- 10 DHHS. State Standards for Access to Care in Medicaid Managed Care. 2014 https://oig.hhs.gov/oei/reports/oei-02-11-00320.pdf . Accessed June 1, 2017
- 11 Farquhar M. Elderly people's definitions of quality of life. Soc Sci Med 1995; 41 (10) 1439-1446
- 12 Frisch MB. Quality of Life Inventory. Minneapolis, MN: National Computer Systems; 1994
- 13 Hart PD. Sex differences in the physical inactivity and health-related quality of life relationship among rural adults. Health Promot Perspect 2016; 6 (04) 185-189
- 14 Helvik A-S, Jacobsen G, Halberg LR. Psychological well-being of adults with acquired hearing impairment. Disabil Rehabil 2006; 28 (09) 535-545
- 15 Howell DM, Cleary KK. Rural seniors' perceptions of quality of life. Phys Occup Ther Geriatr 2007; 25 (04) 55-71
- 16 Hughson W, Westlake H. Manual for program outline for rehabilitation of aural casualties both military and civilian. Trans Am Acad Ophthalmol Otolaryngol 1944; 48: 1-15
- 17 Lamu AN, Olsen JA. The relative importance of health, income and social relations for subjective well-being: an integrative analysis. Soc Sci Med 2016; 152: 176-185
- 18 Lemos CF, Rodrigues MP, Veiga JR. Family income is associated with quality of life in patients with chronic kidney disease in the pre-dialysis phase: a cross sectional study. Health Qual Life Outcomes 2015; 13: 202
- 19 Lindner P, Andersson G, Ost LG, Carlbring P. Validation of the internet-administered Quality of Life Inventory (QOLI) in different psychiatric conditions. Cogn Behav Ther 2013; 42 (04) 315-327
- 20 Mondelli MFCG, de Souza PJS. Quality of life in elderly adults before and after hearing aid fitting. Braz J Otorhinolaryngol 2012; 78 (03) 49-56
- 21 National Academies of Sciences Engineering Medicine. Hearing Health Care for Adults: Priorities for Improving Access and Affordability. Washington, DC: The National Academies Press; 2016
- 22 Nieman CL, Lin FR. Increasing access to hearing rehabilitation for older adults. Curr Opin Otolaryngol Head Neck Surg 2017; 25 (05) 342-346
- 23 Nordvik O, Laugen Heggdal PO, Brannstrom J, Vassbotn F, Aarstad AK, Aarstad HJ. Generic quality of life in persons with hearing loss: a systematic literature review. BMC Ear Nose Throat Disord 2018; 18: 1
- 24 Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care 1981; 19: 127-140
- 25 Pronk M, Deeg DJ, Kramer SE. Hearing status in older persons: a significant determinant of depression and loneliness? Results from the longitudinal aging study Amsterdam. Am J Audiol 2013; 22 (02) 316-320
- 26 Ratanjee-Vanmali H, Swanepoel W, Laplante-Levesque A. Characteristics, behaviours and readiness of persons seeking hearing healthcare online. Int J Audiol 2019; 58: 107-115
- 27 Robert SA, Cherepanov D, Palta M, Dunham NC, Feeny D, Fryback DG. Socioeconomic status and age variations in health-related quality of life: results from the national health measurement study. J Gerontol Ser B Psychol Sci Soc Sci 2009; 64B (03) 378-389
- 28 USDA. Rural-Urban Continuum Codes. 2017 https://www.ers.usda.gov/data-products/rural-urban-continuum-codes/documentation/ . Accessed September 25, 2018
- 29 van Zyl M, Swanepoel W, Myburgh HC. Modernising speech audiometry: using a smartphone application to test word recognition. Int J Audiol 2018; 57 (08) 561-569
- 30 Ward M, McGarrigle CA, Kenny RA. More than health: quality of life trajectories among older adults-findings from the Irish Longi- tudinal Study of Ageing (TILDA). Qual Life Res 2019; 28 (02) 429-439
- 31 World Health Organization. WHOQOL: Measuring Quality of Life. 2018 http://www.who.int/healthinfo/survey/whoqol-qualityoflife/en/ . Accessed November 16, 2018