

Subscribe to RSS
DOI: 10.1055/s-0046-1816560
Probing Perianal Fistulas with Diffusion-Weighted Magnetic Resonance Imaging: Insights into Activity and Architecture
Authors


Abstract
Background and Objectives
Magnetic resonance imaging (MRI) is the imaging modality of choice for evaluation of perianal fistulas. With the emergence of newer treatment modalities, it is imperative to assess fistula “activity,” along with its architecture, for effective management. The objectives of this study were to estimate the cut-off for the mean apparent diffusion coefficient (ADC) value to differentiate between active and inactive fistulas and to assess the role of diffusion-weighted imaging (DWI) in the characterization of perianal fistulas.
Methods
MRI examination was performed on 54 patients using a 3T MRI system. Combined T2W + DWI and contrast-enhanced MRI (CE-MRI) images were evaluated for the visibility of fistulas. The ADC value was measured using region-of-interest placement within the fistula tract. Fistulas were designated as active or inactive based on surgical and/or clinical findings. Data were analyzed using standard statistical methods.
Results
Combined T2W + DWI and CE-MRI showed substantial agreement in visualization of fistulas, their internal openings, secondary tracts, and associated abscesses (p < 0.01). Inactive fistulas had significantly higher ADC values than active fistulas (p < 0.01). A cut-off of ADC value ≤1.170 × 10−3 mm2/s predicted active fistula with a sensitivity of 92.7%, a specificity of 85.7%, and a diagnostic accuracy of 82%.
Conclusion
Addition of DWI to T2-weighted imaging is a logistically feasible way of assessing fistula activity, along with optimal evaluation of the fistula architecture. DWI obviates the requirement of gadolinium-based contrast administration.
Introduction
Perianal fistula refers to an abnormal epithelium-lined track between the rectum or anal canal and the perianal skin. It is a prevalent condition in the South Asian population that significantly impairs quality of life due to chronic pain, discomfort, and the potential for recurrent infections.[1] [2]
Perianal fistulas are frequently difficult to treat, and even with intensive medical and surgical treatment, complete recovery is uncommon. A more aggressive approach is often required for fistulas actively draining pus or showing signs of active inflammation on clinical examination and/or surgical exploration, which are considered to be “active” fistulas. After surgical therapy, complications such as fecal incontinence and recurrence are reported in as many as 25 to 30% of cases, frequently caused by poorly understood architecture of the fistulous tract and its relationship to the anal sphincter complex, undetected secondary tracts, and/or infections associated with the fistula.[3] [4] [5] [6]
Magnetic resonance imaging (MRI) is regarded as the imaging modality of choice due to its outstanding soft tissue contrast and multiplanar capacity.[7] [8] [9] Contrast-enhanced sequences are frequently added to the MRI technique as they help identify active lesions and detect abscess development more accurately. Albeit it is costly, and although rare, gadolinium-based contrast agents—particularly Class I agents—carry a risk of developing nephrogenic systemic fibrosis (NSF) in patients with renal insufficiency.[10] Diffusion-weighted imaging (DWI), on the other hand, is a functional imaging approach based on water movement that effectively contrasts the inflammatory process from nearby normal-appearing tissues.
The objectives of this study were to estimate cut-off for the mean apparent diffusion coefficient (ADC) value to differentiate between active and inactive fistulas and to assess the role of DWI in characterization of perianal fistulas.
Materials and Methods
This cross-sectional study was conducted in the Department of Radiodiagnosis at a tertiary care hospital in New Delhi, India. Fifty-four patients referred to the Department of Radiodiagnosis with a clinical diagnosis of perianal fistula were included in the study after obtaining informed written consent. Patients with contraindications to MRI, such as cardiac pacemakers, MR unsafe metallic implants, cochlear and ocular implants, hemostatic clips, claustrophobic patients, and patients with contraindications for intravenous contrast administration were excluded from the study.
MRI was performed on a Siemens Germany 3T MRI system MAGNETOM Skyra and following MRI sequences were obtained: oblique axial and oblique coronal T2-weighted fast spin-echo imaging (TR/TE: 4,000–6,000/90–120 ms; slice thickness: 3 mm; interslice gap: 0.5 mm; field of view [FOV]: 22–26 cm; matrix: 256 × 256); DWI (single-shot EPI; b = 0, 400, 800 s/mm2; TR/TE: 4,000–6,000/60–90 ms; slice thickness: 3 mm; FOV: 22–26 cm; matrix: 128 × 128), with ADC maps generated; oblique axial and oblique coronal contrast-enhanced T1-weighted (T1W) imaging (TR/TE: 500–800/10–15 ms; slice thickness: 3 mm; gap: 0.5 mm; FOV: 22–26 cm; matrix: 256 × 256), following intravenous gadolinium-based contrast administration (0.1 mmol/kg).
Along with morphological assessment of the fistula tract, contrast-enhanced MRI (CE-MRI) and combined T2W + DWI sequences were assessed for the visibility of internal opening, secondary tracts, and associated abscesses on a three-point Likert scale as follows: score 0: not visualized, score 1: poorly visualized, and score 2: adequately visualized.
Evaluation of Fistula Architecture
-
Internal opening: proximal opening of the fistulous tract was defined as an interruption of the anal sphincter showing T2-weighted (T2W)/DWI hyperintensity or post-contrast enhancement.
-
Secondary tracts: contrast-enhancing, T2W/DWI hyperintense tracts radiating from the primary tract into the intersphincteric or ischioanal/ischiorectal space.
-
Abscess: focal dilatation of the fistulous tract more than 5 mm showing diffusion restriction and irregular peripheral post-contrast enhancement.[4]
-
Classification of the fistula: as per St. James's University Hospital Classification.
Quantitative Analysis for ADC Values
ADC values were calculated by placing a circular region of interest as large as possible within the confines of the fistulous tract. ADC values were measured three times in different regions and an average value was calculated.
Clinical and/or Surgical Correlation for Fistula “Activity”
The fistulas were divided into two groups: “active” and “inactive” based on clinical and/or surgical findings. For 46 individuals who underwent surgery, operative findings were used as the reference. Identification of pus within the fistula tract or an associated abscess on surgery resulted in its classification as an active fistula. Eight individuals who did not undergo surgery were divided into the two groups based on the findings of local clinical assessment. A perianal fistula was considered active if it was associated with purulent discharge or visible signs of active inflammation, such as redness, pain, swelling, and fluctuation. The ones lacking such features on surgical/clinical findings were considered inactive.
Statistical Analysis
Data were entered and coded in MS Excel spreadsheet program. SPSS v23 (IBM Corp.) was used for data analysis. For continuous variables, descriptive statistics were presented as means/standard deviations (SDs) and medians/interquartile ranges; for categorical variables, they were expressed as frequencies and percentages. For categorical data group comparisons, the chi-squared test was employed. The Kappa test was used to estimate the agreement between two different tests in measuring the outcome. The statistical significance was maintained at p <0.05. To determine the optimal cut-off for a continuous predictor forecasting a binary result, receiver operating characteristic (ROC) curve analysis was carried out.
Results
Out of 54 participants in our study, 46 were male and 8 were female. Almost 80% of the participants were in the second to fourth decade of life. The mean (SD) age was 37.2 (11.9) years. Perianal discharge and perianal pain were the most common clinical symptoms in our study. Frank pus discharge and perianal erythema/tenderness were the common signs elicited on clinical examination. One of the participants had tuberculosis, 2 had Crohn's disease/ulcerative colitis, and 1 had a history of anorectal trauma. The remaining 50 (92.5%) participants had no known contributory cause.
Sixty-two fistulas were detected in 54 patients. In our study, 8 (14.8%) participants had more than one fistula. Based on clinical and surgical findings, 41 (66.2%) of the fistulas were classified as “active” and 21 (33.8%) of the fistulas were classified as “inactive.”
Characterization of the Fistulas on MRI
As per St. James University Hospital Classification, the most common type of perianal fistula in our study was class 1 fistula (35.5%). The least common type was class 5 fistula (1.6%) ([Table 1]). Nineteen (30%) of the fistulas had secondary ramifications in the intersphincteric or ischiorectal/ischioanal space. Thirty (48.3%) of the fistulas were associated with an abscess.
Comparison of Visibility Scores Between Combined T2W + DWI and CE-MRI
The two methods agreed on the visibility score of the fistulas in 96.7% cases with a substantial level of agreement (k = 0.652), which was statistically significant (p < 0.01). On assessment of internal opening, the two approaches agreed in 83.8% of the fistulas with a substantial level of agreement (k = 0.626, p < 0.01). Almost perfect agreement was seen in the visibility scores of abscesses, where the two methods agreed in 90% of the fistulas (k = 0.911, p < 0.01). The two methods agreed on the visibility score of the secondary tracts in 68.4% of the fistulas with a substantial level of agreement (k = 0.795, p < 0.01; [Table 2] and [Figs. 1] [2] [3] [4]).
Abbreviations: CE-MRI, contrast-enhanced magnetic resonance imaging; DWI, diffusion-weighted imaging; MRI, magnetic resonance imaging; T2W, T2-weighted.




Our study also found a significant linear trend with an increase in the mean visibility score of the fistulas on T2W, combined T2W + DWI, and CE-MRI (p < 0.001). CE-MRI had the highest mean visibility score (1.97). Isolated T2W had the lowest mean visibility score (1.54). However, addition of DWI to T2W improved fistula detection from score 1 to score 2 in 34 cases. The mean visibility score on combined T2W + DWI was 1.93.
Association Between Activity and ADC Value
The mean (SD) of ADC value (in × 10−3 mm2/s) in active and inactive fistulas was 0.99 (0.15) and 1.23 (0.15), respectively. This difference in ADC values was statistically significant (p < 0.01), with inactive fistulas having higher ADC values ([Fig. 5]).

Prediction Analysis for Activity Using ADC Values
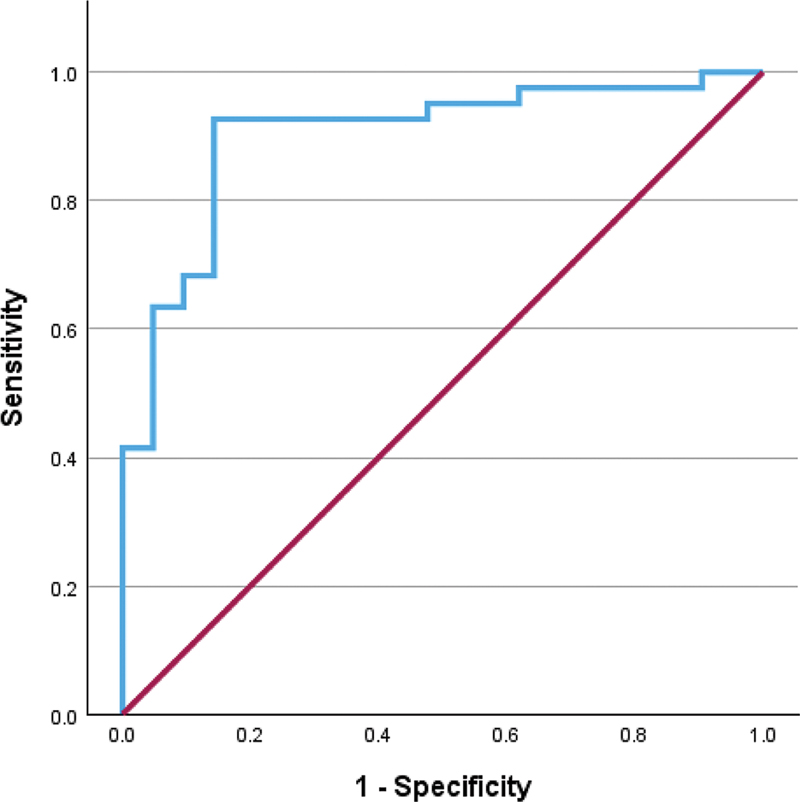
On ROC analysis, the area under the ROC curve was 0.901 and the optimal cut-off ADC was 1.17 × 10−3 mm2/s with lower values predicting an active fistula. This optimal cut-off ADC yielded a sensitivity of 92.7% and a specificity of 85.7%, giving a diagnostic accuracy of 82% ([Fig. 6]).
Discussion
A perianal fistula is an abnormal tract that connects the rectum or the anal canal to the perianal skin. About 8.6 out of every 10,000 people in South Asian countries suffer from this extremely common ailment, predominantly affecting males in the third and fifth decades of life.[1] [2]
Surgical management involves tract excision with abscess drainage while preserving the anal sphincter; however, recurrence and fecal incontinence occur in up to 25 to 30% of cases. These are often associated with complex fistulae, horseshoe extensions, unidentified internal openings, missed extensions, and prior surgery.[4] [11]
Hence, preoperative understanding of the fistula architecture and the extent of disease is essential for effective patient management.
In recent times, procedures like LIFT (ligation of intersphincteric tract), mucosal flap advancement, and biomaterials like biological glues and collagen-based materials are promising alternatives as well as adjuncts, particularly in complex fistulas.[12] [13] With the emergence of these newer treatment modalities, it has also become important to assess the “activity” of the ongoing infectious process, as active fistulas often require a more aggressive management approach. Assessment of the activity of the fistulous tract is also required in monitoring treatment response in patients with Crohn's disease–associated perianal fistulas.[14]
MRI is the most accurate noninvasive method for determining the presence and architecture of the entire fistulous tract in relation to the underlying anatomy in a projection relevant to surgical exploration.[7] [8] [9] Preoperative MRI avoids treatment failure after surgery and reduces further recurrence by 75%, especially in patients with recurrent fistulas.[15] [16] [17] [18] [19] [20]
On MRI, perianal fistulas are frequently diagnosed on conventional T1W and fat-suppressed T2W turbo spin echo or fast spin echo sequences. However, these sequences are unable to differentiate between active and inactive diseases. Fistulas containing pus and areas of edema show high signal intensity on T2WI, which may be seen even in the fibrosed tracts.[21] Post-gadolinium T1W images are often added to the MRI technique as they help identify active lesions and detect abscess development more accurately.[22] [23] However, contrast use increases cost, and, although rare, gadolinium-based contrast agents—particularly Class I agents—in patients with renal insufficiency carry a risk of NSF.[21] [24] [25]
DWI is a functional imaging technique that provides information about water mobility, tissue cellularity, and the integrity of the cell membranes. In body imaging, DWI has mostly been utilized for tumor detection and characterization. However, in recent times, DWI has been found to be useful in the identification of perianal fistulas and their complications.[26] The DWI signal increases with a reduction in water molecule mobility, and the ADC value drops along with it. Hence, DWI not only provides information regarding fistula anatomy, but also provides functional information regarding the disease activity. Further added advantage of DWI is that it can be easily incorporated into the MRI protocol as it does not require any additional equipment or contrast, the acquisition time is less, and data processing is relatively easier.[26] [27] [28]
The current study was performed to estimate cut-off for mean ADC values to differentiate between active and inactive fistulas and to assess the role of DWI in the characterization of perianal fistulas.
Our study comprised 54 patients with a mean age of 37.2 years. This correlates with multiple studies that suggest that perianal fistula is commonly seen in the second to fourth decades of life. The mean age of participants in studies done by Boruah et al[4] and Mohsen and Osman[22] were 38.5 years and 37 years, respectively. In our study, 85.1% of the participants were male and 14.9% were female. This is similar to previous studies showing a male predilection for the disease.[4] [26] [29] No known contributory causes were present in 92.5% of our study participants. Sainio[1] has also suggested that most of the perianal fistulas are idiopathic in origin.
Characterization of the Fistulas on MRI
Sixty-two fistulas were detected in 54 patients. In our study, 8 (14.8%) patients had more than one fistula. Boruah et al[4] and Mohsen and Osman[22] also reported that 8 (17%) and 7 (18%) of their study population had more than one fistula, respectively.
As per St. James University Hospital Classification, the most common type of perianal fistula in our study was class 1 fistula (35.5%). The least common type was class 5 fistula (1.6%). Among the remaining fistulas, 27.4% were classified as class 2, 8.0% as class 3, and 27.4% were classified as class 4. Mohsen and Osman[22] and Aggarwal et al[30] also found that the most common type of fistula in their study population was grade 1. This can be explained by the most widely accepted theory of cryptoglandular origin of perianal fistula, whereby intersphincteric gland infection with an obstructed duct represents the inciting event. The sphincter complex functions as a barrier and, as the abscess ruptures, pus moves into the intersphincteric space—the path of least resistance—where it eventually forms an intersphincteric fistula.[31] However, Aslan reported that grade 3 and grade 4 fistulas were more common in their study population.[32]
Nineteen (30%) of the fistulas in our study had secondary ramifications in the intersphincteric or ischiorectal/ischioanal space. Boruah et al[4] and Aslan[32] also found secondary tracts in almost 50 to 60% of the fistulas. Thirty (48.3%) of the fistulas in our study were associated with an abscess. Boruah et al[4] and Aslan[32] found abscesses in 40 and 56% of their study population, respectively.
Comparison of Visibility Scores
One of the major limitations of DWI is the inherent poor spatial resolution in comparison to spin-echo or gradient-echo sequences, making it difficult to assess the fistula architecture in relation to the anal canal and perianal anatomy, especially the sphincter complex. Therefore, agreement between visibility scores was compared between combined T2W + DWI (rather than isolated DWI) and CE-MRI sequences.[33] [34] DWI sequences with higher b-value (b = 800 s/mm2) were used as they show improved contrast, higher tissue diffusibility, and lesser T2 shine-through effect as compared to lower b-value images.[35]
Our study showed that combined T2W + DWI and CE-MRI showed similar performance in characterizing the fistula architecture. The two methods showed substantial agreement in visualizing the fistula tracts (k = 0.652, p < 0.01), their internal openings (k = 0.626, p < 0.01), and secondary ramifications (k = 0.795, p < 0.01). The two methods showed almost perfect agreement in visualizing associated abscesses (k = 0.911, p < 0.01).
Disagreement in visibility of 3.3% fistulas between combined T2 + DWI and CE-MRI may be attributed to differences in contrast mechanisms, fistula activity, spatial resolution, and susceptibility artifacts. Chronic or fibrotic tracts may be visible on T2W images but show limited enhancement or diffusion restriction, while small tracts may be underestimated on DWI than CE-MRI due to lower spatial resolution.
Aggarwal et al[30] also found that combining DWI with T2WI was as effective as CE-MRI in detecting and characterizing perianal fistulas with almost perfect agreement for the detection of the internal opening, secondary tracts, and abscesses. Cavusoglu et al[26] also found no significant difference in the ability to detect fistulas and abscesses, on adding DWI or CE-MRI to the T2WI sequence; however, they suggested that adding CE-MRI was more effective in identifying internal openings and secondary tracts than adding DWI to T2WI.
Association Between Activity and ADC Value
The mean (SD) of ADC value (in × 10−3 mm2/s) in active and inactive fistulas was 0.99 (0.15) and 1.23 (0.15), respectively. This difference in ADC value was statistically significant (p < 0.01), with inactive fistulas having higher ADC values. Our findings were similar to the studies by Boruah et al,[4] Yoshizako et al,[29] and Wang et al,[36] who also found that the ADC values of the active fistulas were significantly lower than those of the inactive fistulas, in their respective studies. However, Mohsen and Osman[22] found that there was no significant difference in ADC values between active and inactive fistulas in their study.
Prediction Analysis for Activity Using ADC Values
On ROC analysis, the optimal cut-off ADC value to differentiate between active and inactive fistulas was 1.170 × 10−3 mm2/s, with a lower ADC value suggestive of an active fistula. It yielded a sensitivity of 92.7%, a specificity of 85.7%, and a diagnostic accuracy of 82%. Similarly, Yoshizako et al[29] suggested a cut-off ADC value of 1.109 × 10−3 mm2/s to differentiate between active and inactive fistulas. In another study, Boruah et al[4] reported that a cut-off ADC value of 1.105 × 10−3 mm2/s could differentiate active from inactive fistula with a diagnostic accuracy of 82.98%.
Conclusion
We conclude from this study that the addition of DWI to T2WI offers a noninvasive, logistically feasible, contrast-free alternative in detecting and characterizing fistula architecture and associated complications. It also provides insight into the active inflammatory disease process, which has an established role in presurgical evaluation as well as selection for novel nonsurgical treatment options. These benefits are especially pertinent for patients with renal impairment or contraindications to contrast administration.
Merits and Limitations of Our Study
Even though few studies are available from the Indian population to assess the role of DWI in the evaluation of perianal fistulae, these studies have been performed on 0.5/1.5T MRI machines. Our study was performed on a 3T MRI machine that provides more detailed images. Also, for assigning the visibility scores, our study used a three-point scale including a “poorly visualized” category, along with “not visualized” and “adequately visualized.” This is a more realistic categorization, as many a times, visibility of a pathological process on MRI does not fit into a binary classification of “visualized” and “not visualized.”
Limitations of our study include a small sample size, a single-center design, and limited generalizability to other field strengths. A multicenter study with a large sample size is required to establish a cut-off ADC value to differentiate between active and inactive fistulas.
Conflict of Interest
None declared.
Acknowledgements
None.
-
References
- 1 Sainio P. Fistula-in-ano in a defined population. Incidence and epidemiological aspects. Ann Chir Gynaecol 1984; 73 (04) 219-224
- 2 Zanotti C, Martinez-Puente C, Pascual I, Pascual M, Herreros D, García-Olmo D. An assessment of the incidence of fistula-in-ano in four countries of the European Union. Int J Colorectal Dis 2007; 22 (12) 1459-1462
- 3 Sharma A, Yadav P, Sahu M. et al. Current imaging techniques for evaluation of fistula in ano: a review. Egypt J Radiol Nucl Med 2020; 51: 130
- 4 Boruah DK, Hazarika K, Ahmed H. et al. Role of diffusion-weighted imaging in the evaluation of perianal fistulae. Indian J Radiol Imaging 2021; 31 (01) 91-101
- 5 Tozer PJ, Burling D, Gupta A, Phillips RK, Hart AL. Review article: medical, surgical and radiological management of perianal Crohn's fistulas. Aliment Pharmacol Ther 2011; 33 (01) 5-22
- 6 Amato A, Bottini C, De Nardi P. et al; Italian society of colorectal surgery. Evaluation and management of perianal abscess and anal fistula: a consensus statement developed by the Italian Society of Colorectal Surgery (SICCR). Tech Coloproctol 2015; 19 (10) 595-606
- 7 Sahni VA, Ahmad R, Burling D. Which method is best for imaging of perianal fistula?. Abdom Imaging 2008; 33 (01) 26-30
- 8 Berman L, Israel GM, McCarthy SM, Weinreb JC, Longo WE. Utility of magnetic resonance imaging in anorectal disease. World J Gastroenterol 2007; 13 (23) 3153-3158
- 9 Beets-Tan RGH, Beets GL, van der Hoop AG. et al. Preoperative MR imaging of anal fistulas: does it really help the surgeon?. Radiology 2001; 218 (01) 75-84
- 10 Baskan O, Koplay M, Sivri M, Erol C. Our experience with MR imaging of perianal fistulas. Pol J Radiol 2014; 79: 490-497
- 11 Garcia-Aguilar J, Belmonte C, Wong WD, Goldberg SM, Madoff RD. Anal fistula surgery. Factors associated with recurrence and incontinence. Dis Colon Rectum 1996; 39 (07) 723-729
- 12 Sileri P, Cadeddu F, D'Ugo S. et al. Surgery for fistula-in-ano in a specialist colorectal unit: a critical appraisal. BMC Gastroenterol 2011; 11 (01) 120
- 13 Gage KL, Deshmukh S, Macura KJ, Kamel IR, Zaheer A. MRI of perianal fistulas: bridging the radiological-surgical divide. Abdom Imaging 2013; 38 (05) 1033-1042
- 14 Ziech MLW, Lavini C, Bipat S. et al. Dynamic contrast-enhanced MRI in determining disease activity in perianal fistulizing Crohn disease: a pilot study. AJR Am J Roentgenol 2013; 200 (02) W170-7
- 15 Halligan S, Stoker J. Imaging of fistula in ano. Radiology 2006; 239 (01) 18-33
- 16 Szurowska E, Wypych J, Izycka-Swieszewska E. Perianal fistulas in Crohn's disease: MRI diagnosis and surgical planning: MRI in fistulazing perianal Crohn's disease. Abdom Imaging 2007; 32 (06) 705-718
- 17 Waniczek D, Adamczyk T, Arendt J, Kluczewska E, Kozińska-Marek E. Usefulness assessment of preoperative MRI fistulography in patients with perianal fistulas. Pol J Radiol 2011; 76 (04) 40-44
- 18 Buchanan G, Halligan S, Williams A. et al. Effect of MRI on clinical outcome of recurrent fistula-in-ano. Lancet 2002; 360 (9346): 1661-1662
- 19 Singh K, Singh N, Thukral C, Singh KP, Bhalla V. Magnetic resonance imaging (MRI) evaluation of perianal fistulae with surgical correlation. J Clin Diagn Res 2014; 8 (06) RC01-RC04
- 20 Morris J, Spencer JA, Ambrose NS. MR imaging classification of perianal fistulas and its implications for patient management. Radiographics 2000; 20 (03) 623-635 , discussion 635–637
- 21 Torkzad MR, Ahlström H, Karlbom U. Comparison of different magnetic resonance imaging sequences for assessment of fistula-in-ano. World J Radiol 2014; 6 (05) 203-209
- 22 Mohsen LA, Osman NM. Diffusion-weighted imaging in the evaluation of perianal fistula and abscess. Egypt J Radiol Nucl Med 2020; 51 (01) 71
- 23 Yildirim N, Gökalp G, Öztürk E. et al. Ideal combination of MRI sequences for perianal fistula classification and the evaluation of additional findings for readers with varying levels of experience. Diagn Interv Radiol 2012; 18 (01) 11-19
- 24 Shellock FG, Spinazzi A. MRI safety update 2008: part 1, MRI contrast agents and nephrogenic systemic fibrosis. AJR Am J Roentgenol 2008; 191 (04) 1129-1139
- 25 Chrysochou C, Buckley DL, Dark P, Cowie A, Kalra PA. Gadolinium-enhanced magnetic resonance imaging for renovascular disease and nephrogenic systemic fibrosis: critical review of the literature and UK experience. J Magn Reson Imaging 2009; 29 (04) 887-894
- 26 Cavusoglu M, Duran S, Sözmen Cılız D. et al. Added value of diffusion-weighted magnetic resonance imaging for the diagnosis of perianal fistula. Diagn Interv Imaging 2017; 98 (05) 401-408
- 27 Horsthuis K, Lavini C, Bipat S, Stokkers PC, Stoker J. Perianal Crohn disease: evaluation of dynamic contrast-enhanced MR imaging as an indicator of disease activity. Radiology 2009; 251 (02) 380-387
- 28 Spencer JA, Ward J, Beckingham IJ, Adams C, Ambrose NS. Dynamic contrast-enhanced MR imaging of perianal fistulas. AJR Am J Roentgenol 1996; 167 (03) 735-741
- 29 Yoshizako T, Wada A, Takahara T. et al. Diffusion-weighted MRI for evaluating perianal fistula activity: feasibility study. Eur J Radiol 2012; 81 (09) 2049-2053
- 30 Aggarwal P, Malik R, Sarawagi R, Kumar A. Comparing the efficacy of a combination of diffusion-weighted imaging and T2-STIR (short tau inversion recovery) imaging with contrast-enhanced MRI in the evaluation of perianal fistula. Cureus 2024; 16 (02) e53485
- 31 de Miguel Criado J, del Salto LG, Rivas PF. et al. MR imaging evaluation of perianal fistulas: spectrum of imaging features. Radiographics 2012; 32 (01) 175-194
- 32 Aslan S. Added value of contrast-enhanced and diffusion-weighted MRI data sets for characterization of perianal fistulas; single center experience. Ann Med Res 2020; 27 (10) 2763
- 33 Yoshizako T, Kitagaki H. A pictorial review of the impact of adding diffusion-weighted MR imaging to other MR sequences for assessment of anal fistulae. Jpn J Radiol 2013; 31 (06) 371-376
- 34 Hori M, Oto A, Orrin S, Suzuki K, Baron RL. Diffusion-weighted MRI: a new tool for the diagnosis of fistula in ano. J Magn Reson Imaging 2009; 30 (05) 1021-1026
- 35 Tomar V, Yadav A, Rathore RKS. et al. Apparent diffusion coefficient with higher b-value correlates better with viable cell count quantified from the cavity of brain abscess. AJNR Am J Neuroradiol 2011; 32 (11) 2120-2125
- 36 Wang Y, Gu C, Huo Y. et al. Diffusion tensor imaging for evaluating perianal fistula: Feasibility study. Medicine (Baltimore) 2018; 97 (29) e11570
Address for correspondence
Publication History
Article published online:
06 February 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Sainio P. Fistula-in-ano in a defined population. Incidence and epidemiological aspects. Ann Chir Gynaecol 1984; 73 (04) 219-224
- 2 Zanotti C, Martinez-Puente C, Pascual I, Pascual M, Herreros D, García-Olmo D. An assessment of the incidence of fistula-in-ano in four countries of the European Union. Int J Colorectal Dis 2007; 22 (12) 1459-1462
- 3 Sharma A, Yadav P, Sahu M. et al. Current imaging techniques for evaluation of fistula in ano: a review. Egypt J Radiol Nucl Med 2020; 51: 130
- 4 Boruah DK, Hazarika K, Ahmed H. et al. Role of diffusion-weighted imaging in the evaluation of perianal fistulae. Indian J Radiol Imaging 2021; 31 (01) 91-101
- 5 Tozer PJ, Burling D, Gupta A, Phillips RK, Hart AL. Review article: medical, surgical and radiological management of perianal Crohn's fistulas. Aliment Pharmacol Ther 2011; 33 (01) 5-22
- 6 Amato A, Bottini C, De Nardi P. et al; Italian society of colorectal surgery. Evaluation and management of perianal abscess and anal fistula: a consensus statement developed by the Italian Society of Colorectal Surgery (SICCR). Tech Coloproctol 2015; 19 (10) 595-606
- 7 Sahni VA, Ahmad R, Burling D. Which method is best for imaging of perianal fistula?. Abdom Imaging 2008; 33 (01) 26-30
- 8 Berman L, Israel GM, McCarthy SM, Weinreb JC, Longo WE. Utility of magnetic resonance imaging in anorectal disease. World J Gastroenterol 2007; 13 (23) 3153-3158
- 9 Beets-Tan RGH, Beets GL, van der Hoop AG. et al. Preoperative MR imaging of anal fistulas: does it really help the surgeon?. Radiology 2001; 218 (01) 75-84
- 10 Baskan O, Koplay M, Sivri M, Erol C. Our experience with MR imaging of perianal fistulas. Pol J Radiol 2014; 79: 490-497
- 11 Garcia-Aguilar J, Belmonte C, Wong WD, Goldberg SM, Madoff RD. Anal fistula surgery. Factors associated with recurrence and incontinence. Dis Colon Rectum 1996; 39 (07) 723-729
- 12 Sileri P, Cadeddu F, D'Ugo S. et al. Surgery for fistula-in-ano in a specialist colorectal unit: a critical appraisal. BMC Gastroenterol 2011; 11 (01) 120
- 13 Gage KL, Deshmukh S, Macura KJ, Kamel IR, Zaheer A. MRI of perianal fistulas: bridging the radiological-surgical divide. Abdom Imaging 2013; 38 (05) 1033-1042
- 14 Ziech MLW, Lavini C, Bipat S. et al. Dynamic contrast-enhanced MRI in determining disease activity in perianal fistulizing Crohn disease: a pilot study. AJR Am J Roentgenol 2013; 200 (02) W170-7
- 15 Halligan S, Stoker J. Imaging of fistula in ano. Radiology 2006; 239 (01) 18-33
- 16 Szurowska E, Wypych J, Izycka-Swieszewska E. Perianal fistulas in Crohn's disease: MRI diagnosis and surgical planning: MRI in fistulazing perianal Crohn's disease. Abdom Imaging 2007; 32 (06) 705-718
- 17 Waniczek D, Adamczyk T, Arendt J, Kluczewska E, Kozińska-Marek E. Usefulness assessment of preoperative MRI fistulography in patients with perianal fistulas. Pol J Radiol 2011; 76 (04) 40-44
- 18 Buchanan G, Halligan S, Williams A. et al. Effect of MRI on clinical outcome of recurrent fistula-in-ano. Lancet 2002; 360 (9346): 1661-1662
- 19 Singh K, Singh N, Thukral C, Singh KP, Bhalla V. Magnetic resonance imaging (MRI) evaluation of perianal fistulae with surgical correlation. J Clin Diagn Res 2014; 8 (06) RC01-RC04
- 20 Morris J, Spencer JA, Ambrose NS. MR imaging classification of perianal fistulas and its implications for patient management. Radiographics 2000; 20 (03) 623-635 , discussion 635–637
- 21 Torkzad MR, Ahlström H, Karlbom U. Comparison of different magnetic resonance imaging sequences for assessment of fistula-in-ano. World J Radiol 2014; 6 (05) 203-209
- 22 Mohsen LA, Osman NM. Diffusion-weighted imaging in the evaluation of perianal fistula and abscess. Egypt J Radiol Nucl Med 2020; 51 (01) 71
- 23 Yildirim N, Gökalp G, Öztürk E. et al. Ideal combination of MRI sequences for perianal fistula classification and the evaluation of additional findings for readers with varying levels of experience. Diagn Interv Radiol 2012; 18 (01) 11-19
- 24 Shellock FG, Spinazzi A. MRI safety update 2008: part 1, MRI contrast agents and nephrogenic systemic fibrosis. AJR Am J Roentgenol 2008; 191 (04) 1129-1139
- 25 Chrysochou C, Buckley DL, Dark P, Cowie A, Kalra PA. Gadolinium-enhanced magnetic resonance imaging for renovascular disease and nephrogenic systemic fibrosis: critical review of the literature and UK experience. J Magn Reson Imaging 2009; 29 (04) 887-894
- 26 Cavusoglu M, Duran S, Sözmen Cılız D. et al. Added value of diffusion-weighted magnetic resonance imaging for the diagnosis of perianal fistula. Diagn Interv Imaging 2017; 98 (05) 401-408
- 27 Horsthuis K, Lavini C, Bipat S, Stokkers PC, Stoker J. Perianal Crohn disease: evaluation of dynamic contrast-enhanced MR imaging as an indicator of disease activity. Radiology 2009; 251 (02) 380-387
- 28 Spencer JA, Ward J, Beckingham IJ, Adams C, Ambrose NS. Dynamic contrast-enhanced MR imaging of perianal fistulas. AJR Am J Roentgenol 1996; 167 (03) 735-741
- 29 Yoshizako T, Wada A, Takahara T. et al. Diffusion-weighted MRI for evaluating perianal fistula activity: feasibility study. Eur J Radiol 2012; 81 (09) 2049-2053
- 30 Aggarwal P, Malik R, Sarawagi R, Kumar A. Comparing the efficacy of a combination of diffusion-weighted imaging and T2-STIR (short tau inversion recovery) imaging with contrast-enhanced MRI in the evaluation of perianal fistula. Cureus 2024; 16 (02) e53485
- 31 de Miguel Criado J, del Salto LG, Rivas PF. et al. MR imaging evaluation of perianal fistulas: spectrum of imaging features. Radiographics 2012; 32 (01) 175-194
- 32 Aslan S. Added value of contrast-enhanced and diffusion-weighted MRI data sets for characterization of perianal fistulas; single center experience. Ann Med Res 2020; 27 (10) 2763
- 33 Yoshizako T, Kitagaki H. A pictorial review of the impact of adding diffusion-weighted MR imaging to other MR sequences for assessment of anal fistulae. Jpn J Radiol 2013; 31 (06) 371-376
- 34 Hori M, Oto A, Orrin S, Suzuki K, Baron RL. Diffusion-weighted MRI: a new tool for the diagnosis of fistula in ano. J Magn Reson Imaging 2009; 30 (05) 1021-1026
- 35 Tomar V, Yadav A, Rathore RKS. et al. Apparent diffusion coefficient with higher b-value correlates better with viable cell count quantified from the cavity of brain abscess. AJNR Am J Neuroradiol 2011; 32 (11) 2120-2125
- 36 Wang Y, Gu C, Huo Y. et al. Diffusion tensor imaging for evaluating perianal fistula: Feasibility study. Medicine (Baltimore) 2018; 97 (29) e11570