

Subscribe to RSS
DOI: 10.1055/s-0045-1814759
Microsurgical Clipping of Ruptured Cerebral Aneurysms in a Regional Hospital: A 7-Year Single-Surgeon Experience
Authors

Abstract
Background
Microsurgical clipping remains a vital treatment for ruptured cerebral aneurysms, particularly in regional hospitals where emergent endovascular access may be limited. Timely surgery by experienced neurosurgeons can yield favorable outcomes even outside academic centers.
Aims
The aim of the study is to evaluate clinical outcomes of microsurgical clipping for ruptured cerebral aneurysms performed by a single neurosurgeon in a regional hospital over a seven-year period, with subgroup analysis by WFNS grade.
Materials and Methods
A retrospective cohort study was conducted on 189 patients with radiologically confirmed ruptured cerebral aneurysms who underwent microsurgical clipping at our center between July 2018 and June 2025. Data on demographics, aneurysm characteristics, clinical grade, surgical timing, and outcomes were analyzed. Subgroup analyses included WFNS grade (good-grade I–III vs. poor-grade IV–V), timing of surgery, and operative phase. Favorable outcome was defined as a modified Rankin Scale (mRS) score of 0 to 2 at 6 months.
Results
Good-grade WFNS patients comprised 59.3% of the cohort and achieved excellent outcomes, with 85.1% attaining mRS 0 to 2 at 6 months. Ultra-early surgery (<24 hours) was performed in 58.2% of cases. Overall mortality was 6.3%. At 6 months, 74.6% of all patients had favorable outcomes. Poor initial WFNS grade (OR 0.33, p = 0.011) and vasospasm (OR 0.15, p < 0.001) were independently associated with unfavorable outcomes.
Conclusion
Microsurgical clipping remains a safe and durable option for ruptured cerebral aneurysms in regional practice. With consistent surgical experience and timely intervention, outcomes comparable to those of academic centers can be achieved.
Keywords
ruptured cerebral aneurysm - microsurgical clipping - WFNS grade - surgical timing - functional outcome - cisternal irrigationIntroduction
Ruptured cerebral aneurysms represent a critical neurosurgical emergency, requiring timely intervention to prevent rebleeding, permanent neurological deficits, or death.[1] While both microsurgical clipping and endovascular coiling are accepted standard treatments, the choice of modality often depends on aneurysm morphology, clinical status, institutional resources, and urgency.[2] Although endovascular techniques have gained widespread popularity, their availability for emergency cases remains limited in many regional hospitals.[3] In particular, the use of endovascular intervention is often restricted to selected unruptured or complex aneurysms that can tolerate treatment delays.[4] Consequently, microsurgical clipping continues to play a central role in the management of ruptured aneurysms, especially in non-metropolitan areas where rapid surgical access remains more feasible.[5]
Our center is a large provincial hospital located in a small, remote city in northern Thailand. Although it is not a university-based tertiary referral center, it serves as the only neurosurgical referral hospital for a catchment population of approximately 1.4 million people across several provinces. Within this region, there are only eight practicing neurosurgeons in total, and microsurgical clipping of aneurysms is performed exclusively at this institution. In this context, microsurgical clipping represents the primary modality for ruptured aneurysms requiring urgent intervention. This study therefore reports the outcomes of a consecutive series of patients treated over a 7-year period by a single neurosurgeon within this regional referral system. While limited by its single-surgeon design, the series provides insights into the safety and feasibility of microsurgical clipping in real-world, resource-limited environments and may serve as a benchmark for similar regional hospitals in Asia and other developing regions.
Materials and Methods
This study was conducted at a large provincial referral center in northern Thailand. Although not a university-based tertiary hospital, it serves as the only institution in the region capable of performing microsurgical clipping for aneurysms. The center provides neurosurgical care for a catchment population of approximately 1.4 million people across several provinces, with only eight practicing neurosurgeons in the region. Within this system, all urgent cases of ruptured aneurysm requiring clipping were concentrated at this hospital and managed by the senior author, ensuring consistency of surgical technique and perioperative care throughout the study period
This retrospective cohort study included patients with ruptured cerebral aneurysms who underwent microsurgical clipping at a regional hospital between July 2018 and June 2025. All procedures were performed by a single neurosurgeon. Ethical approval was obtained from the local institutional review board (approval number blinded for peer review).
Inclusion criteria were patients aged 18 years or older with radiologically confirmed ruptured cerebral aneurysms who received microsurgical clipping as the primary treatment. There were no exclusion criteria.
Endovascular therapy became available at our center in 2020. During the study period, treatment modality was determined based on aneurysm location, clinical condition, and resource availability. Microsurgical clipping was generally performed for anterior circulation aneurysms and for most ruptured aneurysms requiring urgent intervention. Endovascular treatment was preferentially selected for posterior circulation aneurysms, as well as for patients with severe brain swelling in whom immediate craniotomy was deemed high risk. In such cases, endovascular intervention was typically scheduled as a non-emergency session once the patient's condition stabilized.
Clinical data were retrospectively collected from inpatient medical records, operative notes, and imaging archives. The following variables were extracted: demographic characteristics, comorbidities, aneurysm location and size, initial World Federation of Neurosurgical Societies (WFNS) grade, modified Fisher grade, surgical details, intraoperative events, postoperative complications, length of hospital stay, and total cost of treatment.
Clinical vasospasm was defined as the development of a new focal neurological deficit or unexplained decline in consciousness lasting >1 hour, not attributable to rebleeding, hydrocephalus, or metabolic disturbance. Radiological confirmation with computed tomography angiography (CTA) or digital subtraction angiography (DSA) was obtained when feasible.
Functional outcomes were assessed using the modified Rankin Scale (mRS) at discharge, and at 1 and 6 months. Outcome analyses, including subgroup comparisons, were conducted according to the intention-to-treat (ITT) principle with non-responder imputation: all enrolled patients were retained in the denominator, and those without 6-month follow-up data were conservatively classified as having unfavorable outcomes. Patients were followed either through scheduled outpatient clinic visits or, for those residing in remote areas, via telemedicine consultations conducted by the neurosurgical team.
For subgroup analysis, patients were categorized based on initial clinical grade, operative period, and long-term functional outcome:
-
Initial neurological status was stratified into good grade (WFNS I–III) and poor grade (WFNS IV–V) groups.
-
The operative period was divided into two phases:
-
(1) Initial phase (July 2018–December 2021), and
-
(2) Substantial phase (January 2022–June 2025), reflecting the evolution of surgical protocol and team proficiency.
-
-
Functional outcome was dichotomized as favorable (mRS 0–2 at 6 months) and unfavorable (mRS 3–6).
Descriptive and inferential statistics were performed using SPSS software (version 26.0; IBM Corp., Armonk, New York, United States). Continuous variables were presented as mean ± standard deviation or median with interquartile range, as appropriate. Categorical variables were summarized using frequencies and percentages. Group comparisons were analyzed using Chi-square or Fisher's exact test for categorical variables, and Student's t-test or Mann–Whitney U test for continuous variables. Statistical significance was defined as p < 0.05. Additionally, a post-hoc power analysis, using the observed 6-month favorable outcome rate of 74.6% compared with the 66% benchmark reported in the ISAT surgical arm, indicated approximately 68% power at a two-sided α of 0.05.
Operative Considerations and Management
All procedures were performed using an operating microscope (Zeiss Tivato, Carl Zeiss Meditec AG, Jena, Germany) equipped with intraoperative indocyanine green (ICG) angiography. Standard microsurgical instruments included the Takayama set and suction–irrigation system (Takayama Instrument Inc., Tokyo, Japan), intraoperative micro-Doppler ultrasonography (Mizuho Co., Ltd., Tokyo, Japan), and neuronavigation (Stealth Station, Medtronic, Minneapolis, Minnesota, United States), which was selectively employed in anatomically complex cases. Titanium aneurysm clips with Yasargil design were used in all cases. Clips were primarily sourced from Aesculap AG (Tuttlingen, Germany), supplemented by Peter Lazic GmbH (Tuttlingen, Germany) for specific shapes not available from a single vendor.
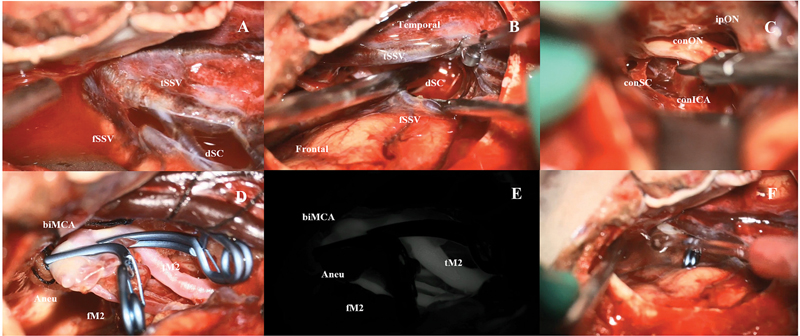
Most procedures utilized a standard pterional approach to ensure consistent exposure. For posterior circulation aneurysms—including those involving the PICA, SCA, or basilar trunk—alternative routes such as the subtemporal or retrosigmoid approach were chosen to optimize access. In all feasible cases, aggressive cisternal irrigation under microscopic visualization was routinely performed to clear subarachnoid blood, facilitate brain relaxation, and improve CSF dynamics ([Fig. 1]). “Postoperative CT findings demonstrating effective clearance of subarachnoid blood are illustrated in [Fig. 2].”

Brain relaxation was primarily achieved through CSF release via sharp arachnoid dissection; mannitol was used selectively. Temporary clipping of parent vessels was employed when necessary, typically limited to ≤10 minutes per episode, except in cases of intraoperative rupture, where prolonged occlusion was occasionally required. Clip placement was routinely confirmed intraoperatively with ICG angiography and micro-Doppler ultrasonography in all patients. Postoperative vascular imaging with CTA or DSA was not performed in all cases due to resource limitations but was selectively obtained in complex aneurysms, posterior circulation lesions, or when intraoperative findings were inconclusive.
All procedures were supported by experienced scrub nurses. Postoperative care was conducted in an intensive care unit under a standardized protocol for neurological monitoring and complication management.
All patients received nimodipine for vasospasm prophylaxis, administered orally or intravenously when needed. Upon signs of new neurological deficits suggestive of vasospasm, triple-H therapy (hypertension, hypervolemia, hemodilution) was initiated. If symptoms persisted or worsened, elective four-vessel angiography was performed, followed by intra-arterial nimodipine infusion when indicated. Transcranial Doppler (TCD) was not available during the study period.
Results
Patient Characteristics
Between July 2018 and June 2025, 478 patients with cerebral aneurysms were treated at a regional hospital in Thailand. Of these, 364 underwent microsurgical treatment and 114 received endovascular intervention, which became available in 2020. Among the surgical cases, 226 were performed by a single neurosurgeon. After excluding unruptured, complex, or elective cases, 189 patients who underwent microsurgical clipping for ruptured aneurysms during the acute phase were included in this study.
The mean age was 55.7 ± 11.1 years (range, 18–81), with a predominance of females (66.1%). Referrals primarily came from Lampang (n = 74), Phrae (n = 57), Nan (n = 38), and Tak (n = 16). Hypertension was the most common comorbidity (52.2%), while 42.3% had no recorded comorbidities. Baseline clinical and demographic characteristics are summarized in [Table 1].
Abbreviations: AcoMA, anterior communicating artery; AchOA, anterior choroidal artery; ICA, internal carotid artery; MCA, middle cerebral artery; PcoMA, posterior communicating artery; SD, standard deviation; WFNS, World Federation of Neurosurgical Societies.
Initial severity was assessed using WFNS grades: 59.3% were good grade (I–III), and 40.7% poor grade (IV–V). On the modified Fisher scale, 60.3% had grade 3 or 4 hemorrhage. The anterior communicating artery (AComA) was the most frequent aneurysm site (52.4%), followed by PComA (17.5%) and middle cerebral artery (MCA; 16.4%). Mean aneurysm diameter was 6.0 ± 3.1 mm, with 89.4% measuring <10 mm. Hydrocephalus on admission was present in 40.2%.
Timing and Operative Details
Surgery was performed ultra-early (<24 hours) in 58.2%, early (24–72 hours) in 22.2%, late (72 hours to 7 days) in 2.1%, and delayed (>7 days) in 17.5%. Intraoperative brain swelling occurred in 20.1%, and aneurysm rupture in 18.0%. The mean operative time was 173.9 minutes (range, 100–480), and median estimated blood loss was 200 mL (range, 50–600). Complete aneurysm occlusion was achieved in 96.8%. No intraoperative deaths were reported. Intraoperative findings stratified by timing and WFNS grade are detailed in [Table 2].
Abbreviations: ANOVA, Analysis of Variance; EBL, estimation of blood loss; SD, standard deviation; WFNS, World Federation of Neurosurgical Societies.
Note: Data are shown as number (%) or mean ± SD. Timing group comparisons were analyzed using Chi-square test for categorical variables and one-way ANOVA for continuous variables (Fisher's exact test applied where appropriate). WFNS group comparisons were analyzed using Chi-square test for categorical variables and Welch's t-test for continuous variables. Asterisks indicate statistical significance: *p < 0.05, **p < 0.01, ***p < 0.001.
Postoperative Vascular Imaging
Postoperative vascular imaging was not routinely performed but was selectively obtained in complex or uncertain cases. In total, 56 patients (29.6%) underwent postoperative vascular imaging: 31 had CTA, 28 had DSA, and 3 underwent both modalities.
Hydrocephalus Management
External ventricular drain was used in the acute phase as needed. Among patients with persistent hydrocephalus, 31.2% required permanent CSF diversion via ventriculoperitoneal or ventriculoatrial shunt.
Clinical Vasospasm
Clinical vasospasm occurred in 30 patients (15.9%). It was more frequent in poor-grade patients (16/75, 21.3%) than in good-grade patients (14/114, 12.3%). By surgical timing, vasospasm was observed in 16.4% of ultra-early, 19.0% of early, 0% of late, and 12.1% of delayed cases. All vasospasm cases occurred in the anterior circulation, most commonly involving the AComA (15 cases), PComA (five cases), and MCA (four cases). At 6 months, only 36.7% of patients with vasospasm achieved favorable outcome, while 30% died, compared with 82.2% favorable outcome in patients without vasospasm.”
Functional Outcomes
Functional status was assessed using the mRS at discharge, and at 1 month and 6 months. At discharge, 59.8% had favorable outcomes (mRS 0–2), and 5.3% had died. Among the 10 deaths, six were poor-grade patients who died from malignant vasospasm, and four were good-grade patients who died from rebleeding, acute respiratory distress syndrome (ARDS), or gastrointestinal (GI) bleeding.
Postoperative aneurysm rebleeding occurred in one patient (0.5%). This was a WFNS grade V patient with a PComA aneurysm, in whom intraoperative ICG and postoperative DSA initially confirmed complete clipping. The patient subsequently developed clip displacement and fatal rebleeding within 1 month. The imaging sequence of this case, illustrating initial occlusion and subsequent clip displacement with rebleeding, is shown in [Fig. 3]. At 1 month, 69.3% had favorable outcomes and mortality rose to 6.3% (n = 12) due to two post-discharge deaths. At 6 months, functional outcome analysis was performed using the intention-to-treat approach: 74.6% (141/189) achieved favorable outcomes (mRS 0–2), with no further deaths. This included eight patients from 2025 who had not yet reached the 6-month time point and were conservatively classified as unfavorable. Functional outcomes and mortality by WFNS grade and surgical timing are presented in [Table 3].

Abbreviations: mRS, modified Rankin Scale; WFNS, World Federation of Neurosurgical Societies.
Note: Favorable outcome defined as modified Rankin Scale (mRS) 0–2. WFNS comparisons used Chi-square test (two-group). Timing comparisons used overall Chi-square test across four groups; Fisher–Freeman–Halton exact test was considered where expected counts were <5 (e.g., Late group n = 4). Asterisks indicate statistical significance: *p < 0.05, **p < 0.01, ***p < 0.001.). All outcomes analyzed using intention-to-treat principle with non-responder imputation; denominator fixed at n = 189. Patients without complete 6-month follow-up (n = 8) were conservatively classified as unfavorable.
Subgroup Analysis
By WFNS Grade: poor-grade patients had lower 6-month favorable outcomes (58.7 vs. 85.1%, p < 0.001), higher shunt rates (52.0 vs. 17.5%, p < 0.001), longer hospital stays (median 13 vs. 10 days, p = 0.001), and higher treatment costs (median 186,851 vs. 120,724 THB, p < 0.001). Operative time and blood loss were not significantly different.
By operative period: Favorable outcomes at discharge improved from 30.3% in the initial phase to 40.5% in the substantial phase (2022–2025), particularly among poor-grade patients. Although subgroup comparisons did not reach statistical significance, the trend suggests institutional learning and procedural refinement benefiting even those with initially severe clinical grades.
By surgical timing: Among good-grade patients, 6-month favorable outcomes were 90.0% (ultra-early), 73.1% (early), and 89.5% (delayed). In poor-grade patients, earlier surgery was associated with better outcomes (ultra-early: 60.0%; early: 54.5%; delayed: 50.0%).
On multivariate analysis, poor WFNS grade (OR 0.33, p = 0.011) and vasospasm (OR 0.15, p < 0.001) were independent predictors of unfavorable outcome. Other variables—including hydrocephalus requiring shunt, operative time, blood loss, length of stay, and cost—were not independently associated.
Discussion
Despite the widespread use of endovascular techniques, microsurgical clipping remains essential for ruptured aneurysms in regional hospitals where emergent endovascular access is limited.[3] [5] [6] This study reflects real-world outcomes from a provincial hospital equipped with the surgical expertise and infrastructure to deliver effective care. Our results align with prior reports from high-volume regional centers, such as Leake et al,[6] underscoring the role of consistent surgical teams in achieving favorable outcomes. Timely access to clipping, supported by a stable team, remains a cornerstone of acute-phase aneurysm management.[7] [8]
Although this is a single-surgeon series, the findings represent the experience of the only referral center for aneurysm surgery in a region of approximately 1.4 million people. In this context, the outcomes may provide practical benchmarks for regional hospitals in resource-limited settings and complement the data from tertiary academic centers.
The outcomes in this single-surgeon series compare favorably with those reported in major studies. At 6 months, 74.6% of patients achieved functional independence, including 85.1% in good-grade and 58.7% in poor-grade groups. This aligns with the BRAT trial (77% favorable at 1 year) and exceeds the ISAT clipping arm (66%).[2] A comparative summary of selected microsurgical clipping studies is provided in [Table 4]. Our in-hospital mortality rate (5.3%) is also lower than the 7 to 11% range reported in BRAT, ISAT, and single-center series such as that of LeRoux et al.[9] [10] [11]
|
Study/Center |
Setting |
n |
WFNS Good (%) |
mRS 0–2 at 6 mo (%) |
Mortality (%) |
Shunt rate (%) |
Vasospasm (%) |
Cost (THB) |
Re-treatment (%) |
|---|---|---|---|---|---|---|---|---|---|
|
This study (Lampang) |
Regional, single surgeon |
189 |
59.3 |
74.6 |
6.3 |
31.2 |
15.9 |
Mean 175,982 |
0 |
|
BRAT (2013)[3] |
Academic center |
approx. 500+ |
approx. 70 |
77 (clip arm) |
10.6 |
17–20 |
NR |
Not reported |
approx. 1 |
|
ISAT (2005/2009)[2] |
Multicenter (Europe) |
2,143 |
Good grade only |
66 (clip arm) |
approx. 10 |
17 |
NR |
Much higher |
30–40 (coil) |
|
LeRoux (1998)[5] |
Single-center (US) |
approx. 100 |
NR |
71 (at DC) |
11 |
NR |
NR |
Not reported |
NR |
|
Leake et al (2011)[6] |
High-volume regional hospital |
approx. 200 |
Mixed |
72.5 |
6.5 |
approx. 20 |
NR |
Not reported |
0 |
Abbreviations: BRAT, Barrow Ruptured Aneurysm Trial; ISAT, International Subarachnoid Aneurysm Trial; mRS, modified Rankin Scale; NR, not reported; THB, Thai Baht; WFNS, World Federation of Neurosurgical Societies.
Note: Favorable outcome defined as mRS 0 to 2. This table compares clinical outcomes, shunt rate, vasospasm incidence, treatment cost, and re-treatment rates from selected microsurgical clipping series. Data from BRAT[3] and ISAT[2] refer to the surgical arm. Leake et al[6] reported outcomes from a high-volume regional hospital, demonstrating results comparable to academic centers.
Subgroup analysis further elucidated the impact of WFNS grade, surgical timing, and procedural refinement—particularly in poor-grade SAH. These insights may inform treatment strategies in regional or resource-limited settings.
Another major determinant of outcome after aneurysmal SAH is vasospasm. In this series, clinical vasospasm occurred in 30 patients (15.9%), all involving anterior circulation aneurysms, most commonly the AComA and PComA. This incidence lies at the lower end of the 20 to 40% reported in large series such as BRAT and ISAT, where symptomatic vasospasm was observed in 20 to 24% of patients, and in single-center cohorts where rates approached 25%.[2] [6] [9] Differences in case mix and diagnostic thresholds may account for this variation, and under-reporting of milder or transient cases cannot be excluded in a retrospective review. Outcomes in patients with vasospasm were predictably worse, with only 36.7% achieving functional independence and 30% mortality, underscoring the devastating impact of malignant vasospasm in poor-grade patients. While aggressive cisternal irrigation was consistently performed to clear subarachnoid blood, the present data cannot establish a causal effect on vasospasm incidence, and further study is warranted.
One factor contributing to the relatively long mean operative time (173.9 minutes) was the emphasis on aggressive cisternal irrigation during arachnoid dissection. Unlike conventional dissection limited to clip placement, this technique involved clearing subarachnoid blood from the basal cisterns to enhance CSF flow. Though further validation is needed, the low rate of delayed cerebral ischemia in this series suggests potential long-term benefit.
While overall mortality was low (6.3%), case review revealed key patterns. Among poor-grade patients, six died in-hospital from malignant vasospasm, and two post-discharge from pneumonia and rebleeding. These findings highlight the ongoing lethality of vasospasm and the need for extended monitoring in this group.
In contrast, all four deaths in good-grade patients occurred in-hospital despite initial recovery. Causes included delayed vasospasm, rebleeding before surgery, ARDS, and upper GI bleeding. This underscores the importance of perioperative vigilance—not only for neurological decline but also for systemic complications, even in seemingly stable patients. A rebleeding case in a poor-grade patient also highlighted the need for meticulous clip application in difficult exposures. In deep or swollen operative fields, full neck exploration under high magnification is critical, and clip reinforcement or the use of fenestrated blades with higher closing force may reduce the risk of delayed failure.
While ISAT favored coiling in select good-grade anterior circulation aneurysms, long-term follow-up revealed higher rebleeding and re-treatment rates compared with clipping.[2] [12] BRAT also showed increased re-treatment in coiled patients (41 vs. 1%),[9] reinforcing clipping's long-term advantage. Meta-analyses suggest that poor-grade SAH, posterior circulation aneurysms, and younger patients may benefit more from clipping.[13] [14] In our series, which included 40.7% poor-grade patients, favorable outcomes (74.6%) and low mortality support clipping's continued relevance. Importantly, no patient in this study required re-treatment, underscoring the durability of high-quality microsurgical repair—especially in regional centers with timely access and experienced teams.
Contributing factors included continuity of care by a single neurosurgeon and the consistent use of micro-Doppler ultrasonography, ICG angiography, and careful CSF release to reduce the rupture risk. Unlike academic centers, these surgeries were supported not by trainees but by trained scrub nurses familiar with the lead surgeon's workflow. This stable team likely enhanced procedural consistency—especially during key steps like sylvian dissection and clip placement.
Early in the study, a keyhole approach was occasionally used to follow global trends toward minimalism. Over time, this shifted to a “maximum effective surgery” model—favoring standard craniotomies that prioritized safety, clarity, and team consistency over smaller exposures. This approach proved more practical for emergency settings with rotating nursing staff, allowing key steps like sylvian dissection to proceed reliably. Small incisions were still used selectively for cosmetic reasons when surgical exposure was not compromised.
The transsylvian approach is viewed as the gateway to aneurysm surgery, with Sylvian vein dissection allowing frontal–temporal lobe separation. The Takayama scissors—modeled after a katana tip—enabled precise arachnoid dissection under high magnification. Once the Sylvian fissure is open, basal and even posterior circulation cisterns become accessible. This technique is illustrated in [Fig. 1], which demonstrates intraoperative dissection, irrigation, and postoperative clearance of subarachnoid blood.
The author emphasizes intraoperative clearance of subarachnoid blood during this phase to improve CSF dynamics and potentially reduce vasospasm. Although the evidence remains limited, this strategy may explain the favorable outcomes seen in this series and warrants future study.
The average treatment cost (mean 175,982 THB) was substantially lower than typical endovascular care, reinforcing the cost-effectiveness of clipping in regional hospitals. This study also demonstrates that non-academic centers can achieve outcomes comparable to tertiary hospitals—supporting investment in decentralized neurosurgical care. With focused training, consistent teams, and essential tools, regional centers can sustainably deliver equitable treatment in underserved areas.
While coiling is often favored for good-grade anterior circulation aneurysms, evidence suggests that clipping can yield comparable or better outcomes in selected patients—especially when performed by experienced surgeons. Clipping also eliminates the need for follow-up angiography or re-treatment, making it preferable in younger patients or those without long-term imaging access.[15] In our series, many good-grade anterior circulation aneurysms were clipped as first-line treatment, with favorable results.
That said, coiling remains valuable in posterior circulation, poor-grade, or high-risk patients. Rather than basing treatment on practitioner background, outcomes improve when both modalities are considered through a balanced, collaborative approach.[16] [17] The development of “Micro–Endo” teams—even in regional hospitals—can help optimize modality selection and ensure personalized, pathology-driven care.
Limitations and Future Directions
This study has several limitations. First, its retrospective, single-center, single-surgeon design may limit the generalizability of the findings to broader clinical settings. Second, the lack of a comparator arm—such as endovascular or conservative treatment—precludes direct evaluation of relative treatment efficacy. Third, vasospasm diagnosis was based primarily on clinical signs, with limited use of confirmatory angiography, which may have led to underestimation of its true incidence. Fourth, postoperative vascular imaging with CTA or DSA was not performed routinely but selectively in complex or uncertain cases due to resource limitations, which may have resulted in under-detection of small remnants compared with studies using standardized imaging. Fifth, follow-up was limited to 6 months; long-term outcomes such as quality of life, cognitive function, and delayed complications were not systematically assessed. While the single-surgeon design may limit generalizability, it also ensured consistency of surgical technique and perioperative management, which can be valuable for interpreting outcomes in regional referral hospitals.
Future research should address these gaps through prospective studies incorporating objective vasospasm monitoring, long-term functional and neurocognitive follow-up, and comparative analyses between microsurgical and endovascular modalities—especially in poor-grade or complex aneurysms. Multicenter collaborations could help validate the reproducibility of techniques such as aggressive cisternal irrigation across different practice environments.
Of particular interest is the emerging role of hybrid strategies that combine microsurgical and endovascular approaches in a single-session or coordinated workflow. Although this series did not include such cases, the implementation of intraoperative fluoroscopy and collaboration with neurointerventionists at our center has laid the groundwork for future hybrid protocols, even in the absence of a formal Hybrid Operating Room. Systematic evaluation of these approaches may help define their utility in regional hospitals, particularly for challenging aneurysms requiring both modalities. Additionally, the integration of multidisciplinary neurovascular teams and shared decision-making frameworks may serve as a model for delivering sustainable, high-quality cerebrovascular care beyond academic institutions.
Conclusion
This study underscores the continued importance of microsurgical clipping in managing ruptured cerebral aneurysms, particularly in regional hospitals where emergent endovascular access may be limited. With consistent surgical expertise and perioperative care, outcomes comparable to academic centers are achievable. Subgroup analysis highlights the influence of surgical timing and patient selection. Microsurgical clipping remains a durable and effective option when performed by experienced hands within a structured team-based approach.
Conflict of Interest
None declared.
Acknowledgment
The author gratefully acknowledges Dr. Kannachod Chanvanitkulchai, neurointerventionist, for his valuable input and collaborative discussions in the management planning of aneurysm cases.
Note
ChatGPT (OpenAI, 2024) was utilized for language editing and grammar refinement during manuscript preparation.
Ethical Approval
Approved by the Institutional Review Board of Lampang Hospital (IRB No. EC 145/68). The study was conducted in accordance with the Declaration of Helsinki.
-
References
- 1 Connolly Jr ES, Rabinstein AA, Carhuapoma JR. et al; American Heart Association Stroke Council, Council on Cardiovascular Radiology and Intervention, Council on Cardiovascular Nursing, Council on Cardiovascular Surgery and Anesthesia, Council on Clinical Cardiology. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2012; 43 (06) 1711-1737
- 2 Molyneux AJ, Kerr RS, Yu LM. et al. ISAT Collaborators. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2005; 366 (9488) 809-817
- 3 Hoh BL, Ogilvy CS. Endovascular management of intracranial aneurysms: current experience and future advances. Lancet Neurol 2004; 3 (10) 605-612
- 4 Hoh BL, Ogilvy CS. Surgical management of unruptured intracranial aneurysms. J Neurosurg 2011; 114 (03) 603-607
- 5 LeRoux PD, Elliott JP, Eskridge JM. et al. Risk and benefit of surgical vs endovascular therapy for acutely ruptured cerebral aneurysms. Neurosurgery 1998; 43 (06) 1235-1246
- 6 Leake CB, Brinjikji W, Kallmes DF. et al. Microsurgical clipping in the modern era: a single-institution experience with aneurysm treatment. J Neurosurg 2011; 114 (03) 641-648
- 7 Guresir E, Schuss P, Vatter H. et al. Rapid ventricular pacing for clip reconstruction of complex anterior circulation aneurysms: a single-center series. Stroke 2011; 42 (07) 1897-1903
- 8 Komotar RJ, Zacharia BE, Otten ML. et al. Controversies in the management of ruptured intracranial aneurysms: endovascular coiling versus microsurgical clipping. Neurosurg Focus 2009; 26 (05) E11
- 9 Spetzler RF, McDougall CG, Zabramski JM. et al. The barrow ruptured aneurysm trial: 6-year results. J Neurosurg 2015; 123 (03) 609-617
- 10 Johnston SC, Higashida RT, Barrow DL. et al; Committee on Cerebrovascular Imaging of the American Heart Association Council on Cardiovascular Radiology. Recommendations for the endovascular treatment of intracranial aneurysms: a statement for healthcare professionals from the Committee on Cerebrovascular Imaging of the American Heart Association Council on Cardiovascular Radiology. Stroke 2002; 33 (10) 2536-2544
- 11 Raaymakers TW, Rinkel GJ, Limburg M, Algra A. Mortality and morbidity of surgery for unruptured intracranial aneurysms: a meta-analysis. Stroke 1998; 29 (08) 1531-1538
- 12 Campi A, Ramzi N, Molyneux AJ. et al. Retreatment of ruptured cerebral aneurysms in patients randomized by coiling or clipping in the International Subarachnoid Aneurysm Trial (ISAT). Stroke 2007; 38 (05) 1538-1544
- 13 Guresir E, Schuss P, Vatter H. et al. Natural history of poor-grade aneurysmal subarachnoid hemorrhage: a single-center study. Neurosurgery 2011; 68 (06) 1731-1738
- 14 Dasenbrock HH, Rudy RF, Smith TR. et al. Comparison of clipping and coiling of unruptured aneurysms in elderly patients: a cohort study. J Neurosurg 2017; 126 (03) 811-819
- 15 Hino A, Fujimoto M, Iwamoto Y. et al. Surgery of ruptured anterior communicating artery aneurysms: significance of aneurysm projection and direction. Acta Neurochir (Wien) 1995; 133 (3–4): 129-135
- 16 Amenta PS, Starke RM, Jabbour PM. et al. Update on endovascular and microsurgical treatment of intracranial aneurysms. Neurosurg Focus 2012; 33 (05) E2
- 17 Peluso JP, van Rooij WJ, Sluzewski M. et al. Coiling of anterior communicating artery aneurysms: incidence of aneurysm recurrence and risk factors. AJNR Am J Neuroradiol 2008; 29 (01) 52-54
Address for correspondence
Publication History
Article published online:
14 January 2026
© 2026. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Connolly Jr ES, Rabinstein AA, Carhuapoma JR. et al; American Heart Association Stroke Council, Council on Cardiovascular Radiology and Intervention, Council on Cardiovascular Nursing, Council on Cardiovascular Surgery and Anesthesia, Council on Clinical Cardiology. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2012; 43 (06) 1711-1737
- 2 Molyneux AJ, Kerr RS, Yu LM. et al. ISAT Collaborators. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2005; 366 (9488) 809-817
- 3 Hoh BL, Ogilvy CS. Endovascular management of intracranial aneurysms: current experience and future advances. Lancet Neurol 2004; 3 (10) 605-612
- 4 Hoh BL, Ogilvy CS. Surgical management of unruptured intracranial aneurysms. J Neurosurg 2011; 114 (03) 603-607
- 5 LeRoux PD, Elliott JP, Eskridge JM. et al. Risk and benefit of surgical vs endovascular therapy for acutely ruptured cerebral aneurysms. Neurosurgery 1998; 43 (06) 1235-1246
- 6 Leake CB, Brinjikji W, Kallmes DF. et al. Microsurgical clipping in the modern era: a single-institution experience with aneurysm treatment. J Neurosurg 2011; 114 (03) 641-648
- 7 Guresir E, Schuss P, Vatter H. et al. Rapid ventricular pacing for clip reconstruction of complex anterior circulation aneurysms: a single-center series. Stroke 2011; 42 (07) 1897-1903
- 8 Komotar RJ, Zacharia BE, Otten ML. et al. Controversies in the management of ruptured intracranial aneurysms: endovascular coiling versus microsurgical clipping. Neurosurg Focus 2009; 26 (05) E11
- 9 Spetzler RF, McDougall CG, Zabramski JM. et al. The barrow ruptured aneurysm trial: 6-year results. J Neurosurg 2015; 123 (03) 609-617
- 10 Johnston SC, Higashida RT, Barrow DL. et al; Committee on Cerebrovascular Imaging of the American Heart Association Council on Cardiovascular Radiology. Recommendations for the endovascular treatment of intracranial aneurysms: a statement for healthcare professionals from the Committee on Cerebrovascular Imaging of the American Heart Association Council on Cardiovascular Radiology. Stroke 2002; 33 (10) 2536-2544
- 11 Raaymakers TW, Rinkel GJ, Limburg M, Algra A. Mortality and morbidity of surgery for unruptured intracranial aneurysms: a meta-analysis. Stroke 1998; 29 (08) 1531-1538
- 12 Campi A, Ramzi N, Molyneux AJ. et al. Retreatment of ruptured cerebral aneurysms in patients randomized by coiling or clipping in the International Subarachnoid Aneurysm Trial (ISAT). Stroke 2007; 38 (05) 1538-1544
- 13 Guresir E, Schuss P, Vatter H. et al. Natural history of poor-grade aneurysmal subarachnoid hemorrhage: a single-center study. Neurosurgery 2011; 68 (06) 1731-1738
- 14 Dasenbrock HH, Rudy RF, Smith TR. et al. Comparison of clipping and coiling of unruptured aneurysms in elderly patients: a cohort study. J Neurosurg 2017; 126 (03) 811-819
- 15 Hino A, Fujimoto M, Iwamoto Y. et al. Surgery of ruptured anterior communicating artery aneurysms: significance of aneurysm projection and direction. Acta Neurochir (Wien) 1995; 133 (3–4): 129-135
- 16 Amenta PS, Starke RM, Jabbour PM. et al. Update on endovascular and microsurgical treatment of intracranial aneurysms. Neurosurg Focus 2012; 33 (05) E2
- 17 Peluso JP, van Rooij WJ, Sluzewski M. et al. Coiling of anterior communicating artery aneurysms: incidence of aneurysm recurrence and risk factors. AJNR Am J Neuroradiol 2008; 29 (01) 52-54