

Subscribe to RSS
DOI: 10.1055/s-0046-1816582
Diagnostic Performance of ROMA and Biomarkers in Ovarian Cancer: A Systematic Review of Sensitivity, Specificity, and Menopausal Influence
Authors

Abstract
Ovarian cancer is a leading cause of gynecological cancer mortality. Despite the widespread use of cancer antigen 125 (CA125), its sensitivity for early-stage detection is limited. This review evaluates the diagnostic accuracy of CA125, Human epididymis protein 4 (HE4), Risk of Ovarian Malignancy Algorithm (ROMA), and the Assessment of Different Neoplasia's in the adneXa (ADNEX) model in distinguishing benign from malignant ovarian masses. A systematic review was conducted using PubMed, Embase, and Scopus, selecting studies published up to June 2025. Studies were included if they provided data on the diagnostic accuracy of HE4, CA125, ROMA, or ADNEX in women with pelvic masses. A total of seven studies met the inclusion criteria. ROMA demonstrated high diagnostic performance, with sensitivity ranging from 64.8 to 93.75% and specificity from 72.8 to 94.9%, particularly in postmenopausal women. Although CA125 showed a sensitivity of 85.07% in one study, several other studies reported higher sensitivity for ROMA, particularly in postmenopausal women, as well as higher specificity (92.31%). HE4 exhibited very high specificity (up to 97.87%) but demonstrated variable sensitivity across studies, outperforming ROMA in some cohorts, such as Montagnana et al. ROMA performed comparably to Risk of Malignancy Index (RMI) in some studies, although RMI demonstrated slightly higher overall accuracy in Anton et al and outperformed CA125 in several studies. The ADNEX model showed higher sensitivity (91.9%) but lower specificity (65.7%) compared with ROMA. ROMA is a valuable diagnostic tool, especially in postmenopausal women, offering better diagnostic accuracy than CA125 alone, with sensitivity as high as 93.75% and specificity up to 94.9%. However, its sensitivity in premenopausal women is limited. Further research is needed to optimize ROMA's cutoff values and improve its integration with other diagnostic methods.
Introduction
Ovarian cancer is a leading cause of gynecological cancer mortality worldwide, representing a significant clinical challenge due to its late presentation and poor prognosis.[1] Globally, more than 310,000 new cases and over 200,000 deaths are reported annually, with the majority of women presenting at advanced stages of the disease.[1] [2] The 5-year survival rate for advanced ovarian cancer remains below 30%, in stark contrast to over 90% for early-stage disease, underscoring the critical importance of early detection.[2] [3]
Despite decades of research, effective screening strategies for ovarian cancer remain elusive. The most widely used serum biomarker, cancer antigen 125 (CA125), was first described in the 1980s and has since become a cornerstone in the diagnosis and monitoring of ovarian cancer.[4] However, CA125 is limited by its lack of sensitivity for early-stage disease—being elevated in only ∼50% of stage I cases—and by its poor specificity, as levels can rise in a variety of benign gynecological and non-gynecological conditions such as endometriosis, menstruation, and liver disease.[4] [5] [6]
In response to these limitations, the search for novel biomarkers and improved diagnostic algorithms has intensified. Human epididymis protein 4 (HE4) emerged as a promising biomarker in the early 2000s, demonstrating higher specificity than CA125, particularly in premenopausal women and in patients with benign conditions that can elevate CA125.[5] [7] HE4 is overexpressed in serous and endometrioid ovarian carcinomas, but rarely in benign gynecological diseases, making it a valuable addition to the diagnostic arsenal.[5] [8]
Recognizing the complementary strengths of CA125 and HE4, Moore et al introduced the Risk of Ovarian Malignancy Algorithm (ROMA), which combines both biomarkers with menopausal status to generate a composite risk score.[4] The ROMA algorithm calculates separate logistic regression equations for premenopausal and postmenopausal women, thereby accommodating the biological differences in marker expression. Numerous validation studies have since demonstrated that ROMA outperforms either CA125 or HE4 alone in distinguishing malignant from benign pelvic masses, particularly in postmenopausal women.[3] [4]
Parallel to advances in serum biomarkers, imaging-based risk models have also evolved. The International Ovarian Tumor Analysis (IOTA) group has developed a series of ultrasound-based models, culminating in the Assessment of Different Neoplasia's in the adneXa (ADNEX) model.[3] The ADNEX model integrates clinical, ultrasound, and biomarker data (including CA125) to estimate the risk of benign, borderline, early-stage invasive, advanced-stage invasive, and secondary metastatic ovarian tumors. In a large, prospective, multicenter study, the ADNEX model demonstrated high diagnostic accuracy, with an area under the receiver operating characteristic curve (AUC) exceeding 0.90 for differentiating malignant from benign adnexal masses.[3]
The clinical application of these biomarkers and algorithms is crucial for optimizing patient triage, surgical planning, and referral to gynecologic oncologists. International guidelines, such as those from the American College of Obstetricians and Gynecologists and the European Society for Medical Oncology, increasingly recommend the use of multimodal risk assessment tools, combining serum biomarkers with imaging findings.[3] [6]
However, there remains considerable variability in the reported diagnostic performance of these tools across different populations and clinical settings. Factors such as disease prevalence, patient demographics, and the prevalence of benign conditions that can elevate CA125 or HE4 may influence sensitivity, specificity, and predictive values.[3] [6] Moreover, the optimal cutoff values for these algorithms may differ by population, necessitating local validation and calibration.[3] [7]
Given the rapidly evolving landscape of ovarian cancer diagnostics and the proliferation of new biomarkers and algorithms, there is a pressing need for systematic reviews and comparative studies that synthesize the latest evidence and provide clear guidance for clinicians.[6] [8] Such research is essential for clarifying the relative strengths and limitations of each approach, informing clinical decision-making, and identifying areas for future investigation.
This article aims to provide a comprehensive synthesis of the current evidence regarding the diagnostic accuracy of CA125, HE4, ROMA, and the ADNEX model in women with pelvic or adnexal masses. By systematically comparing these biomarkers and algorithms across multiple studies and populations, we seek to clarify their relative diagnostic performance, inform clinical practice, and highlight priorities for future research.
Methodology
The methodology for this systematic review involved a comprehensive and structured approach to identify, select, and synthesize studies evaluating ovarian cancer biomarkers and diagnostic algorithms. A systematic literature search was performed across major biomedical databases, including PubMed, Embase, and Scopus, using keywords such as “ovarian cancer,” “HE4,” “CA125,” “ROMA,” and “ADNEX,” with the search limited to studies published up to June 2025. Studies were eligible for inclusion if they evaluated the diagnostic accuracy of HE4, CA125, ROMA, or the ADNEX model in women with pelvic or adnexal masses and provided sufficient data to calculate sensitivity, specificity, or AUC, with histopathological diagnosis or standardized clinical/imaging follow-up as the reference standard.
Studies were excluded if they focused solely on nonepithelial ovarian tumors, lacked sufficient diagnostic accuracy data, or were reviews, editorials, case reports, or conference abstracts. Two reviewers independently screened titles and abstracts, assessed full texts for eligibility, and extracted data on study design, patient characteristics, biomarkers or algorithms tested, diagnostic thresholds, reference standards, and reported measures of diagnostic performance. Disagreements were resolved by consensus or consultation with a third reviewer. After full-text assessment, seven studies met all inclusion criteria and were selected for final analysis. These studies included Montagnana et al, Wei et al, Tangjanyatham and Chaowawanit, Park et al, and three additional studies detailed in the review.
These selected studies included both prospective and retrospective designs, with sample sizes ranging from 104 to 443 women, and all used histopathological confirmation or standardized clinical follow-up as the reference standard. The search for studies was conducted across multiple databases, including PubMed, Scopus, and EMBASE, for publications between 2009 and 2025. Keywords such as “Risk of Ovarian Malignancy Algorithm,” “ROMA ovarian cancer diagnosis,” and “biomarkers” were combined with terms like “CA125,” “HE4,” and “RMI” using Boolean operators AND OR. For example, a typical search string used in PubMed was: (“ROMA” OR “Risk of Ovarian Malignancy Algorithm”) AND (“CA125” OR “HE4” OR “RMI”) AND (“diagnosis” OR “sensitivity” OR “specificity”).
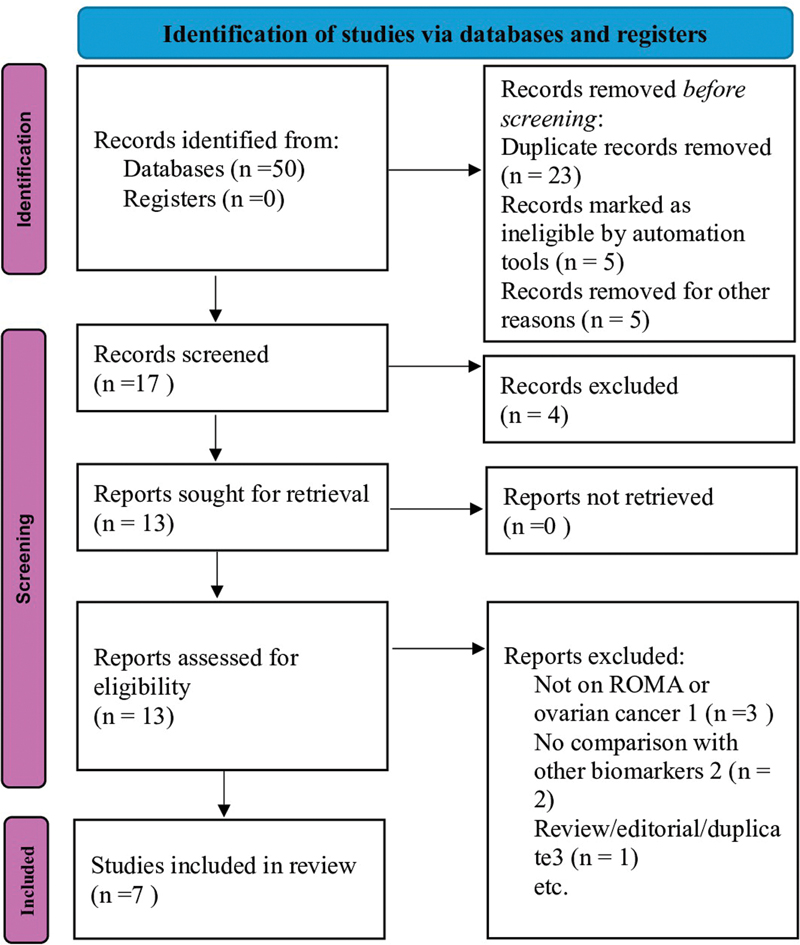
The search strategy was designed to capture studies focusing on the diagnostic accuracy of ROMA for ovarian cancer detection. A PRISMA ([Fig. 1]) flow diagram was used to track the study selection process, showing how many studies were retrieved, screened, excluded, and included. For data extraction, two independent reviewers collected key information, including study design, sample size, ROMA's sensitivity and specificity, and comparison with other biomarkers. Disagreements during data extraction were resolved through discussion to ensure consistency and accuracy. Studies not published in English or lacking peer-reviewed credibility were excluded. The Newcastle–Ottawa Scale was used by the reviewers to assess the risk of bias in included studies. Discrepancies in quality scoring were resolved by consensus. Due to heterogeneity in study designs, populations, and diagnostic thresholds, a qualitative synthesis was performed, summarizing and comparing the diagnostic performance of HE4, CA125, ROMA, and ADNEX, with particular attention to differences by menopausal status and the impact of cutoff adjustments. This review utilized only published data; therefore, no ethical approval was required for this synthesis, as the primary studies obtained ethical approval in accordance with institutional and international guidelines.
Results
The results of this systematic review highlight the effectiveness and limitations of ROMA in diagnosing ovarian cancer, particularly in postmenopausal women. ROMA combines two biomarkers, HE4 and CA125, and has been widely studied for its ability to differentiate malignant from benign ovarian masses. One of the most significant findings comes from the study by Montagnana et al, which assessed ROMA's diagnostic performance in postmenopausal women.[9] The study demonstrated that ROMA had a diagnostic AUC of 0.92, making it more accurate than CA125 alone, which had a sensitivity of 85.07% and a specificity of 92.31%. Although HE4 alone had a slightly higher AUC (0.94), ROMA proved to be more accurate in distinguishing postmenopausal women at high risk for epithelial ovarian cancer. However, in premenopausal women, ROMA did not outperform HE4, as both ROMA and HE4 had AUCs of 0.77, showing that ROMA's performance in younger women is less reliable.
In a follow-up study, Wei et al found that ROMA demonstrated a sensitivity of 93.75% and a specificity of 92.55%, outperforming CA125 in diagnostic accuracy.[10] CA125 alone had a sensitivity of 85.07%, highlighting ROMA's role as a more reliable method when used in conjunction with HE4 for distinguishing between benign and malignant ovarian masses. This is particularly important in clinical settings where rapid diagnosis is crucial. The study underscores the value of ROMA as a highly reliable method for detecting ovarian cancer, reinforcing its use in mixed clinical populations, although the study did not stratify results by menopausal status.
A traffic light plot ([Fig. 2]) illustrates the risk of bias across the seven studies evaluating ROMA and comparator biomarkers. Judgments were made across six domains, with green representing low risk, yellow indicating some concerns, and red (not present here) indicating high risk.

A major comparison to ROMA is the ADNEX model, which was evaluated by Tangjanyatham and Chaowawanit. In their analysis, ADNEX demonstrated higher sensitivity (91.9 vs. 64.8%), whereas ROMA showed higher specificity (86.3 vs. 65.7%), making ROMA a more accurate tool for ruling out benign conditions. The ADNEX model includes additional diagnostic parameters, such as ultrasound findings and serum markers, and has been shown to be a better predictor of ovarian malignancy in complex cases, such as adnexal masses, where ultrasound findings are inconclusive. Despite ADNEX's higher sensitivity, ROMA remains an essential tool in settings where ultrasound expertise may not be readily available or when a rapid diagnostic assessment is needed.[11]
In contrast, Anton et al conducted a study comparing ROMA with Risk of Malignancy Index (RMI) and CA125 in a cohort of 128 patients. They found that ROMA had comparable sensitivity (74.1%) to RMI (74.1%) in distinguishing benign from malignant ovarian masses.[12] However, RMI was slightly more accurate overall, showcasing the competitive performance of ROMA against other established models. ROMA was found to slightly outperform CA125 in patients with complex ovarian tumors, providing evidence of its diagnostic accuracy even in complicated clinical scenarios. The study concluded that both ROMA and RMI had similar performances, but ROMA remains valuable when used alongside HE4.
One of ROMA's key strengths is its ability to provide separate diagnostic models for pre- and post-menopausal women, addressing hormonal differences that significantly influence HE4 and CA125 levels. Studies have consistently shown that ROMA performs better in postmenopausal women, where its diagnostic accuracy is significantly higher. Park et al conducted a clinical study in Korea, where ROMA achieved a sensitivity of 88.9% and a specificity of 94.9% for postmenopausal women. However, for premenopausal women, ROMA's sensitivity decreased, with the study highlighting the need for adjusted cutoffs to improve diagnostic accuracy in younger women.[13] This finding reinforces the importance of tailoring diagnostic models to the patient population, especially considering the variation in menopausal status.
Several studies, including Lee et al, compared ROMA with CA125 and HE4 for early-stage ovarian cancer detection. ROMA showed relatively improved performance for endometriotic-type ovarian tumors, although overall sensitivity for early-stage disease remained modest, whereas CA125 alone demonstrated low sensitivity. CA125 demonstrated a sensitivity of 93.5% for distinguishing malignant tumors, whereas ROMA, when combined with HE4, demonstrated superior sensitivity and specificity.[14] These findings suggest that ROMA is a more reliable diagnostic tool for certain subtypes, particularly in tumors with low malignant potential.
However, ROMA also has notable limitations. A significant drawback is its lower sensitivity in premenopausal women, where it showed only 53.3% sensitivity, compared with 82.5% in postmenopausal women. This discrepancy highlights the challenge of using ROMA for diagnosing ovarian cancer in younger women, where benign conditions like endometriosis and fibroids often present similarly to malignant tumors. Additionally, Ngu et al demonstrated that in cases where IOTA ultrasound rules were inconclusive, expert ultrasound outperformed ROMA in diagnosing malignant ovarian masses, with 81% sensitivity compared with ROMA's 63%. This suggests that ROMA may not entirely replace expert imaging, particularly in cases where clinical judgment and imaging play critical roles.[15]
Finally, ROMA's performance varies depending on tumor subtype. According to Lee et al, ROMA demonstrated relatively improved performance for endometriotic-type tumors, although overall sensitivity remained limited, where CA125 had low sensitivity. However, ROMA's performance in other tumor subtypes,[14] such as serous and clear cell carcinomas, was similar to that of HE4, indicating that ROMA may be most beneficial for specific subtypes but may require further refinement for broader tumor classifications ([Table 1]).
|
Study |
Target group |
ROMA sensitivity (%) |
ROMA specificity (%) |
CA125 sensitivity (%) |
CA125 specificity (%) |
HE4 sensitivity (%) |
HE4 specificity (%) |
RMI sensitivity (%) |
RMI specificity (%) |
Key comparison |
Key statistical findings |
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Montagnana et al (2011)[9] |
Postmenopausal |
82.5 |
85 |
84 |
73 |
94 |
88 |
ROMA HE4 > ROMA > CA125 |
ROMA AUC: 0.92; HE4 AUC: 0.94; CA125 AUC: 0.84 (postmenopausal) |
||
|
Wei et al (2016)[10] |
All groups |
93.8 |
93 |
85.1 |
92 |
75 |
98 |
ROMA > HE4 > CA125 |
ROMA AUC: 0.994; HE4 AUC: 0.990; CA125 AUC: 0.941 |
||
|
Tangjanyatham and Chaowawanit (2025)[11] |
Women with adnexal masses |
64.8 |
86 |
86.5 |
91 |
78.4 |
97 |
ADNEX more sensitive, ROMA more specific |
ADNEX AUC: 0.83 vs. ROMA AUC: not reported; ADNEX sensitivity: 91.9% |
||
|
Park et al (2019)[13] |
Clinical practice (low-prevalence) |
77.8 |
89 |
70.4 |
74 |
79.6 |
67 |
63 |
92.4 |
Adjusted ROMA improves sensitivity |
Adjusted ROMA cutoffs improved sensitivity to 88.9% |
|
Lee et al (2020)[14] |
Early-stage tumors |
47.3 |
53 |
58.2 |
47 |
23.1 |
77 |
ROMA only better for endometriotic subtype |
ROMA more effective in endometriotic tumors only |
||
|
Anton et al (2012)[12] |
Mixed ovarian masses |
74.1 |
76 |
70.4 |
74 |
79.6 |
67 |
63 |
92.4 |
No single test superior; RMI most accurate |
RMI AUC: 0.861 vs. ROMA AUC: 0.824; all methods statistically similar |
|
Ngu et al (2022)[15] |
Inconclusive IOTA |
63 |
73 |
81.5 |
85 |
76.4 |
84 |
66.5 |
91.1 |
Expert US > ROMA in sensitivity |
Expert US sensitivity: 81% vs. ROMA: 63%; specificity ∼72% for both |
Abbreviations: ADNEX, Assessment of Different Neoplasia's in the adneXa; AUC, area under the receiver operating characteristic curve; CA125, cancer antigen 125; HE4, Human epididymis protein 4; IOTA, International Ovarian Tumor Analysis; RMI, Risk of Malignancy Index; ROMA, Risk of Ovarian Malignancy Algorithm; US, ultrasound.
In conclusion, ROMA is a valuable diagnostic tool for assessing ovarian cancer risk, especially in postmenopausal women. It demonstrates high sensitivity and specificity when combined with HE4 and CA125, particularly in differentiating malignant from benign ovarian masses. However, its utility is limited in premenopausal women, where sensitivity is lower, and in cases where initial imaging results are inconclusive. Further research into optimized cutoff values, tailored approaches based on menopausal status and tumor subtypes, and the potential for combined diagnostic strategies could enhance ROMA's overall diagnostic utility in ovarian cancer detection ([Table 2]).
|
Study |
Population/group |
ROMA sensitivity/specificity (%) |
CA125 sensitivity/specificity (%) |
HE4 sensitivity/specificity (%) |
Comparator model (sensitivity/specificity) |
Key findings |
|---|---|---|---|---|---|---|
|
Montagnana et al (2011)[9] |
Pre- and postmenopausal women with pelvic masses |
Pre: 53.3/80.6 Post: 82.5/85 |
Pre: 64/– Post: 84/73 |
Pre: 77/– Post: 94/88 |
– |
HE4 slightly superior to ROMA; ROMA performs well only in postmenopausal women |
|
Wei et al (2016)[10] |
Mixed clinical population |
93.8/93 |
85.1/92 |
75/98 |
– |
ROMA outperformed CA125 and HE4; highest diagnostic accuracy in the study |
|
Tangjanyatham and Chaowawanit (2025)[11] |
Women with adnexal masses |
64.8/86.3 |
86.5/91 |
78.4/97 |
ADNEX: 91.9/65.7 |
ADNEX more sensitive; ROMA more specific |
|
Park et al (2019)[13] |
Pre- and postmenopausal women in clinical practice |
Pre: lower Post: 88.9/94.9 |
70.4/74 |
79.6/67 |
RMI: 63/92.4 |
Adjusted ROMA cutoffs improved sensitivity in postmenopausal women |
|
Lee et al (2020)[14] |
Early-stage tumor subtypes |
47.3/53 |
58.2/47 |
23.1/77 |
– |
ROMA superior only in endometriotic tumors; limited early-stage utility |
|
Anton et al (2012)[12] |
Mixed ovarian masses |
74.1/76 |
70.4/74 |
79.6/67 |
RMI: 63/92.4 |
RMI slightly more accurate; ROMA comparable but not superior |
|
Ngu et al (2020)[15] |
Inconclusive IOTA ultrasound cases |
63/73 |
81.5/85 |
76.4/84 |
RMI: 66.5/91.1 Expert US: 81% sens |
Expert ultrasound outperformed ROMA in sensitivity |
Abbreviations: ADNEX, Assessment of Different Neoplasia's in the adneXa; CA125, cancer antigen 125; HE4, Human epididymis protein 4; IOTA, International Ovarian Tumor Analysis; RMI, Risk of Malignancy Index; ROMA, Risk of Ovarian Malignancy Algorithm; US, ultrasound.
Discussion
Ovarian cancer remains one of the deadliest gynecological malignancies, and early detection is essential for improving patient outcomes.[16] [17] This systematic review demonstrates that ROMA provides clinically meaningful diagnostic stratification, particularly in postmenopausal women, when compared with CA125 alone.
Several studies included in this review consistently indicate that ROMA offers improved diagnostic discrimination over single-marker approaches, reflecting the complementary biological roles of HE4 and CA125.[18] [19] Rather than repeating numerical performance metrics, the present discussion focuses on the clinical interpretation of these findings. ROMA appears especially useful as a triage tool for identifying patients who may benefit from referral to gynecologic oncology services, particularly in postmenopausal populations where ovarian cancer prevalence is higher.
Comparative analyses with other diagnostic models suggest that ROMA and imaging-based approaches such as the ADNEX model serve complementary roles. While ADNEX demonstrates higher sensitivity in some cohorts, ROMA shows stronger specificity, which may reduce unnecessary surgical interventions for benign disease, particularly in settings where advanced ultrasound expertise is not readily available. Similarly, ROMA demonstrates performance comparable to RMI, supporting its role as an alternative or adjunct diagnostic strategy in clinical practice.[12] [20]
Menopausal status remains a key determinant of ROMA's diagnostic utility. Across multiple studies, ROMA consistently performs better in postmenopausal women than in premenopausal women, likely due to hormonal influences on biomarker expression and the higher prevalence of benign conditions such as endometriosis in younger patients. These findings highlight the importance of population-specific interpretation and the potential need for adjusted cutoff values.
Despite its clinical value, ROMA should not be considered a replacement for expert ultrasound assessment, particularly in complex or inconclusive cases. Instead, the evidence supports its use as part of a multimodal diagnostic strategy integrating serum biomarkers, imaging findings, and clinical judgement.
Limitations
This systematic review has several limitations that should be acknowledged. First, substantial heterogeneity was observed among the included studies with respect to study design, patient populations, menopausal status, and diagnostic cutoff values for CA125, HE4, and ROMA, which limits direct comparability of results. Second, the relatively small number of eligible studies, reflecting strict inclusion criteria, may reduce the generalizability of the findings. Third, a quantitative meta-analysis could not be performed due to methodological heterogeneity and incomplete reporting of diagnostic accuracy metrics, and therefore, the findings were synthesized qualitatively. Finally, variability in assay methods and population-specific cutoff thresholds may have influenced reported sensitivity and specificity values. These limitations highlight the need for larger, well-designed prospective studies with standardized methodologies and population-specific validation of diagnostic algorithms.
Conclusion
ROMA represents a valuable diagnostic tool for assessing ovarian cancer risk, particularly in postmenopausal women, where its diagnostic performance is highest. When used alongside HE4 and CA125, ROMA supports more accurate differentiation between benign and malignant ovarian masses. However, its reduced sensitivity in premenopausal women and reliance on appropriate cutoff values underscore the need for cautious interpretation. Future research should focus on optimizing diagnostic thresholds and integrating ROMA within multimodal diagnostic pathways to enhance early detection across diverse patient populations.
Conflict of Interest
None declared.
-
References
- 1 Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- 2 Torre LA, Trabert B, DeSantis CE. et al. Ovarian cancer statistics, 2018. CA Cancer J Clin 2018; 68 (04) 284-296
- 3 Van Gorp T, Cadron I, Despierre E. et al. HE4 and CA125 as a diagnostic test in ovarian cancer: prospective validation of the Risk of Ovarian Malignancy Algorithm. Br J Cancer 2011; 104 (05) 863-870
- 4 Jacobs I, Oram D, Fairbanks J, Turner J, Frost C, Grudzinskas JG. A risk of malignancy index incorporating CA 125, ultrasound and menopausal status for the accurate preoperative diagnosis of ovarian cancer. Br J Obstet Gynaecol 1990; 97 (10) 922-929
- 5 Moore RG, Brown AK, Miller MC. et al. The use of multiple novel tumor biomarkers for the detection of ovarian carcinoma in patients with a pelvic mass. Gynecol Oncol 2008; 108 (02) 402-408
- 6 Kaijser J. Towards an evidence-based approach for diagnosis and management of adnexal masses: findings of the International Ovarian Tumour Analysis (IOTA) studies. Facts Views Vis ObGyn 2015; 7 (01) 42-59
- 7 Moore RG, Miller MC, Eklund EE, Lu KH, Bast Jr RC, Lambert-Messerlian G. Serum levels of the ovarian cancer biomarker HE4 are decreased in pregnancy and increase with age. Am J Obstet Gynecol 2012; 206 (04) 349.e1-349.e7
- 8 Van Calster B, Van Hoorde K, Valentin L. et al; International Ovarian Tumour Analysis Group. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: prospective multicentre diagnostic study. BMJ 2014; 349: g5920
- 9 Montagnana M, Danese E, Ruzzenente O. et al. The ROMA (Risk of Ovarian Malignancy Algorithm) for estimating the risk of epithelial ovarian cancer in women presenting with pelvic mass: is it really useful?. Clin Chem Lab Med 2011; 49 (03) 521-525
- 10 Wei SU, Li H, Zhang B. The diagnostic value of serum HE4 and CA-125 and ROMA index in ovarian cancer. Biomed Rep 2016; 5 (01) 41-44
- 11 Tangjanyatham P, Chaowawanit W. Comparison of sensitivity for Risk of Ovarian Malignancy Algorithm (ROMA) and Assessment of Different NEoplasias in the adneXa (ADNEX) model for predicting ovarian cancer in a woman with adnexal masses. Int J Gynecol Cancer 2025; 35 (06) 101827
- 12 Anton C, Carvalho FM, Oliveira EI, Maciel GA, Baracat EC, Carvalho JP. A comparison of CA125, HE4, risk ovarian malignancy algorithm (ROMA), and risk malignancy index (RMI) for the classification of ovarian masses. Clinics (Sao Paulo) 2012; 67 (05) 437-441
- 13 Park H, Shin JE, Lee DW, Kim MJ, Lee HN. Diagnostic accuracy of the risk of ovarian malignancy algorithm in clinical practice at a single hospital in Korea. Ann Lab Med 2019; 39 (03) 252-262
- 14 Lee YJ, Kim YM, Kang JS, Nam SH, Kim DY, Kim YT. Comparison of Risk of Ovarian Malignancy Algorithm and cancer antigen 125 to discriminate between benign ovarian tumor and early-stage ovarian cancer according to imaging tumor subtypes. Oncol Lett 2020; 20 (01) 931-938
- 15 Ngu SF, Chai YK, Choi KM. et al. Diagnostic Performance of Risk of Malignancy Algorithm (ROMA), Risk of Malignancy Index (RMI) and Expert Ultrasound Assessment in a Pelvic Mass Classified as Inconclusive by International Ovarian Tumour Analysis (IOTA) Simple Rules. Cancers (Basel) 2022; 14 (03) 810
- 16 Allison KH, Hammond MEH, Dowsett M. et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP guideline update. J Clin Oncol 2020; 38 (12) 1346-1366
- 17 Wang J, Wang B, Li C. et al. Evolving global trends in PCOS burden: a three-decade analysis (1990-2021) with projections to 2036 among adolescents and young adults. Front Endocrinol (Lausanne) 2025; 16: 1569694
- 18 Kim B, Park Y, Kim B. et al. Diagnostic performance of CA 125, HE4, and risk of Ovarian Malignancy Algorithm for ovarian cancer. J Clin Lab Anal 2019; 33 (01) e22624
- 19 Hsu ST, Su YJ, Hung CH, Chen MJ, Lu CH, Kuo CE. Automatic ovarian tumors recognition system based on ensemble convolutional neural network with ultrasound imaging. BMC Med Inform Decis Mak 2022; 22 (01) 298
- 20 Jacobs I, Bast Jr RC. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod 1989; 4 (01) 1-12
Address for correspondence
Publication History
Article published online:
16 February 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- 2 Torre LA, Trabert B, DeSantis CE. et al. Ovarian cancer statistics, 2018. CA Cancer J Clin 2018; 68 (04) 284-296
- 3 Van Gorp T, Cadron I, Despierre E. et al. HE4 and CA125 as a diagnostic test in ovarian cancer: prospective validation of the Risk of Ovarian Malignancy Algorithm. Br J Cancer 2011; 104 (05) 863-870
- 4 Jacobs I, Oram D, Fairbanks J, Turner J, Frost C, Grudzinskas JG. A risk of malignancy index incorporating CA 125, ultrasound and menopausal status for the accurate preoperative diagnosis of ovarian cancer. Br J Obstet Gynaecol 1990; 97 (10) 922-929
- 5 Moore RG, Brown AK, Miller MC. et al. The use of multiple novel tumor biomarkers for the detection of ovarian carcinoma in patients with a pelvic mass. Gynecol Oncol 2008; 108 (02) 402-408
- 6 Kaijser J. Towards an evidence-based approach for diagnosis and management of adnexal masses: findings of the International Ovarian Tumour Analysis (IOTA) studies. Facts Views Vis ObGyn 2015; 7 (01) 42-59
- 7 Moore RG, Miller MC, Eklund EE, Lu KH, Bast Jr RC, Lambert-Messerlian G. Serum levels of the ovarian cancer biomarker HE4 are decreased in pregnancy and increase with age. Am J Obstet Gynecol 2012; 206 (04) 349.e1-349.e7
- 8 Van Calster B, Van Hoorde K, Valentin L. et al; International Ovarian Tumour Analysis Group. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: prospective multicentre diagnostic study. BMJ 2014; 349: g5920
- 9 Montagnana M, Danese E, Ruzzenente O. et al. The ROMA (Risk of Ovarian Malignancy Algorithm) for estimating the risk of epithelial ovarian cancer in women presenting with pelvic mass: is it really useful?. Clin Chem Lab Med 2011; 49 (03) 521-525
- 10 Wei SU, Li H, Zhang B. The diagnostic value of serum HE4 and CA-125 and ROMA index in ovarian cancer. Biomed Rep 2016; 5 (01) 41-44
- 11 Tangjanyatham P, Chaowawanit W. Comparison of sensitivity for Risk of Ovarian Malignancy Algorithm (ROMA) and Assessment of Different NEoplasias in the adneXa (ADNEX) model for predicting ovarian cancer in a woman with adnexal masses. Int J Gynecol Cancer 2025; 35 (06) 101827
- 12 Anton C, Carvalho FM, Oliveira EI, Maciel GA, Baracat EC, Carvalho JP. A comparison of CA125, HE4, risk ovarian malignancy algorithm (ROMA), and risk malignancy index (RMI) for the classification of ovarian masses. Clinics (Sao Paulo) 2012; 67 (05) 437-441
- 13 Park H, Shin JE, Lee DW, Kim MJ, Lee HN. Diagnostic accuracy of the risk of ovarian malignancy algorithm in clinical practice at a single hospital in Korea. Ann Lab Med 2019; 39 (03) 252-262
- 14 Lee YJ, Kim YM, Kang JS, Nam SH, Kim DY, Kim YT. Comparison of Risk of Ovarian Malignancy Algorithm and cancer antigen 125 to discriminate between benign ovarian tumor and early-stage ovarian cancer according to imaging tumor subtypes. Oncol Lett 2020; 20 (01) 931-938
- 15 Ngu SF, Chai YK, Choi KM. et al. Diagnostic Performance of Risk of Malignancy Algorithm (ROMA), Risk of Malignancy Index (RMI) and Expert Ultrasound Assessment in a Pelvic Mass Classified as Inconclusive by International Ovarian Tumour Analysis (IOTA) Simple Rules. Cancers (Basel) 2022; 14 (03) 810
- 16 Allison KH, Hammond MEH, Dowsett M. et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP guideline update. J Clin Oncol 2020; 38 (12) 1346-1366
- 17 Wang J, Wang B, Li C. et al. Evolving global trends in PCOS burden: a three-decade analysis (1990-2021) with projections to 2036 among adolescents and young adults. Front Endocrinol (Lausanne) 2025; 16: 1569694
- 18 Kim B, Park Y, Kim B. et al. Diagnostic performance of CA 125, HE4, and risk of Ovarian Malignancy Algorithm for ovarian cancer. J Clin Lab Anal 2019; 33 (01) e22624
- 19 Hsu ST, Su YJ, Hung CH, Chen MJ, Lu CH, Kuo CE. Automatic ovarian tumors recognition system based on ensemble convolutional neural network with ultrasound imaging. BMC Med Inform Decis Mak 2022; 22 (01) 298
- 20 Jacobs I, Bast Jr RC. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod 1989; 4 (01) 1-12