

Subscribe to RSS
DOI: 10.1055/s-0046-1816583
Effect of Water Storage on Microleakage of Class II MOD Bulk-fill Resin Composite Restorations: In Vitro Evaluation
Authors

Abstract
Objective
To evaluate and compare the effect of 6-month water storage on the marginal microleakage of class II MOD cavities restored with two different bulk-fill resin composites (sculptable and no-cap flowable) and a conventional resin composite.
Materials and Methods
A total of 60 sound freshly extracted mandibular molars, each with a standardized class II MOD cavity, were assigned into three main groups according to the restorative material used as follows: bulk-fill resin composite (SimpliShade, Kerr), no-cap flowable bulk-fill resin composite (G-aenial Bulk Injectable, GC), and conventional resin composite (Neo Spectra ST LV, Dentsply Sirona). Each group was further divided into two subgroups (n = 10) based on the water-storage time: 24 hours (immediate) and 6-month water storage (aged). All specimens were thermocycled 5,000 times between 5°C ± 2°C and 55°C ± 2°C, then immersed in 2% basic fuchsin dye for 24 hours. The specimens were longitudinally sectioned, and the amount of dye penetration was evaluated using stereomicroscope under 25× magnification. The results were analyzed by non-parametric Kruskal-Wallis, Mann-Whitney, and Wilcoxon signed-rank tests. The level of significance was set at p <0.05.
Results
Both bulk-fill resin composites exhibited significantly lower microleakage scores than conventional resin composite (p <0.05). However, 6-month water storage significantly increased the microleakage for all tested groups.
Conclusions
Water storage has a negative impact on the marginal microleakage regardless of the type of the restoration.
Introduction
One of the most essential factors determining the success of a restoration is its ability to conform to the prepared tooth surface, properly adapt, and effectively seal the cavity walls, thereby ensuring long-term clinical performance.[1] [2] Ideally, a strong bond between the restorative material and the tooth structure should result in a tight, concealed marginal seal.[3] Despite stupendous technological advancements, achieving a perfect marginal seal remains a persistent challenge,[4] since no restorative material could optimally adhere and form such intimate contact to the tooth surface.[5] Consequently, marginal gaps may develop along the interface between the cavity walls and the restorative material, allowing the passage of bacteria, molecules, ions, and fluids through the tooth–restoration interface, which is referred to as microleakage.[6] [7] Clinically, microleakage can result in marginal discoloration, secondary caries, pulpal inflammation, and postoperative sensitivity.[8]
Indirect restorations are considered a highly recommended treatment option for managing large defects in posterior teeth.[9] [10] [11] However, using indirect restorations is more time-consuming and involves additional costs and appointments that may not align with the patient's preferences and budget.[12] Consequently, direct resin composite restorations have been adopted as an easier and more practical alternative, showing comparable clinical longevity to indirect restorations in posterior teeth.[13] Resin composite restorative materials have undergone remarkable improvements since their introduction to the field of restorative dentistry.[14] [15] A major clinical challenge, however, is the selection of an appropriate placement technique particularly when restoring class II cavities.[16] Direct resin composite restorations are conventionally applied in increments, with each layer cured separately in the so-called incremental filling technique. Despite considered the standard technique, it exhibits several drawbacks including prolonged application time, potential internal flexure, and entrapment of voids between layers.[17] [18]
Bulk-fill resin composites were recently introduced to the dental market in an attempt to overcome the limitations of conventional resin composites. These materials can be placed in a single increment of up to 4 to 5 mm and cured in bulk, which simplifies the restorative procedures and reduces the time required for placement.[19] [20] [21] Their ability to undergo bulk polymerization is attributed to modifications in chemical composition by using modified monomers that minimize polymerization shrinkage stresses. Moreover, the increased translucency achieved by modifying the filler systems, along with incorporating alternative photoinitiators, facilitates deeper light penetration and improved depth of cure.[22] [23]
Current bulk-fill resin composites are categorized into sculptable (high-viscosity) and flowable (low-viscosity) based on their filler content.[24] High-viscosity bulk-fill composite can substitute both enamel and dentin in a single increment without any capping layer owing to its high filler load.[25] [26] On the other hand, the flowable bulk-fill composites were only limited to restoring simple proximal cavities or serving as dentin replacement materials, as their low surface hardness and modulus of elasticity necessitate a final coverage with a conventional resin composite.[25] [27] More recently, an enhanced category of flowable bulk-fill composites has been developed, which can be placed in one layer up to 4 mm without requiring a composite capping layer owing to the full-coverage silane coating of its filler nanoparticles, thereby providing high flexural strength and extraordinary wear resistance.[18] [28] [29]
Since microleakage represents a major cause of restoration failure, its evaluation remains an important parameter for assessing the clinical success of bulk-fill restorative materials.[8] Furthermore, another parameter to consider is the water-storage effect, as the tooth–restoration interface is constantly exposed to saliva and consequently subjected to degradation in the oral cavity.[30] Indeed, numerous studies have evaluated the microleakage of bulk-fill compared to conventional resin composites in class II restorations.[8] [31] [32] [33] However, according to the authors' knowledge, no studies have evaluated the microleakage of the recently introduced G-aenial Bulk Injectable, a flowable bulk-fill resin composite without a capping layer, particularly with respect to the effect of water storage. Therefore, the aim of this study was to assess and compare the microleakage of class II MOD cavities restored with bulk-fill, no-cap flowable bulk-fill, and conventional resin composite, both immediately and after 6-month water storage. The null hypothesis tested was that the microleakage would not be influenced by the type of resin composite or the time of storage.
Materials and Methods
Restorative Materials
In the current study, the resin composite restorative materials and their corresponding adhesive systems were: bulk-fill resin composite (SimpliShade/OptiBond Universal, Kerr, Orange, CA, USA), no-cap flowable bulk-fill resin composite (G-aenial Bulk Injectable/G-Premio Bond, GC, Tokyo, Japan), and conventional resin composite (Neo Spectra ST LV/Prime & Bond Universal, Dentsply Sirona GmbH, Konstanz, Germany). A detailed description of each material is presentenced in [Table 1].
Abbreviations: 4-MET, 4-methacryloxyethyl trimellitate; BHT, butylated hydroxytoluene; Bis-EMA, bisphenol-A ethoxylated dimethacrylate; MDP, methacryloyloxydecyl dihydrogen phosphate; MDTP, 10-methacryloyloxydecyl dihydrogen thiophosphate; PENTA, dipentaerythritol pentacrylate phosphate; UDMA, urethane dimethacrylate; UV light, ultraviolet light.
Teeth Selection
A total of 60 sound freshly extracted, non-carious human mandibular molars with comparable dimensions were collected from healthy individuals at the Oral Surgery Department Clinic after gaining informed consent. The ethical approval was granted by the Faculty Research Ethics Committee under protocol number 024121261. All methods were carried out in accordance with relevant guidelines and regulations of Helsinki Declarations. After removing any residual calculus or plaque, teeth were disinfected using 0.5% chloramine-T solution and then were cleansed using a rubber cup and fine pumice water slurry. A binocular stereomicroscope (SZ TP, Olympus, Tokyo, Japan) was used for detecting any microscopic cracks or enamel craze lines. To avoid teeth dehydration, they were stored in distilled water at 37°C ± 1°C using an incubator (BTC, BioTech Company, Cairo, Egypt) and removed only for testing.[34] [35]
Sample Size Calculation
Sample size was calculated using a statistical software program (G*Power, Ver.3.1.9.1, Dusseldorf, Germany) based on a previous study.[36] A two-tailed test with an effect size of 1.37, a significance level (α) of 0.01, and 99% statistical power was considered. Therefore, a representative sample composed of 10 teeth per subgroup was selected for this study.
Specimens' Preparation
Each tooth was fixed in self-curing acrylic blocks up to 2 mm below the cementoenamel junction (CEJ).[22] Standardized class II MOD cavities were prepared using a flat-ended, straight fissure diamond instrument (836.HP.027; Komet, Brasseler, Lemgo, Germany) in a high-speed handpiece (Dentsply Sirona GmbH, Konstanz, Germany) under continuous air–water cooling. The depth of the prepared cavity was 4 mm from the central groove, with a width of two-third of the intercuspal distance. The buccal and lingual walls were prepared parallel to each other, with a 90 degrees cavosurface angle. The width of proximal boxes was also two-third of the buccolingual distance. The axial wall of each box was at 1.5 mm depth. The cervical margins were placed 1 mm coronal to CEJ. All prepared cavities were finished using extra-fine diamond instruments (835KREF.314.012, Komet) in order to obtain smooth walls and rounded internal angles.[18] A magnifying aid with LED light (Perioptix Inc, Central Ave, CA, USA) was used to ensure proper cavity preparation. A digital caliper (Whitworth, CA, USA) was used for measuring the cavity dimensions. The prepared teeth were assigned randomly into three main groups (n = 20) using a random generator software via a specific website (https://www.random.org), based on the resin composite restorative material as follows:
-
Group 1–Bulk-fill resin composite, SimpliShade bulk-fill
-
Group 2–No-cap flowable bulk-fill resin composite, G-aenial Bulk Injectable
-
Group 3–Conventional resin composite, Neo Spectra ST LV
Restorative Procedures
A circumferential metal matrix/band (Omni-Matrix, Ultradent Products, South Jordan, UT, USA) was fixed around each prepared tooth in order to restore the proximal contours.[37] The enamel margins were etched using 37% phosphoric acid gel for 15 to 20 seconds (N-Etch, IvoclarVivadent AG, Schaan, Liechtenstein) following selective enamel etching protocol. The cavity preparation was then thoroughly rinsed by water for 10 seconds and gently dried with oil-free air. Subsequently, each universal adhesive was applied to enamel and dentin using microbrush, scrubbed for 20 seconds, gently air-dried for 5 seconds, and then light-cured for 10 seconds according to the manufacturers' instructions using a light-emitting diode (LED) curing unit (Elipar S10, 3M Oral Care) with a light intensity of 1,200 mW/cm2, as calibrated by the built-in radiometer.
For both bulk-fill groups, the prepared cavities were restored in one bulk increment (4 mm) and light-cured for 10 seconds. Meanwhile, conventional resin composite was applied in increments of 2 mm thickness and cured separately for 10 seconds. The proximal surfaces of all restorations were further cured for 10 seconds from buccal and lingual surfaces after matrix removal to ensure optimum polymerization. Finishing and polishing procedures were performed using high-speed diamond finishing instruments (4092.314, Komet) under copious air–water cooling followed by flexible discs (Sof-Lex XT Pop On, 3M Oral Care) and rubber polishing points (OneGloss, Shofu, Kyoto, Japan).
Testing
Half of the specimens of each group (n = 10) were stored in distilled water in an incubator (BTC, BioTech Company, Cairo, Egypt) at 37°C ± 1°C for 24 hours (immediate), then thermocycled for 5,000 cycles between 5°C ± 2°C and 55°C ± 2°C with dwell time of 30 seconds and transfer time of 2 seconds from one bath to the other.[18] The other half of the specimens were stored for 6 months before subjecting to thermocycling (aged).
The teeth were then coated with three coats of nail polish except for the restoration and 1 mm rim of the tooth structure, then immersed in 2% basic fuchsin dye solution in dark room for 24 hours.[35] [38] After washing thoroughly with distilled water, teeth were sectioned in mesio-distal direction into two halves by a cutting saw machine (ISOMET 4000, Buehler, Lake Bluff, IL, USA) at speed of 2,500 rpm under copious water cooling. The resulted cross-sections were examined by stereomicroscope (SZ TP, Olympus, Tokyo, Japan) at 25× magnification.[31] [32]
Microleakage was scored based on the degree of dye penetration using a five-grade scoring system as follows: 0 = no dye penetration; 1 = superficial dye penetration not beyond amelodentinal junction (ADJ); 2 = dye penetration along the gingival wall; 3 = dye penetration along the gingival and axial walls; 4 = dye penetration along the pulpal floor.[32]
Statistical Analysis
Data were collected and statistically analyzed using a statistical software package (IBM-SPSS, version 24, Armonk, NY, USA). Since the results exhibited clearly ordinal structural data, and the data did not follow a normal distribution pattern according to the Shapiro–Wilk test (p < 0.05), a non-parametric analysis of variance, Kruskal-Wallis test, was used to compare between different groups at each storage time. Mann-Whitney U test was used for pairwise comparisons, while Wilcoxon signed-rank test was used to assess the effect of storage time on group. The level of significance was set at p <0.05.
Results
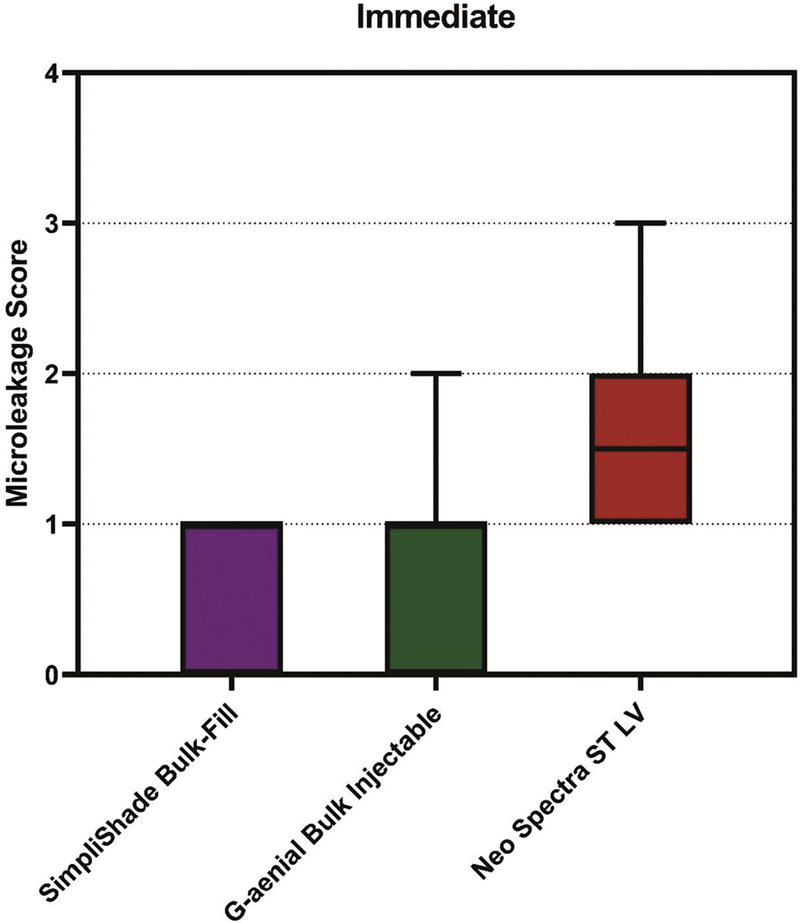
Microleakage results among the tested groups are shown in [Table 2]. Kruskal-Wallis test indicated a significant difference in the microleakage scores among the three tested groups immediately (p = 0.001) and after 6 months (p = 0.002). The microleakage scores in both bulk-fill groups were significantly lower than those of the conventional group (p < 0.05). For all immediately restored groups, score 3 was observed only for conventional resin composite group. Score 4 was not noted for any of the immediate groups, while it was recorded for both no-cap flowable bulk-fill and conventional resin composite groups after 6-month water storage.
|
SimpliShade Bulk-Fill |
G-aenial Bulk Injectable |
Neo Spectra ST LV |
p-value |
p1 |
p2 |
p3 |
|
|---|---|---|---|---|---|---|---|
|
Immediate |
1.00 (0.00–1.00) |
1.00 (0.00–2.00) |
1.5 (1.00–3.00) |
0.001[*] |
0.326 |
0.002[*] |
0.009[*] |
|
Aged |
2.00 (1.00–3.00) |
2.00 (1.00–4.00) |
3.00 (1.00–4.00) |
0.002[*] |
0.804 |
0.001[*] |
0.005[*] |
|
p -value |
0.003[*] |
0.006[*] |
0.001[*] |
Notes: p1: SimpliShade Bulk-Fill vs. G-aenial Bulk Injectable.
p2: SimpliShade Bulk-Fill vs. Neo Spectra ST LV.
p3: G-aenial Bulk Injectable vs. Neo Spectra ST LV.
* Statistically significant at p <0.05.
For immediately tested groups, Mann-Whitney U test indicated no statistically significant difference between bulk-fill and no-cap flowable bulk-fill restored groups (p = 0.326). Both bulk-fill restored groups exhibited significantly lower microleakage scores compared to the conventional resin composite group (p < 0.05) ([Fig. 1]). For groups tested after 6-month water storage, there was also no statistically significant difference between bulk-fill and no-cap flowable bulk-fill restored groups (p = 0.804). The conventional resin composite group showed significantly higher microleakage scores than both bulk-fill restored groups (p < 0.05) ([Fig. 2]).

Regarding the effect of storage time, the results of the Wilcoxon signed-rank test revealed that each immediately restored group showed significantly lower microleakage scores compared with its corresponding aged group (p < 0.05). Different microleakage patterns and the amount of dye penetration are presented in [Fig. 3].

Discussion
One of the major causes of restoration failure is microleakage that occurs due to presence of microscopic openings at the tooth–restoration interface.[39] The current in vitro study evaluated the microleakage of class II MOD cavities restored with two different types of bulk-fill resin composite restorative materials in comparison to conventional resin composite immediately and after 6-month water storage. The study results showed that both types of bulk-fill resin composites exhibited superior resistance to microleakage compared to conventional resin composite. Moreover, water storage had a negative effect on the tested groups. Therefore, the null hypothesis formulated at the beginning of the study was rejected.
Class II MOD cavities were prepared to simulate a clinically challenging scenario involving the loss of both marginal ridges.[18] Unlike conventional resin composites, which require incremental placement, bulk-fill composites can be applied in a single 4-mm increment, simplifying the procedure and reducing chair time.[40] [41] A novel flowable bulk-fill composite was selected in this study, providing the additional advantage of eliminating the need for a final capping layer.[28] The incorporation of densely packed, ultra-fine fillers contributes to high flexural strength and reduces internal shear stress within the polymer matrix. Additionally, the distribution of fillers, represented by the closely packed particles, helps protect the interstitial resin from abrasion by neighboring particles, thereby providing better wear resistance.[29]
Each tested composite material was applied with its corresponding universal adhesive from the same manufacturer to ensure compatibility and avoid potential inaccuracies.[2] A key limitation of universal adhesives when applied in self-etch mode is their inadequate etching of enamel, producing a shallow and poorly defined etching pattern. Therefore, selective enamel etching was employed to ensure reliable bonding to enamel, which is essential for establishing an effective marginal seal and protecting the underlying dentin bond from degradation.[42]
Dye penetration technique is one of the simplest and most commonly used methods for evaluating microleakage, being highly feasible, easily reproducible, and involving no reactive chemicals or radiation.[5] [43] [44] [45] Basic fuchsin dye was utilized for its low cost, wide availability, and ease of use without requiring sophisticated laboratory equipment. Specimens were immersed in the dye for 24 hours, a duration deemed sufficient for leakage assessment without compromising the adhesive interface, as supported by Pushpa and Suresh[38] and Sawani et al.[46]
Evaluating the performance of new restorative materials requires replicating oral challenges, including fluctuations in temperature and humidity. In this study, specimens underwent 5,000 thermal cycles following ISO standard protocol (ISO TR 11450) to simulate thermal stresses from hot and cold extremes intraorally.[18] To further replicate oral conditions and intensify the aging effect, half of the specimens were stored in distilled water for 6 months, promoting water sorption and the release of incompletely polymerized monomers, which may affect the long-term durability of the restorations.[47] [48]
The two bulk-fill resin composites demonstrated superior marginal sealing compared to the conventional resin composite, both immediately and after aging. This favorable performance of bulk-fill resin composites may be attributed to their lower polymerization shrinkage and associated stresses, which may contribute to better adaptation to cavity walls and reduced microleakage.[49] [50] [51] These findings are consistent with several in vitro studies that reported reduced microleakage and improved marginal sealing when bulk-fill resin composites were compared with incrementally placed conventional ones.[52] [53] In contrast, other studies have reported comparable or even inferior marginal sealing performance of bulk-fill resin composites relative to conventional resin composites.[33] [39] [54] Such discrepancies may be attributed to differences in evaluation protocols, cavity design, materials tested, and the dye employed.
The comparable performance of both the bulk-fill resin composites may be attributed to their high translucency and improved depth of cure, which result in a favorable degree of conversion and controlled polymerization stresses, contributing to better marginal sealing irrespective of material consistency.[55] This observation aligns with previous reports indicating no significant influence of bulk-fill resin composite consistency on marginal microleakage.[32] [56] However, some studies reported contradictory outcomes when flowable types were compared with higher-viscosity formulations.[57] [58] These conflicts may be ascribed to the compositional differences between the investigated materials as well as variations in the experimental conditions.
Water storage impaired marginal sealing in all tested materials. This effect may be attributed to resin composite degradation induced by water sorption, which can compromise the integrity of the polymer network and promote hydrolysis at the filler–matrix interface. These findings are in line with those of Scotti et al[59] who reported increased dye penetration in resin composites after 12 months of storage. However, a previous study found no significant effect of water storage on marginal leakage, likely due to the 3-month storage duration being insufficient to induce measurable degradation.[30]
It should be recognized that the current study has certain limitations. One of these limitations was the 6-month storage period, which may not fully capture the effects of long-term aging on the materials' marginal sealing. Another limitation was relying on the basic fuchsin dye penetration technique as the sole method for microleakage assessment. Along with its subjective assessment, the small particle size of basic fuchsin dye allows deeper penetration into dentinal tubules, possibly staining dentin, which could affect the reliability of the test.[45]
Future studies evaluating marginal sealing should consider using alternative dyes, such as silver nitrate, which may provide a more reliable assessment and reduce potential exaggerated results. In addition, advanced evaluation techniques, including confocal laser scanning microscopy (CLSM), optical coherence tomography (OCT), and micro-computed tomography (micro-CT), should be incorporated to allow a more accurate, objective, and comprehensive evaluation of microleakage. Furthermore, studies with longer storage durations are recommended to better assess the durability of marginal sealing under long-term aging conditions.
Conclusion
Within the limitations of the current study, it was concluded that:
-
None of the tested resin composites were completely free from microleakage.
-
Bulk-fill and no-cap flowable bulk-fill resin composites outperformed conventional resin composite with lower microleakage values in large class II MOD cavities.
-
For all tested materials, 6-month water storage had a negative effect on marginal sealing.
Conflict of Interest
None declared.
-
References
- 1 Jia S, Chen D, Wang D, Bao X, Tian X. Comparing marginal microleakage of three different dental materials in veneer restoration using a stereomicroscope: an in vitro study. BDJ Open 2017; 3: 16010
- 2 El-Maksoud OA, Hamama H, Wafaie RA, El-Wassefy N, Mahmoud SH. Impact of refrigeration of different resin composite restorative materials on the marginal adaptation in class II restorations. BMC Oral Health 2024; 24 (01) 1174
- 3 Shih WY. Microleakage in different primary tooth restorations. J Chin Med Assoc 2016; 79 (04) 228-234
- 4 Pecie R, Onisor I, Krejci I, Bortolotto T. Marginal adaptation of direct class II composite restorations with different cavity liners. Oper Dent 2013; 38 (06) E210-E220
- 5 Punathil S, Almalki SA, AlJameel AH, Gowdar IM, Mc VA, Chinnari K. Assessment of microleakage using dye penetration method in primary teeth restored with tooth-colored materials: an in vitro study. J Contemp Dent Pract 2019; 20 (07) 778-782
- 6 Karaman E, Ozgunaltay G. Polymerization shrinkage of different types of composite resins and microleakage with and without liner in class II cavities. Oper Dent 2014; 39 (03) 325-331
- 7 Cobanoglu N, Ozer F, Demirci M, Erganis O, Imazato S. Bacterial penetration of restored cavities using two self-etching bonding systems. Eur J Dent 2014; 8 (02) 166-171
- 8 Cayo-Rojas CF, Hernández-Caba KK, Aliaga-Mariñas AS, Ladera-Castañeda MI, Cervantes-Ganoza LA. Microleakage in class II restorations of two bulk fill resin composites and a conventional nanohybrid resin composite: an in vitro study at 10,000 thermocycles. BMC Oral Health 2021; 21 (01) 619
- 9 Vetromilla BM, Opdam NJ, Leida FL. et al. Treatment options for large posterior restorations: a systematic review and network meta-analysis. J Am Dent Assoc 2020; 151 (08) 614-624.e18
- 10 Kimmel M, Faggion Jr CM. Systematic reviews comparing direct and indirect restorations: an umbrella review that examines restoration type and confidence in results. Clin Exp Dent Res 2025; 11 (03) e70149
- 11 Opdam N, Frankenberger R, Magne P. From “direct versus indirect” toward an integrated restorative concept in the posterior dentition. Oper Dent 2016; 41 (S7): S27-S34
- 12 Incekara MS, Karadas M. Clinical comparison of direct and indirect class II composite restorations: a prospective 12-month follow-up study. BMC Oral Health 2025; 25 (01) 1217
- 13 Josic U, D'Alessandro C, Miletic V. et al. Clinical longevity of direct and indirect posterior resin composite restorations: an updated systematic review and meta-analysis. Dent Mater 2023; 39 (12) 1085-1094
- 14 St-Pierre L, Bergeron C, Qian F. et al. Effect of polishing direction on the marginal adaptation of composite resin restorations. J Esthet Restor Dent 2013; 25 (02) 125-138
- 15 Karabela MM, Sideridou ID. Synthesis and study of properties of dental resin composites with different nanosilica particles size. Dent Mater 2011; 27 (08) 825-835
- 16 Moda MD, Briso AF, Hoshino I. et al. Three-year randomized prospective clinical trial of class II restorations using flowable bulk-fill resin composites. Oper Dent 2021; 46 (05) 516-528
- 17 Loguercio AD, Rezende M, Gutierrez MF, Costa TF, Armas-Vega A, Reis A. Randomized 36-month follow-up of posterior bulk-filled resin composite restorations. J Dent 2019; 85: 93-102
- 18 Wafaie RA, Ahmed B, Mahmoud SH. Fracture resistance of molars with class II MOD cavities restored with bulk-fill, no-cap flowable bulk-fill, and conventional resin composite restorative systems after 6-months water storage. BMC Oral Health 2025; 25 (01) 741
- 19 Gerula-Szymańska A, Kaczor K, Lewusz-Butkiewicz K, Nowicka A. Marginal integrity of flowable and packable bulk fill materials used for class II restorations—a systematic review and meta-analysis of in vitro studies. Dent Mater J 2020; 39 (03) 335-344
- 20 Tauböck TT, Marovic D, Zeljezic D, Steingruber AD, Attin T, Tarle Z. Genotoxic potential of dental bulk-fill resin composites. Dent Mater 2017; 33 (07) 788-795
- 21 Zorzin J, Maier E, Harre S. et al. Bulk-fill resin composites: polymerization properties and extended light curing. Dent Mater 2015; 31 (03) 293-301
- 22 Gamarra VSS, Borges GA, Júnior LHB, Spohr AM. Marginal adaptation and microleakage of a bulk-fill composite resin photopolymerized with different techniques. Odontology 2018; 106 (01) 56-63
- 23 Bucuta S, Ilie N. Light transmittance and micro-mechanical properties of bulk fill vs. conventional resin based composites. Clin Oral Investig 2014; 18 (08) 1991-2000
- 24 Yazici AR, Kutuk ZB, Ergin E, Karahan S, Antonson SA. Six-year clinical evaluation of bulk-fill and nanofill resin composite restorations. Clin Oral Investig 2022; 26 (01) 417-426
- 25 Atalay C, Yazici AR, Horuztepe A, Nagas E, Ertan A, Ozgunaltay G. Fracture resistance of endodontically treated teeth restored with bulk fill, bulk fill flowable, fiber-reinforced, and conventional resin composite. Oper Dent 2016; 41 (05) E131-E140
- 26 Ferracane JL. Resin composite—state of the art. Dent Mater 2011; 27 (01) 29-38
- 27 Sartawi SY, AbuSidu Z, El-Qawasmi Y, Salim NA. In vitro analysis of flowable and high viscosity bulk fill composite versus conventional composite in core build up of endodontically treated teeth. Sci Rep 2024; 14 (01) 28013
- 28 Khoramian Tusi S, Hamdollahpoor H, Mohammadi Savadroodbari M, Sheikh Fathollahi M. Comparison of polymerization shrinkage of a new bulk-fill flowable composite with other composites: an in vitro study. Clin Exp Dent Res 2022; 8 (06) 1605-1613
- 29 Ujiie M, Tsujimoto A, Barkmeier WW. et al. Comparison of occlusal wear between bulk-fill and conventional flowable resin composites. Am J Dent 2020; 33 (02) 74-78
- 30 Sadek FT, Moura SK, Ballester RY, Muench A, Cardoso PE. The effect of long-term storage on the microleakage of composite resin restorations: qualitative and quantitative evaluation. Pesqui Odontol Bras 2003; 17 (03) 261-266
- 31 Moorthy A, Hogg CH, Dowling AH, Grufferty BF, Benetti AR, Fleming GJ. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J Dent 2012; 40 (06) 500-505
- 32 Tomaszewska IM, Kearns JO, Ilie N, Fleming GJ. Bulk fill restoratives: to cap or not to cap—that is the question?. J Dent 2015; 43 (03) 309-316
- 33 Rengo C, Spagnuolo G, Ametrano G. et al. Marginal leakage of bulk-fill composites in class II restorations: a microCT and digital microscope analysis. Int J Adhes Adhes 2015; 60: 123-129
- 34 Sahli A, Daeniker L, Rossier I. et al. Comparison of class II bulk-fill, self-adhesive composites, alkasite, and high-viscosity glass ionomer restorations in terms of marginal and internal adaptation. Materials (Basel) 2024; 17 (17) 4373
- 35 Şenol AA, Karabulut Gençer B, Tarçın B, Kahramanoğlu E, Yılmaz Atalı P. Microleakage and marginal integrity of ormocer/methacrylate-based bulk-fill resin restorations in MOD cavities: SEM and stereomicroscopic evaluation. Polymers (Basel) 2023; 15 (07) 1716
- 36 Kalmowicz J, Phebus JG, Owens BM, Johnson WW, King GT. Microleakage of class I and II composite resin restorations using a sonic-resin placement system. Oper Dent 2015; 40 (06) 653-661
- 37 García Marí L, Climent Gil A, LLena Puy C. In vitro evaluation of microleakage in class II composite restorations: high-viscosity bulk-fill vs conventional composites. Dent Mater J 2019; 38 (05) 721-727
- 38 Pushpa R, Suresh BS. Marginal permeability of one step self-etch adhesives: effects of double application or the application of hydrophobic layer. J Conserv Dent 2010; 13 (03) 141-144
- 39 Poggio C, Chiesa M, Scribante A, Mekler J, Colombo M. Microleakage in class II composite restorations with margins below the CEJ: in vitro evaluation of different restorative techniques. Med Oral Patol Oral Cir Bucal 2013; 18 (05) e793-e798
- 40 Çağırır Dindaroğlu F, Yılmaz E. Two-year evaluation of a nano-hybrid and a bulk-fill resin composite: a randomized, double-blind split-mouth clinical study. Clin Oral Investig 2024; 28 (04) 208
- 41 de Assis FS, Lima SN, Tonetto MR. et al. Evaluation of bond strength, marginal integrity, and fracture strength of bulk- vs incrementally-filled restorations. J Adhes Dent 2016; 18 (04) 317-323
- 42 Ahmed B, El-Maksoud OA, Wafaie RA, Mahmoud SH. Effect of short dentin etching and water storage on bonding of resin composite to dentin with universal and two-step self-etch adhesive systems. Sci Rep 2025; 15 (01) 43817
- 43 Ernst CP, Galler P, Willershausen B, Haller B. Marginal integrity of class V restorations: SEM versus dye penetration. Dent Mater 2008; 24 (03) 319-327
- 44 Ozel E, Korkmaz Y, Attar N. Influence of location of the gingival margin on the microleakage and internal voids of nanocomposites. J Contemp Dent Pract 2008; 9 (07) 65-72
- 45 AlHabdan AA. Review of microleakage evaluation tools. J Int Oral Health 2017; 9: 141-145
- 46 Sawani S, Arora V, Jaiswal S, Nikhil V. Comparative evaluation of microleakage in class II restorations using open vs. closed centripetal build-up techniques with different lining materials. J Conserv Dent 2014; 17 (04) 344-348
- 47 Saboia VP, Silva FC, Nato F. et al. Analysis of differential artificial ageing of the adhesive interface produced by a two-step etch-and-rinse adhesive. Eur J Oral Sci 2009; 117 (05) 618-624
- 48 Coelho-De-Souza FH, Camacho GB, Demarco FF, Powers JM. Fracture resistance and gap formation of MOD restorations: influence of restorative technique, bevel preparation and water storage. Oper Dent 2008; 33 (01) 37-43
- 49 Parra Gatica E, Duran Ojeda G, Wendler M. Contemporary flowable bulk-fill resin-based composites: a systematic review. Biomater Investig Dent 2023; 10 (01) 8-19
- 50 Kapoor N, Bahuguna N, Anand S. Influence of composite insertion technique on gap formation. J Conserv Dent 2016; 19 (01) 77-81
- 51 Al-Harbi F, Kaisarly D, Michna A, ArRejaie A, Bader D, El Gezawi M. Cervical interfacial bonding effectiveness of class II bulk versus incremental fill resin composite restorations. Oper Dent 2015; 40 (06) 622-635
- 52 Patel P, Desai MSNAP, Patel KTK. Comparative evaluation of microleakage of class II cavities restored with different bulk fill composite restorative systems: an in vitro study. J Res Adv Dent. 2016; 5: 52-62
- 53 Jawaed NU, Abidi SY, Qazi FU, Ahmed S. An in-vitro evaluation of microleakage at the cervical margin between two different class II restorative techniques using dye penetration method. J Coll Physicians Surg Pak 2016; 26 (09) 748-752
- 54 Webber MBF, Marin GC, Progiante PS, Lolli LF, Marson FC. Bulk fill resin based composites: microleakage of class II restorations. J Surg Clin Dent. 2014; 2: 15-19
- 55 Shadman N, Pezeshki B, Rostami S. Marginal sealing of bulk fill versus conventional composites in class II composite restorations: an in vitro study. Front Dent 2020; 17: 40
- 56 Baltacioğlu İH, Demirel G, Öztürk B, Aydin F, Orhan K. Marginal adaptation of bulk-fill resin composites with different viscosities in class II restorations: a micro-CT evaluation. BMC Oral Health 2024; 24 (01) 228
- 57 Dilian NS, Alaa K. Comparative evaluation of marginal microleakage between bulk-fill, preheated bulk-fill, and bulk-fill flowable composite resins above and below cemento-enamel junction using micro-computed tomography: an in vitro study. Dent Hypotheses 2022; 13: 128
- 58 Orłowski M, Tarczydło B, Chałas R. Evaluation of marginal integrity of four bulk-fill dental composite materials: in vitro study. ScientificWorldJournal 2015; 2015: 701262
- 59 Scotti N, Comba A, Gambino A. et al. Microleakage at enamel and dentin margins with a bulk fills flowable resin. Eur J Dent 2014; 8 (01) 1-8
Address for correspondence
Publication History
Article published online:
26 February 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Jia S, Chen D, Wang D, Bao X, Tian X. Comparing marginal microleakage of three different dental materials in veneer restoration using a stereomicroscope: an in vitro study. BDJ Open 2017; 3: 16010
- 2 El-Maksoud OA, Hamama H, Wafaie RA, El-Wassefy N, Mahmoud SH. Impact of refrigeration of different resin composite restorative materials on the marginal adaptation in class II restorations. BMC Oral Health 2024; 24 (01) 1174
- 3 Shih WY. Microleakage in different primary tooth restorations. J Chin Med Assoc 2016; 79 (04) 228-234
- 4 Pecie R, Onisor I, Krejci I, Bortolotto T. Marginal adaptation of direct class II composite restorations with different cavity liners. Oper Dent 2013; 38 (06) E210-E220
- 5 Punathil S, Almalki SA, AlJameel AH, Gowdar IM, Mc VA, Chinnari K. Assessment of microleakage using dye penetration method in primary teeth restored with tooth-colored materials: an in vitro study. J Contemp Dent Pract 2019; 20 (07) 778-782
- 6 Karaman E, Ozgunaltay G. Polymerization shrinkage of different types of composite resins and microleakage with and without liner in class II cavities. Oper Dent 2014; 39 (03) 325-331
- 7 Cobanoglu N, Ozer F, Demirci M, Erganis O, Imazato S. Bacterial penetration of restored cavities using two self-etching bonding systems. Eur J Dent 2014; 8 (02) 166-171
- 8 Cayo-Rojas CF, Hernández-Caba KK, Aliaga-Mariñas AS, Ladera-Castañeda MI, Cervantes-Ganoza LA. Microleakage in class II restorations of two bulk fill resin composites and a conventional nanohybrid resin composite: an in vitro study at 10,000 thermocycles. BMC Oral Health 2021; 21 (01) 619
- 9 Vetromilla BM, Opdam NJ, Leida FL. et al. Treatment options for large posterior restorations: a systematic review and network meta-analysis. J Am Dent Assoc 2020; 151 (08) 614-624.e18
- 10 Kimmel M, Faggion Jr CM. Systematic reviews comparing direct and indirect restorations: an umbrella review that examines restoration type and confidence in results. Clin Exp Dent Res 2025; 11 (03) e70149
- 11 Opdam N, Frankenberger R, Magne P. From “direct versus indirect” toward an integrated restorative concept in the posterior dentition. Oper Dent 2016; 41 (S7): S27-S34
- 12 Incekara MS, Karadas M. Clinical comparison of direct and indirect class II composite restorations: a prospective 12-month follow-up study. BMC Oral Health 2025; 25 (01) 1217
- 13 Josic U, D'Alessandro C, Miletic V. et al. Clinical longevity of direct and indirect posterior resin composite restorations: an updated systematic review and meta-analysis. Dent Mater 2023; 39 (12) 1085-1094
- 14 St-Pierre L, Bergeron C, Qian F. et al. Effect of polishing direction on the marginal adaptation of composite resin restorations. J Esthet Restor Dent 2013; 25 (02) 125-138
- 15 Karabela MM, Sideridou ID. Synthesis and study of properties of dental resin composites with different nanosilica particles size. Dent Mater 2011; 27 (08) 825-835
- 16 Moda MD, Briso AF, Hoshino I. et al. Three-year randomized prospective clinical trial of class II restorations using flowable bulk-fill resin composites. Oper Dent 2021; 46 (05) 516-528
- 17 Loguercio AD, Rezende M, Gutierrez MF, Costa TF, Armas-Vega A, Reis A. Randomized 36-month follow-up of posterior bulk-filled resin composite restorations. J Dent 2019; 85: 93-102
- 18 Wafaie RA, Ahmed B, Mahmoud SH. Fracture resistance of molars with class II MOD cavities restored with bulk-fill, no-cap flowable bulk-fill, and conventional resin composite restorative systems after 6-months water storage. BMC Oral Health 2025; 25 (01) 741
- 19 Gerula-Szymańska A, Kaczor K, Lewusz-Butkiewicz K, Nowicka A. Marginal integrity of flowable and packable bulk fill materials used for class II restorations—a systematic review and meta-analysis of in vitro studies. Dent Mater J 2020; 39 (03) 335-344
- 20 Tauböck TT, Marovic D, Zeljezic D, Steingruber AD, Attin T, Tarle Z. Genotoxic potential of dental bulk-fill resin composites. Dent Mater 2017; 33 (07) 788-795
- 21 Zorzin J, Maier E, Harre S. et al. Bulk-fill resin composites: polymerization properties and extended light curing. Dent Mater 2015; 31 (03) 293-301
- 22 Gamarra VSS, Borges GA, Júnior LHB, Spohr AM. Marginal adaptation and microleakage of a bulk-fill composite resin photopolymerized with different techniques. Odontology 2018; 106 (01) 56-63
- 23 Bucuta S, Ilie N. Light transmittance and micro-mechanical properties of bulk fill vs. conventional resin based composites. Clin Oral Investig 2014; 18 (08) 1991-2000
- 24 Yazici AR, Kutuk ZB, Ergin E, Karahan S, Antonson SA. Six-year clinical evaluation of bulk-fill and nanofill resin composite restorations. Clin Oral Investig 2022; 26 (01) 417-426
- 25 Atalay C, Yazici AR, Horuztepe A, Nagas E, Ertan A, Ozgunaltay G. Fracture resistance of endodontically treated teeth restored with bulk fill, bulk fill flowable, fiber-reinforced, and conventional resin composite. Oper Dent 2016; 41 (05) E131-E140
- 26 Ferracane JL. Resin composite—state of the art. Dent Mater 2011; 27 (01) 29-38
- 27 Sartawi SY, AbuSidu Z, El-Qawasmi Y, Salim NA. In vitro analysis of flowable and high viscosity bulk fill composite versus conventional composite in core build up of endodontically treated teeth. Sci Rep 2024; 14 (01) 28013
- 28 Khoramian Tusi S, Hamdollahpoor H, Mohammadi Savadroodbari M, Sheikh Fathollahi M. Comparison of polymerization shrinkage of a new bulk-fill flowable composite with other composites: an in vitro study. Clin Exp Dent Res 2022; 8 (06) 1605-1613
- 29 Ujiie M, Tsujimoto A, Barkmeier WW. et al. Comparison of occlusal wear between bulk-fill and conventional flowable resin composites. Am J Dent 2020; 33 (02) 74-78
- 30 Sadek FT, Moura SK, Ballester RY, Muench A, Cardoso PE. The effect of long-term storage on the microleakage of composite resin restorations: qualitative and quantitative evaluation. Pesqui Odontol Bras 2003; 17 (03) 261-266
- 31 Moorthy A, Hogg CH, Dowling AH, Grufferty BF, Benetti AR, Fleming GJ. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J Dent 2012; 40 (06) 500-505
- 32 Tomaszewska IM, Kearns JO, Ilie N, Fleming GJ. Bulk fill restoratives: to cap or not to cap—that is the question?. J Dent 2015; 43 (03) 309-316
- 33 Rengo C, Spagnuolo G, Ametrano G. et al. Marginal leakage of bulk-fill composites in class II restorations: a microCT and digital microscope analysis. Int J Adhes Adhes 2015; 60: 123-129
- 34 Sahli A, Daeniker L, Rossier I. et al. Comparison of class II bulk-fill, self-adhesive composites, alkasite, and high-viscosity glass ionomer restorations in terms of marginal and internal adaptation. Materials (Basel) 2024; 17 (17) 4373
- 35 Şenol AA, Karabulut Gençer B, Tarçın B, Kahramanoğlu E, Yılmaz Atalı P. Microleakage and marginal integrity of ormocer/methacrylate-based bulk-fill resin restorations in MOD cavities: SEM and stereomicroscopic evaluation. Polymers (Basel) 2023; 15 (07) 1716
- 36 Kalmowicz J, Phebus JG, Owens BM, Johnson WW, King GT. Microleakage of class I and II composite resin restorations using a sonic-resin placement system. Oper Dent 2015; 40 (06) 653-661
- 37 García Marí L, Climent Gil A, LLena Puy C. In vitro evaluation of microleakage in class II composite restorations: high-viscosity bulk-fill vs conventional composites. Dent Mater J 2019; 38 (05) 721-727
- 38 Pushpa R, Suresh BS. Marginal permeability of one step self-etch adhesives: effects of double application or the application of hydrophobic layer. J Conserv Dent 2010; 13 (03) 141-144
- 39 Poggio C, Chiesa M, Scribante A, Mekler J, Colombo M. Microleakage in class II composite restorations with margins below the CEJ: in vitro evaluation of different restorative techniques. Med Oral Patol Oral Cir Bucal 2013; 18 (05) e793-e798
- 40 Çağırır Dindaroğlu F, Yılmaz E. Two-year evaluation of a nano-hybrid and a bulk-fill resin composite: a randomized, double-blind split-mouth clinical study. Clin Oral Investig 2024; 28 (04) 208
- 41 de Assis FS, Lima SN, Tonetto MR. et al. Evaluation of bond strength, marginal integrity, and fracture strength of bulk- vs incrementally-filled restorations. J Adhes Dent 2016; 18 (04) 317-323
- 42 Ahmed B, El-Maksoud OA, Wafaie RA, Mahmoud SH. Effect of short dentin etching and water storage on bonding of resin composite to dentin with universal and two-step self-etch adhesive systems. Sci Rep 2025; 15 (01) 43817
- 43 Ernst CP, Galler P, Willershausen B, Haller B. Marginal integrity of class V restorations: SEM versus dye penetration. Dent Mater 2008; 24 (03) 319-327
- 44 Ozel E, Korkmaz Y, Attar N. Influence of location of the gingival margin on the microleakage and internal voids of nanocomposites. J Contemp Dent Pract 2008; 9 (07) 65-72
- 45 AlHabdan AA. Review of microleakage evaluation tools. J Int Oral Health 2017; 9: 141-145
- 46 Sawani S, Arora V, Jaiswal S, Nikhil V. Comparative evaluation of microleakage in class II restorations using open vs. closed centripetal build-up techniques with different lining materials. J Conserv Dent 2014; 17 (04) 344-348
- 47 Saboia VP, Silva FC, Nato F. et al. Analysis of differential artificial ageing of the adhesive interface produced by a two-step etch-and-rinse adhesive. Eur J Oral Sci 2009; 117 (05) 618-624
- 48 Coelho-De-Souza FH, Camacho GB, Demarco FF, Powers JM. Fracture resistance and gap formation of MOD restorations: influence of restorative technique, bevel preparation and water storage. Oper Dent 2008; 33 (01) 37-43
- 49 Parra Gatica E, Duran Ojeda G, Wendler M. Contemporary flowable bulk-fill resin-based composites: a systematic review. Biomater Investig Dent 2023; 10 (01) 8-19
- 50 Kapoor N, Bahuguna N, Anand S. Influence of composite insertion technique on gap formation. J Conserv Dent 2016; 19 (01) 77-81
- 51 Al-Harbi F, Kaisarly D, Michna A, ArRejaie A, Bader D, El Gezawi M. Cervical interfacial bonding effectiveness of class II bulk versus incremental fill resin composite restorations. Oper Dent 2015; 40 (06) 622-635
- 52 Patel P, Desai MSNAP, Patel KTK. Comparative evaluation of microleakage of class II cavities restored with different bulk fill composite restorative systems: an in vitro study. J Res Adv Dent. 2016; 5: 52-62
- 53 Jawaed NU, Abidi SY, Qazi FU, Ahmed S. An in-vitro evaluation of microleakage at the cervical margin between two different class II restorative techniques using dye penetration method. J Coll Physicians Surg Pak 2016; 26 (09) 748-752
- 54 Webber MBF, Marin GC, Progiante PS, Lolli LF, Marson FC. Bulk fill resin based composites: microleakage of class II restorations. J Surg Clin Dent. 2014; 2: 15-19
- 55 Shadman N, Pezeshki B, Rostami S. Marginal sealing of bulk fill versus conventional composites in class II composite restorations: an in vitro study. Front Dent 2020; 17: 40
- 56 Baltacioğlu İH, Demirel G, Öztürk B, Aydin F, Orhan K. Marginal adaptation of bulk-fill resin composites with different viscosities in class II restorations: a micro-CT evaluation. BMC Oral Health 2024; 24 (01) 228
- 57 Dilian NS, Alaa K. Comparative evaluation of marginal microleakage between bulk-fill, preheated bulk-fill, and bulk-fill flowable composite resins above and below cemento-enamel junction using micro-computed tomography: an in vitro study. Dent Hypotheses 2022; 13: 128
- 58 Orłowski M, Tarczydło B, Chałas R. Evaluation of marginal integrity of four bulk-fill dental composite materials: in vitro study. ScientificWorldJournal 2015; 2015: 701262
- 59 Scotti N, Comba A, Gambino A. et al. Microleakage at enamel and dentin margins with a bulk fills flowable resin. Eur J Dent 2014; 8 (01) 1-8