

Subscribe to RSS
DOI: 10.1055/s-0045-1814741
Photodynamic Therapy for Head and Neck Cancers: A Review of a Novel, Patient-Friendly Solution and Prospects
Authors
Funding and Sponsorship This study was funded by the MATCH grant fund of the Ministry of Higher Education Malaysia (MOHE), project code 203.PPSP.6782007.

Abstract
Background
Head and neck cancers (HNCs) are among the six most common malignancies worldwide, with incidence projected to increase substantially by 2030. Although surgery and chemoradiation remain effective standard treatments, they are often costly, less accessible, and associated with significant functional and aesthetic morbidity. Photodynamic therapy (PDT) has emerged as a promising alternative due to its safety profile, cost-effectiveness, and ability to preserve vital structures.
Materials and Methods
This narrative review examined preclinical and clinical studies evaluating PDT for HNC. A structured literature search was conducted in PubMed, Scopus, and Web of Science using terms such as “photodynamic therapy,” “head and neck cancer,” “oral squamous cell carcinoma,” “minimally invasive therapy,” “photoimmunotherapy,” “photochemical internalization,” and “nanoparticle delivery.” Only English-language, peer-reviewed articles reporting on the efficacy, safety, or mechanisms of PDT were included. Eligible studies were selected based on relevance to clinical application and innovation, and findings were organized thematically to highlight therapeutic outcomes, patient-centered advantages, and translational developments supporting broader clinical integration.
Findings
PDT demonstrates several key advantages over conventional treatments, including high tumor specificity, reduced toxicity, preservation of normal tissues, and suitability for outpatient care. These benefits are especially valuable in low-resource settings. PDT also supports better functional and aesthetic outcomes by minimizing scarring and reducing hospital stays. Its compatibility with other modalities, such as chemotherapy, radiotherapy, and immunotherapy, further enhances its role in multimodal treatment strategies. Technological progress, particularly in nanoparticle-based photosensitizers and targeted light delivery, has markedly improved the precision and effectiveness of PDT.
Conclusion
PDT holds strong potential as a safe, accessible, and cost-effective treatment for HNCs. Its favorable therapeutic profile, combined with expanding technological innovations, positions PDT as an important and increasingly relevant option within future oncologic care.
Keywords
minimally invasive therapy - targeted cancer treatment - nanoparticle therapy - photochemical internalization - photoimmunotherapy - salvage therapyIntroduction
Head and neck squamous cell carcinoma (HNSCC) is a heterogeneous group of malignancies arising from the mucosal epithelium of the upper aerodigestive tract, encompassing cancers of the oral cavity, pharynx, and larynx. It represents the sixth most common cancer worldwide, with approximately 570,000 new cases and 294,000 deaths reported in 2022. HNSCC predominantly affects older males and is linked to environmental and lifestyle factors such as tobacco use and alcohol consumption. However, there is an increasing trend in younger individuals due to human papillomavirus (HPV) infection, which has been linked to cancers at the oropharyngeal subsites.[1] [2]
Conventional treatments for HNCs include surgery, radiotherapy, and chemotherapy. However, the treatment approach depends on the anatomical subsite, stage, disease characteristics, functional considerations, and patient wishes.[3] Surgery and radiotherapy usually have good treatment outcomes in the early stages of HNC. However, both treatment modalities affect the functional capabilities of patients.[4] Photodynamic therapy (PDT) is a recently advocated therapeutic option that has been reported to be effective in treating head and neck dysplasia and cancer.[5] [6]
HNCs occupy most visible and functionally vital areas of the body, where both the disease and its treatment can significantly impact a patient's speech, swallowing, appearance, and overall quality of life (QoL). Given our interest in advancing care in this challenging field, we chose to focus this review on PDT as a promising alternative to conventional treatment modalities. This review explores the distinct advantages and innovative aspects of PDT in the management of HNCs, highlighting evidence from relevant clinical studies that demonstrate its practical benefits. Furthermore, we discuss the prospects of PDT, aiming to inspire further interest and research in this patient-centered approach.
Photodynamic Therapy
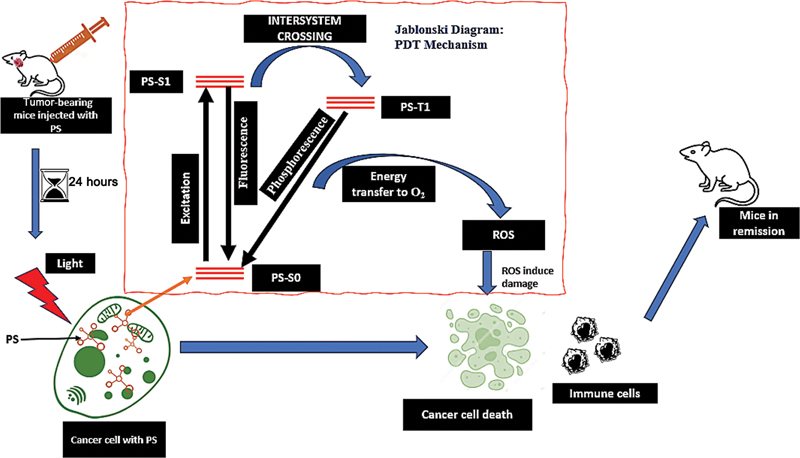
PDT results from the interaction of light-sensitive substances called photosensitizers (PSs), light of an appropriate wavelength, and cellular oxygen. The output of the interaction of this trio is the selective destruction of targeted cells.[7] PDT is a two-step process. First, a PS is administered to the patient, topically, orally, or intravenously, and some time is given for the PS to accumulate in the tumor. Second, the PS-laden tumor is exposed to light of a specific wavelength to activate the PS. Following activation of the PS, a cascade of activity will culminate in the conversion of cellular oxygen to reactive oxygen species (ROS), such as excited singlet oxygen, which kills tumor cells (by inducing apoptosis, necrosis, or autophagy), destroys tumor vasculature, and initiates an immune response.[7] [8] [9] The steps involved in PDT and its mechanism of action are shown in [Fig. 1].
The choice of PS is essential for optimal cancer treatment using PDT. An ideal PS should be pure, nontoxic in the dark, nonmutagenic, cheap, easily activated at the required wavelength of light, have good singlet oxygen quantum yield, and have good pharmacokinetic properties. PSs are classified into first-, second-, and third-generation PSs based on their chemical structure. First-generation PSs (Photofrin) cause longer phototoxicity than second-generation PSs (Foscan), whose chemical structures have been optimized. Third-generation PSs have been developed to reduce these phototoxic effects. They are made by encapsulating second-generation PSs into nanoparticles or coupling them to vectors targeting receptors such as low-density lipoprotein (LDL), peptides, folic acid, or monoclonal antibodies; hence, they are more targeted to tumor cells.[10] [11] The biodistribution of PS is due to its affinity for LDL. Dividing cancer cells upregulates LDL receptors, which allows for the increased uptake of LDL and accumulation of PSs.[7]
Light plays a central role in PDT, acting as the activator of the PS to produce cytotoxic ROS that destroy target cells. Effective light delivery maximizes treatment precision, spares surrounding healthy tissue, and contributes to favorable outcomes in cancer therapy. The characteristics of light, such as wavelength, fluence, power density, and duration, directly impact therapeutic efficacy. PDT commonly utilizes red or near-infrared (NIR) light (600–800 nm), which offers optimal tissue penetration and efficient PS activation. A wide range of light sources is used in PDT, including lasers, light-emitting diodes (LEDs), and broadband lamps. Lasers offer high coherence and precision, making them ideal for localized tumors, while LEDs are cost-effective and adaptable to various clinical needs.[12] [13] [14] Kim and Darafsheh[13] note that advancements such as interstitial and endoscopic light delivery systems, fiberoptics, and diffusing tips have significantly improved the capacity to treat deep-seated or bulky tumors by delivering light directly to or within tissue masses.
While this review primarily highlights the novel advantages of PDT over conventional treatments, this treatment modality, like other treatment modalities, also presents limitations. Key challenges include limited light penetration depth, which restricts its use in treating deeply seated or bulky tumors; the need for specialized light sources and dosimetry equipment, which may not be widely available; and barriers to broader clinical adoption due to logistical, infrastructural, and training constraints. Additionally, PDT is associated with early side effects such as localized pain and skin reactions, and late effects like hyperpigmentation[15] or the development of immune response imbalances—described by the “immunocompromised district” concept. Mitigation strategies include the use of topical nicotinamide (vitamin B3), analgesia, immediate posttreatment cooling, and daylight PDT, where PSs are activated by natural sunlight. Despite these limitations, continued refinement of PDT technologies and protocols continues to expand its therapeutic potential.[16]
Novel Aspect of PDT
Conventional treatments for head and neck cancers (HNCs)—such as surgery, radiotherapy, and chemotherapy—can significantly compromise patients' QoL. Surgery may cause functional and cosmetic deficits, while radiotherapy and chemotherapy often lead to systemic toxicity, mucosal damage, and immunosuppression. These therapies also face challenges with precision, cumulative side effects, and limited suitability for recurrent or inoperable cases.
PDT presents a compelling alternative, offering tumor-selective cytotoxicity, minimal invasiveness, and low systemic toxicity. It preserves organ function and aesthetics, supports repeat treatment, and is cost-effective in appropriate contexts. PDT is especially valuable for early-stage, superficial, or recurrent tumors unsuitable for conventional approaches.
Materials and Methods
This narrative review examined preclinical and clinical studies on PDT in HNC. A structured literature search was performed in PubMed, Scopus, and Web of Science using terms including “photodynamic therapy,” “head and neck cancer,” “oral squamous cell carcinoma,” “minimally invasive therapy,” “photoimmunotherapy,” “photochemical internalisation,” and “nanoparticle delivery.”
Only English-language, peer-reviewed articles reporting on the efficacy, safety, or underlying mechanism of PDT were included. Studies were selected based on their relevance to clinical application and innovation. The literature was organized thematically to emphasize therapeutic outcomes, patient-centered advantages, and translational developments supporting wider clinical integration of PDT.
Advantages of PDT for HNCs
Precision Targeting of Lesions
PDT exhibits selective cytotoxicity toward cancer cells due to preferential PS accumulation within malignant tissues or through targeted light delivery. When activated by light, the PS generates ROS that induce cancer cell death and initiate subsequent biological responses. In the surgical management of HNC, achieving clear margins often requires the excision of surrounding normal tissues, and extensive resections can impair essential functions. For example, glossectomy may involve the removal of intrinsic and extrinsic tongue muscles, resulting in difficulties with speech and swallowing. Surgical treatment in other head and neck regions may also compromise nerves, blood vessels, and adjacent critical structures, and the limitations in surgical precision contribute to the challenge of consistently achieving margin-free resections.[17]
Radiotherapy, despite careful planning, is associated with significant early and late tissue toxicity.[18] Chemotherapy, historically the least targeted modality, is often feared by patients due to its systemic effects on healthy tissues, which may manifest as alopecia, hyperpigmentation, hematologic disorders, gastrointestinal disturbances, and mucosal ulceration.[19] Lou et al[20] demonstrated effective treatment of HNC using PDT, including in tumors situated near vital structures. Patients with nerve compression frequently experience symptom relief following PDT, and unlike surgery or radiotherapy, PDT preserves nerve function. In practice, light is delivered directly over the lesion and slightly beyond its margins, while other areas are shielded. Even in anatomically complex regions, PDT maintains nerve integrity and may affect vascular architecture without causing hemorrhage.
Less Invasive than Traditional Surgical Procedures
PDT for superficially located HNC is minimally invasive, requiring only PS administration, followed by targeted light activation at the tumor site. Although endoscopic light delivery introduces a degree of invasiveness, it rarely damages surrounding normal tissues. In the treatment of nasopharyngeal carcinoma, the light source is introduced into the nasopharynx through the nostrils to ensure direct illumination of the tumor while sparing adjacent structures. In contrast, traditional surgical techniques for HNC are substantially more invasive and are frequently associated with postoperative complications. Recent surgical innovations, including laser micro-cautery and transoral robotic surgery, have reduced invasiveness, lowered complication rates, shortened hospital stays, and decreased postoperative care needs.[21] Nevertheless, PDT remains one of the least invasive treatment options, even when compared with these advanced surgical approaches.
Rapid Outpatient Care
PDT provides an outpatient-friendly approach for managing HNCs, unlike the prolonged and resource-intensive processes associated with surgery and radiotherapy. PDT can be delivered efficiently through PS administration, followed by light activation on the same day. Several anterior oral cancers and dysplastic lesions have been successfully treated in outpatient settings without topical or local anesthesia.[6] For deeper tumors such as nasopharyngeal carcinoma, PDT can also be administered under local anesthesia, with the light source introduced transnasally to illuminate the nasopharynx directly.[22] In contrast, surgical management of HNC requires extensive preoperative evaluation, patient optimization, and assessment by experienced anesthetists, followed by postoperative monitoring and structured follow-up. Perioperative challenges may arise at the preoperative, intraoperative, and postoperative stages, and the timing of surgery often depends on the availability of skilled personnel and suitable facilities.[17] [21] Radiotherapy also cannot be initiated promptly nor performed on an outpatient basis. It requires access to specialized radiotherapy units, detailed treatment planning, CT-based tumor mapping, and trained personnel, all constrained by equipment availability and institutional capacity.[23]
The outpatient nature of PDT positions it as a flexible therapeutic option that can be initiated during surgical or radiotherapy planning phases without concerns about treatment resistance. Its ability to be delivered promptly and safely in ambulatory settings underscores its potential to complement other treatment modalities. To maximize clinical benefit, careful consideration of both procedural and timing factors is essential when integrating PDT into HNC management.
No Long-Term Side Effects
PDT is associated with minimal and short-lived side effects, in contrast to the acute and chronic complications frequently encountered with surgery and radiotherapy for HNC. Surgical treatment remains the optimal option for early-stage HNC because it allows direct removal of the tumor along with adjacent functional tissues. However, radical surgery often necessitates excising substantial amounts of normal tissue to achieve negative margins. For example, partial or total glossectomy for tongue cancer can impair speech, swallowing, and oral function, while also causing noticeable disfigurement. Similarly, partial or total laryngectomy compromises phonation, with profound psychological effects, particularly among individuals who rely on their voices, such as singers. Reconstructive surgery and rehabilitative care may mitigate these functional deficits when appropriate expertise is available.[24] [25]
Radiotherapy, another widely used modality for HNC, may be delivered alone or in combination with surgery or chemotherapy. It effectively eradicates cancer cells through ionizing radiation and is particularly beneficial for early-stage disease. Nonetheless, radiotherapy is associated with numerous side effects that can significantly affect patient well-being. Acute toxicities typically resolve within 3 weeks after treatment completion, whereas late or chronic toxicities may persist for months to years. The likelihood and severity of these complications depend on the total radiation dose, duration of exposure, and the specific head and neck regions irradiated. Chronic adverse effects may include xerostomia, dental caries, osteoradionecrosis, trismus, secondary skin cancers, pharyngeal stenosis, lymphedema, vision loss, and nerve damage.[26] [27]
Preclinical and in vitro studies demonstrate that PDT is safe for neurovascular structures, even at high doses. Wright et al[28] reported that rat neurons tolerated cytotoxic PDT doses and subsequently regrew neurites. Kübler et al[29] observed significant histological changes without vascular rupture or neurological deficits, despite noting 75% nerve demyelination in a rabbit model. A separate study[30] found that PDT-induced vascular injury in a rat model was reversible, with full recovery occurring within 2 weeks. Although complications such as fistula formation and carotid blowout have occasionally been reported following PDT for HNC, most PDT-related adverse effects are mild, nondisabling, and resolve quickly, preserving patients' functional status.[31] [32] [33]
Minimal Effect on Quality of Life
PDT has been shown to significantly improve the health-related QoL of patients with HNC, with reported benefits across social functioning, anxiety reduction, daily living, and mood, without notable adverse effects. QoL reflects the extent to which an individual's physical, mental, social, and spiritual well-being is affected by a specific illness or its management, including malignancies and other acute or chronic diseases.[34] Surgery and chemoradiotherapy have been reported to affect the QoL and body image distress of patients treated with these modalities.[24] [35] Jerjes et al[36] evaluated QoL outcomes in 38 patients treated for various head and neck pathologies after a mean follow-up of 56 days. All patients received PDT to the head and neck region using meta-tetra(hydroxyphenyl)chlorin (mTHPC) as the PS, and all reported improved QoL, demonstrated by significant enhancements in social life, daily functioning, and mood, and reduced anxiety. In a study of 128 patients with recurrent or refractory HNSCC, 61% experienced a clinical QoL improvement, defined as normalization or a gain of ≥2 grades in at least one University of Washington Quality-of-Life (UWQOL) domain: pain, disfigurement, speech, chewing, or swallowing.[15]
Minimal Scarring Posttreatment
PDT is a potentially more acceptable treatment option for HNC because it is associated with minimal and largely temporary side effects, unlike the visible scarring commonly seen after surgery or radiotherapy. Surgical treatment in cosmetically sensitive regions may result in noticeable scars, skin loss, or distortion of the oral commissure, while radiotherapy can contribute to pigmentary skin changes that negatively affect body image.[37] In contrast, PDT rarely causes scarring; most studies report only transient erythema that resolves quickly, enhancing its acceptability as a treatment option.[33]
Although uncommon, isolated reports describe PDT-related effects. Karakullukcu et al[38] noted a few cases of second-degree burns due to noncompliance with light-protection guidelines, all of which healed with conservative management. They also reported mild permanent discoloration at the injection site in some patients and buccal mucosal scarring in a small subset, leading to mild or moderate trismus managed successfully with stretching exercises. These findings remain exceptions and do not alter the overall favorable cosmetic profile of PDT compared with conventional treatments.
Allows for Repeated Treatment at the Same Sites
PDT can be safely repeated at the same site with minimal complications.[39] In contrast, repeated surgery in previously treated areas is associated with higher morbidity. Reoperation for recurrent disease is technically challenging due to fibrosis, altered tissue planes, and wound-healing changes, all of which increase the risk of complications compared with the initial procedure. Repeated radiotherapy similarly damages surrounding normal tissues, resulting in long-term postradiation sequelae. Multiple courses of chemotherapy can cause significant bone marrow suppression, compromising the patient's immune status, and both radiotherapy and chemotherapy carry a risk of inducing secondary malignancies.[25] Moreover, repeated PDT has demonstrated effectiveness against metastatic disease, partly through the induction of abscopal effects, whereby local treatment generates a systemic immune response capable of controlling or eliminating distant, untreated tumors.[22]
Relatively Cost-Effective
Cost-effectiveness evaluations across multiple settings consistently demonstrate that PDT delivers meaningful clinical benefit at a lower overall cost than several standard treatment modalities. In Germany, the total cost of a complete Foscan-mediated PDT course (€8,761) was substantially lower than that of chemotherapy (€11,600).[40] A related United Kingdom analysis by Hopper et al[41] reported similar findings: Foscan-PDT had the lowest unit cost (£5,741) compared with palliative chemotherapy (£9,924) and extensive palliative surgery (£16,912). Even when comparator costs were reduced, Foscan-PDT remained cost-effective at £14,206 per life-year saved and dominated chemotherapy and surgery when three or more chemotherapy cycles were included. Both studies also showed that PDT provided the greatest health-related effectiveness for advanced HNC, prolonging survival by 129 days compared with no treatment and by 48 days compared with four cycles of palliative chemotherapy.
The economic advantages of PDT extend to other malignancies. In early-stage lung cancer, PDT demonstrated markedly reduced overall treatment costs compared with lobectomy (¥1,017,104 vs. ¥1,793,832). When evaluated using quality-adjusted life years, the cost-effectiveness of PDT (¥30,003 per postoperative living month) was 1.3 to 1.5 times greater than that of surgery, with the greatest advantage observed in tumors smaller than 2 cm.[42]
Collectively, these findings show that PDT is a cost-effective alternative capable of achieving meaningful tumor responses, facilitating remission, and extending life expectancy.
High Response Rates in Challenging Head and Neck Cancers
Surgery is widely regarded as the standard treatment for early-stage HNC. However, a meta-analysis by Cerrati et al[43] found no significant difference in treatment outcomes between surgery and PDT for early-stage disease. A systematic review of 26 studies assessing the efficacy of PDT in HNC reported complete response rates ranging from 16 to 100%.[44] In another systematic review, Liu et al[45] noted that despite its minimally invasive nature, PDT shows strong potential for controlling the recurrence of oral precancerous lesions. [Table 1] summarizes key studies demonstrating the remarkable therapeutic outcomes of PDT in managing HNCs, including scenarios in which conventional treatments are not feasible or have limited effectiveness.
|
Study |
Photosensitizer |
No. of cases |
Characteristics of cases |
Response |
Outcome |
|||
|---|---|---|---|---|---|---|---|---|
|
CR |
PR |
SD |
PD |
|||||
|
Karakullukcu et al[38] |
Meta-tetra(hydroxyphenyl)chlorin (mTHPC) |
170 |
Early-stage (Tis, T1, T2) oral cavity and oropharynx squamous cell carcinoma (SCC) or Cis |
70.8% |
19.9% |
Overall mean survival Primary tumor: 120.4 mo Nonprimary tumor: 82.1 mo |
||
|
Lorenz and Maier[70] |
mTHPC |
35 |
Salvage treatment for recurrent cases or cases with secondary HNC tumors |
21 |
10 |
4 |
Median survival: 356 d |
|
|
Stoker et al[22] |
mTHPC |
21 |
Residual/recurrent nasopharyngeal carcinoma (depth, <10 mm) |
20 |
Overall survival: 65% |
|||
|
Lou et al[31] |
mTHPC |
45 |
Salvage treatment for recurrent cases |
9 |
24 |
6 |
6 |
Median survival (CR + PR): 16 mo |
|
Schweitzer[71] |
Photofrin |
20 |
Early-stage Tis-T2N0M0 SCC of the oral cavity and oropharynx (10 cases) and 10 patients with Tis-T2N0M0 SCC of the larynx |
16 |
4 |
|||
|
Ikeda et al[72] |
Talaporfin sodium |
8 (PDT being the primary treatment) |
Oral SCC without metastasis (T2–T4) |
6 |
2 |
Mean overall survival: 40.2 mo |
||
|
Ikeda et al[73] |
Photofrin |
25 (PDT being the primary treatment in 20 cases and secondary treatment in 5 cases) |
Oral SCC (18 cases), dysplasia (7) |
24 |
1 |
Disease-specific survival rate: 95.8% |
||
|
Kübler et al[74] |
mTHPC |
25 (PDT being the primary treatment) |
SCC of the lip (Tis, T1, T2/N0/M0) |
24 |
1 |
Mean follow-up: 428 d |
||
|
Toratani et al[75] |
Photofrin |
34 |
Oral SCC or Cis |
30 |
3 |
1 |
5-y overall survival: 76.5% |
|
|
Biel[76] |
Photofrin |
276 |
Recurrent or primary Cis,g T1N0, and T2N0 laryngeal and oral cancers |
Cure rate: laryngeal (91%), oral (94%) |
||||
|
Jerjes et al[77] |
mTHPC |
110 |
Stage IV or high grade |
32 |
68 |
6 |
4 |
|
|
Hosokawa et al[78] |
Photofrin |
42 |
Head and neck squamous cell carcinoma (T1: 28; T2: 13; T3: 1) |
29 |
12 |
0 |
1 |
5-y overall survival: 57.8% |
|
Hopper et al[79] |
mTHPC |
114 (protocol compliant) |
Primary squamous cell carcinoma of the lip, oral cavity, oropharynx, or hypopharynx, Tis, (T1 or T2, N0, M0) |
97 |
13 |
2 |
2-y survival: 75% |
|
|
D'Cruz et al[15] |
mTHPC |
128 |
Recurrent/refractory HNSCC not amenable to conventional treatment |
30% |
24% |
Median survival for cases with CR: 245 d |
||
|
Tan et al[80] |
mTHPC |
39 |
Recurrent/refractory HNSCC not amenable to conventional treatment (with 3.9-mo median survival[81]) |
19 |
2 |
5 |
5 |
Median overall survival: 37 mo |
Note: WHO response criteria define treatment outcomes as follows: Complete response (CR)—complete disappearance of disease; partial response (PR)—≥50% reduction in tumor size; no response (NR) or stable disease (SD)— < 50% decrease or <25% increase; progressive disease (PD)—≥25% increase or new lesions. Responses must be confirmed at least 4 weeks apart.
Effective as an Adjuvant to Conventional Therapies
PDT can be integrated with surgery, chemotherapy, or radiotherapy to reduce residual tumor burden or enhance overall treatment efficacy.[46] It has been shown to improve disease-free survival in patients with positive surgical margins following resection,[47] and has demonstrated efficacy in managing recurrent squamous cell carcinoma (SCC) of the base of the tongue.[48] In a separate report, redaporfin-mediated PDT successfully ablated all visible lesions in a patient with extensive, treatment-resistant oral cavity tumors. The patient, who had previously undergone surgery, radiotherapy, and multiple systemic therapies, achieved a sustained complete response following subsequent treatment with an immune checkpoint inhibitor.[49] Additionally, Wang et al[50] reported a 90.9% overall response rate when 11 patients with locally advanced oral SCC were treated using a combination of topical 5-aminolevulinic acid (5-ALA) PDT and platinum-based induction chemotherapy.
Recent Development and Prospects of PDT
Although PDT has been demonstrated to be effective in the treatment of HNC, it has also been helpful in the treatment of other medical conditions. Recent developments in PDT have focused on expanding global access by positioning PDT as a safe and relatively low-cost cancer treatment, enhancing tumour selectivity through nanoparticle-based delivery systems, and advancing the translational application of related approaches such as photoimmunotherapy (PIT) and photochemical internalization (PCI).
Advocacy for Global Access of Cancer Patients to PDT
At the 17th International Photodynamic Association World Congress, 2019, held at Cambridge, MA, in addition to advocating for developing worldwide application of PDT for HNC, the congress also made a case to ensure global access to PDT and to open a PDT registry. As PDT is cheap, portable, and effective in treating HNC, assisting developing countries in setting it up will prevent delays associated with waiting for surgery or radiotherapy.[51] A delay in initiating treatment for HNC may significantly worsen outcomes, as even a 1-month postponement may allow the tumor volume to double. The Lancet Commission on Global Surgery (LCoGS) suggests that by 2030, 20 surgeons, anesthetists, and obstetricians should provide care for 100,000 individuals in all countries. In a study to estimate the density of the otorhinolaryngology and head and neck surgery (OHNS) workforce in 114 countries and territories, Petrucci et al[52] reported an average OHNS clinician density of 2.19 per 100,000 population (range: 0–61.7). Europe had the highest density at 5.70 per 100,000 people, while Africa and Southeast Asia had the lowest at 0.18 and 1.12 per 100,000 people, respectively. In addition, the World Health Organization (WHO) has suggested four linear accelerators to serve a million people. This standard is beyond the reach of individuals living in low- and middle-income countries (LMICs). Ensuring the global availability of inexpensive PDT and its adoption as a treatment modality for HNC will reduce the burden of disease associated with HNC.[51] [53] [54] [55] [56] [57] [58] [59]
PDT Associated with Nanoparticles
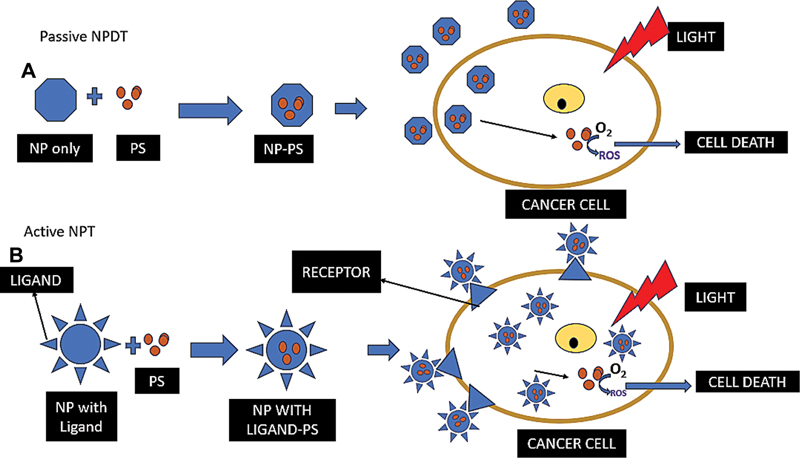
Nanoparticles (hereinafter NPs) are nano-sized carriers capable of delivering targeted therapy to cancer cells, thereby minimizing toxicity to normal tissues. By encapsulating these agents, nanocarriers allow for higher drug concentrations in tumors while reducing side effects in the body. They provide protection against degradation, prolong drug circulation in the bloodstream, increase drug payload, enable controlled release kinetics, and enhance the solubility of insoluble drugs.[11] Based on the materials NPs are prepared from, they are categorized as metallic NPs, polymeric NPs, solid lipid NPs, and nanostructured lipid nanocarriers.[60] [61] NPs demonstrate enhanced permeability and retention due to the abnormal neo-vasculature of the tumor microenvironment, causing substances to accumulate in the tumor cells. NP activity is either active or passive (see [Fig. 2]). It is active if coated with ligands that bind to a specific overexpressed molecule on the tumor surface, hence targeted in action. It is, however, passive if it lacks such ligands.[60] [62] Wang et al[63] reported that active NP-based PDT enhances better treatment efficacy while reducing the PS dose than its passive form.
Photochemical Internalization and Photoimmunotherapy
PCI is an advanced drug-delivery technique that enhances intracellular transport of therapeutic agents through the combined use of a PS and light activation (see [Fig. 3]). When the PS and drug are co-localized within endosomes, subsequent illumination induces a photochemical reaction that disrupts the endosomal membrane, releasing the therapeutic payload into the cytosol. This mechanism has demonstrated strong potential for overcoming intracellular barriers and improving the efficacy of treatments such as chemotherapy and gene delivery, making PCI a promising platform for precise and targeted therapeutic strategies.[64] Preclinical models further indicate that PCI can selectively destroy tumor cells while sparing neuronal viability, suggesting a favorable safety margin for treating cancers located near nervous tissue.[65] Clinical findings align with this safety profile as the first-in-human Phase I trial of TPCS2a-mediated PCI reported that the treatment was generally well tolerated in patients with advanced or recurrent solid malignancies, with adverse events largely limited to local inflammation and expected photosensitivity. Dose-limiting toxicities were observed only at higher PS concentrations, with a maximum tolerated dose of 1.0 mg/kg established, underscoring PCI's feasibility and safety for further clinical development.[66]

PIT is a therapeutic modality that combines the principles of phototherapy and immunotherapy to achieve targeted and precise cancer treatment. This emerging approach involves the use of PSs conjugated to monoclonal antibodies specific to cancer cells or tumor-associated antigens. Upon administration, these photoimmunoconjugates selectively bind to cancerous cells. Subsequent exposure to light of a specific wavelength activates PS, inducing a localized phototoxic effect that selectively eradicates the targeted cancer cells. Notably, the combination of immunological recognition and photochemical cytotoxicity in PIT provides a dual mechanism for cancer cell destruction, potentially enhancing treatment specificity and minimizing collateral damage to healthy tissues. This modality is a promising treatment option for HNSCC and recurrent diseases. Nguyen et al, in an in vitro study, reported that cetuximab-based PS conjugates (Cet-IRDye800CW) were able to induce 90% phototoxicity on FaDu HNC cells.[67] Early-phase clinical trials of PIT in recurrent or metastatic HNSCC—particularly in patients heavily pretreated or no longer amenable to conventional therapy—have demonstrated encouraging safety and efficacy signals. Phase I/II studies of RM-1929[68]and ASP-1929[69] showed that PIT was generally well tolerated, with mostly mild to moderate toxicities and manageable treatment-related adverse events. Objective response rates ranged from 26 to 43%, with several complete responses reported, even in populations with historically poor outcomes and limited therapeutic options. Median overall survival reached 9.3 months with RM-1929 monotherapy and extended to 25.6 months when combined with pembrolizumab in programmed death ligand 1(PD-L1) positive disease. These results highlight the potential of PIT to achieve meaningful tumor control where standard salvage approaches have low success rates.
Conclusion
In summary, PDT is a promising and beneficial treatment modality for HNC. Its inherent qualities, such as targeted specificity, quick administration as an outpatient procedure, cost-effectiveness, noninvasiveness, and repeatability, make PDT a compelling therapeutic option. Notably, the ability of PDT to preserve patients' QoL sets it apart from other HNC treatments. In addition to these immediate benefits, PDT's prospects include addressing issues such as deeply seated tumors, with ongoing advancements in light delivery technologies, and the use of NPs for improved targeted therapy. These combined advantages and evolving prospects highlight the potential of PDT as a treatment for HNCs.
Conflict of Interest
None declared.
Acknowledgments
The authors acknowledge the Malaysian MOHE for funding their research.
Authors' Contributions
N.M.L. had the original idea for the article and developed the review concept. A.M.B. performed the literature search and drafted the initial manuscript. Z.I.M.I., S.E.T.S., T.A.D.A.A.T.D., N.M., S.A., C.F., and N.M.L. critically revised the work for important intellectual content. All the authors read and approved the final version of the manuscript.
Compliance with Ethical Principles
Not applicable.
-
References
- 1 Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2024; 74 (03) 229-263
- 2 Kang H(T), Kennedy TA, Yu E. Head and neck squamous cell cancer: approach to staging and surveillance. In: Hodler J, Kubik-Huch RA, Roos JE. eds. Diseases of the Brain, Head and Neck, Spine 2024–2027: Diagnostic Imaging. Cham: Springer; 2024: 251-264
- 3 Johnson DE, Burtness B, Leemans CR, Lui VWY, Bauman JE, Grandis JR. Head and neck squamous cell carcinoma. Nat Rev Dis Primers 2020; 6 (01) 92
- 4 Pfister DG, Spencer S, Adelstein D. et al. Head and neck cancers, version 2.2020. J Natl Compr Canc Netw 2020; 18 (07) 873-898
- 5 Peng W, de Bruijn HS, Ten Hagen TLM. et al. Targeted photodynamic therapy of human head and neck squamous cell carcinoma with anti-epidermal growth factor receptor antibody cetuximab and photosensitizer IR700DX in the mouse skin-fold window chamber model. Photochem Photobiol 2020; 96 (03) 708-717
- 6 Rigual NR, Thankappan K, Cooper M. et al. Photodynamic therapy for head and neck dysplasia and cancer. Arch Otolaryngol Head Neck Surg 2009; 135 (08) 784-788
- 7 Kwiatkowski S, Knap B, Przystupski D. et al. Photodynamic therapy: mechanisms, photosensitizers and combinations. Biomed Pharmacother 2018; 106: 1098-1107
- 8 Agostinis P, Berg K, Cengel KA. et al. Photodynamic therapy of cancer: an update. CA Cancer J Clin 2011; 61 (04) 250-281
- 9 Zuluaga MF, Lange N. Combination of photodynamic therapy with anti-cancer agents. Curr Med Chem 2008; 15 (17) 1655-1673
- 10 O'Connor AE, Gallagher WM, Byrne AT. Porphyrin and nonporphyrin photosensitizers in oncology: preclinical and clinical advances in photodynamic therapy. Photochem Photobiol 2009; 85 (05) 1053-1074
- 11 Dave D, Desai U, Despande N. Photodynamic therapy: a view through light. J Orofac Res 2012; 2: 82-86
- 12 Allison RR, Huang Z, Dallimore I, Moghissi K. Tools of clinical photodynamic therapy (PDT): a mini compendium. Photodiagnosis Photodyn Ther 2024; 46: 104058
- 13 Kim MM, Darafsheh A. Light sources and dosimetry techniques for photodynamic therapy. Photochem Photobiol 2020; 96 (02) 280-294
- 14 Gunaydin G, Gedik ME, Ayan S. Photodynamic therapy for the treatment and diagnosis of cancer: a review of the current clinical status. Front Chem 2021; 9: 686303
- 15 D'Cruz AK, Robinson MH, Biel MA. mTHPC-mediated photodynamic therapy in patients with advanced, incurable head and neck cancer: a multicenter study of 128 patients. Head Neck 2004; 26 (03) 232-240
- 16 Vidujith AVA, Jayasinghe CD, De Costa MDP, Senthilnithy R. Photodynamic therapy: an overview and insights into a prospective mainstream anticancer therapy. J Turkish Chem Soc Sect Chem 2022; 9 (03) 821-848
- 17 Sarafoleanu C, Vuzitas A, Manea C. Difficulties in the surgical management of head and neck cancer patient. Rom J Rhinol 2017; 7 (27) 153-161
- 18 Embring A, Onjukka E, Mercke C, Lax I, Berglund A, Friesland S. Dose escalation of oropharyngeal cancer: long-time follow-up and side effects. Cancers (Basel) 2023; 15 (09) 2580
- 19 Stubblefield MD. Clinical evaluation and management of radiation fibrosis syndrome. Phys Med Rehabil Clin N Am 2017; 28 (01) 89-100
- 20 Lou PJ, Jäger HR, Jones L, Theodossy T, Bown SG, Hopper C. Interstitial photodynamic therapy as salvage treatment for recurrent head and neck cancer. Br J Cancer 2004; 91 (03) 441-446
- 21 Harréus U. Surgical errors and risks: the head and neck cancer patient. GMS Curr Top Otorhinolaryngol Head Neck Surg 2013; 12: Doc04
- 22 Stoker SD, Indrasari SR, Herdini C. et al. Photodynamic therapy as salvage therapy for patients with nasopharyngeal carcinoma experiencing local failures following definitive radiotherapy. Photodiagnosis Photodyn Ther 2015; 12 (03) 519-525
- 23 Singh MN, Kinhikar RA, Agarwal JP, Laskar SG. Principles and practice of radiation oncology. In: Kataki AC, Barmon D. eds. Fundamentals in Gynaecologic Malignancy. Singapore: Springer; 2022: 99-117
- 24 Melissant HC, Jansen F, Eerenstein SE. et al. Body image distress in head and neck cancer patients: what are we looking at?. Support Care Cancer 2021; 29 (04) 2161-2169
- 25 Ronen O, Robbins KT, Shaha AR. et al. Emerging concepts impacting head and neck cancer surgery morbidity. Oncol Ther 2023; 11 (01) 1-13
- 26 Brook I. Early side effects of radiation treatment for head and neck cancer. Cancer Radiother 2021; 25 (05) 507-513
- 27 Brook I. Late side effects of radiation treatment for head and neck cancer. Radiat Oncol J 2020; 38 (02) 84-92
- 28 Wright KE, Liniker E, Loizidou M, Moore C, Macrobert AJ, Phillips JB. Peripheral neural cell sensitivity to mTHPC-mediated photodynamic therapy in a 3D in vitro model. Br J Cancer 2009; 101 (04) 658-665
- 29 Kübler AC, Stenzel W, Rühling M, Meul B, Fischer JH. Experimental evaluation of possible side effects of intra-operative photodynamic therapy on rabbit blood vessels and nerves. Lasers Surg Med 2003; 33 (04) 247-255
- 30 Grant WE, Speight PM, MacRobert AJ, Hopper C, Bown SG. Photodynamic therapy of normal rat arteries after photosensitisation using disulphonated aluminium phthalocyanine and 5-aminolaevulinic acid. Br J Cancer 1994; 70 (01) 72-78
- 31 Lou PJ, Jäger HR, Jones L, Theodossy T, Bown SG, Hopper C. Interstitial photodynamic therapy as salvage treatment for recurrent head and neck cancer. Br J Cancer 2004; 91 (03) 441-446
- 32 Rigual NR, Thankappan K, Cooper M. et al. Photodynamic therapy for head and neck dysplasia and cancer. Arch Otolaryngol Head Neck Surg 2009; 135 (08) 784-788
- 33 Rigual NR, Shafirstein G, Frustino J. et al. Adjuvant intraoperative photodynamic therapy in head and neck cancer. JAMA Otolaryngol Head Neck Surg 2013; 139 (07) 706-711
- 34 The World Health Organization quality of life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med 1995; 41 (10) 1403-1409
- 35 Tonsbeek AM, Hundepool CA, Roubos J. et al. Quality of life in 583 head and neck cancer survivors assessed with the FACE-Q head and neck cancer module. Oral Oncol 2024; 153: 106813
- 36 Jerjes W, Stevenson H, Ramsay D, Hamdoon Z, Hopper C. Quality of life following photodynamic therapy for head and neck pathologies: an exploratory study. Photodiagnosis Photodyn Ther 2022; 38: 102800
- 37 Hung TM, Lin CR, Chi YC. et al. Body image in head and neck cancer patients treated with radiotherapy: the impact of surgical procedures. Health Qual Life Outcomes 2017; 15 (01) 165
- 38 Karakullukcu B, van Oudenaarde K, Copper MP. et al. Photodynamic therapy of early stage oral cavity and oropharynx neoplasms: an outcome analysis of 170 patients. Eur Arch Otorhinolaryngol 2011; 268 (02) 281-288
- 39 Abbas S, Jerjes W, Upile T, Vaz F, Hopper C. The palliative role of PDT in recurrent advanced nasopharyngeal carcinoma: case series. Photodiagnosis Photodyn Ther 2012; 9 (02) 142-147
- 40 Kübler A, Niziol C, Sidhu M, Dünne A, Werner JA. Analysis of cost effectiveness of photodynamic therapy with Foscan (Foscan-PDT) in comparison with palliative chemotherapy in patients with advanced head-neck tumors in Germany. Laryngorhinootologie 2005; 84 (10) 725-732
- 41 Hopper C, Niziol C, Sidhu M. The cost-effectiveness of Foscan mediated photodynamic therapy (Foscan-PDT) compared with extensive palliative surgery and palliative chemotherapy for patients with advanced head and neck cancer in the UK. Oral Oncol 2004; 40 (04) 372-382
- 42 Kato H, Okunaka T, Tsuchida T, Shibuya H, Fujino S, Ogawa K. Analysis of the cost-effectiveness of photodynamic therapy in early stage lung cancer. Diagn Ther Endosc 1999; 6 (01) 9-16
- 43 Cerrati EW, Nguyen SA, Farrar JD, Lentsch EJ. The efficacy of photodynamic therapy in the treatment of oral squamous cell carcinoma: a meta-analysis. Ear Nose Throat J 2015; 94 (02) 72-79
- 44 Gondivkar SM, Gadbail AR, Choudhary MG, Vedpathak PR, Likhitkar MS. Photodynamic treatment outcomes of potentially-malignant lesions and malignancies of the head and neck region: a systematic review. J Investig Clin Dent 2018; 9 (01) e12270
- 45 Liu W, Zhang X, Shen X, Liu L. Evaluating photodynamic therapy for oral precancerous lesions: highlighting outcome measure of malignant transformation. J Dent Sci 2024; 19 (01) 631-636
- 46 Jiang W, Liang M, Lei Q, Li G, Wu S. The current status of photodynamic therapy in cancer treatment. Cancers (Basel) 2023; 15 (03) 585
- 47 van Doeveren TEM, Karakullukçu MB, van Veen RLP, Lopez-Yurda M, Schreuder WH, Tan IB. Adjuvant photodynamic therapy in head and neck cancer after tumor-positive resection margins. Laryngoscope 2018; 128 (03) 657-663
- 48 Vander Poorten V, Meulemans J, Nuyts S. et al. Postoperative photodynamic therapy as a new adjuvant treatment after robot-assisted salvage surgery of recurrent squamous cell carcinoma of the base of tongue. World J Surg Oncol 2015; 13 (01) 214
- 49 Santos LL, Oliveira J, Monteiro E, Santos J, Sarmento C. Treatment of head and neck cancer with photodynamic therapy with redaporfin: a clinical case report. Case Rep Oncol 2018; 11 (03) 769-776
- 50 Wang X, Li N, Meng J, Wen N. The use of topical ALA-photodynamic therapy combined with induction chemotherapy for locally advanced oral squamous cell carcinoma. Am J Otolaryngol 2021; 42 (06) 103112
- 51 Hopper C, Tan B, Hasan T. et al. Developing world applications of PDT in head and neck cancer (conference presentation). In: Hasan T. ed. 17th International Photodynamic Association World Congress. Vol. 11070. Bellingham, WA: SPIE; 2019. :110703U
- 52 Petrucci B, Okerosi S, Patterson RH. et al. The global otolaryngology-head and neck surgery workforce. JAMA Otolaryngol Head Neck Surg 2023; 149 (10) 904-911
- 53 Patterson RH, Fischman VG, Wasserman I. et al. Global burden of head and neck cancer: economic consequences, health, and the role of surgery. Otolaryngol Head Neck Surg 2020; 162 (03) 296-303
- 54 Gollnick S, Anton K. Development of a registry for patients treated with photodynamic therapy (conference presentation). In: Kessel DH, Hasan T. eds. Optical Methods for Tumor Treatment and Detection: Mechanisms and Techniques in Photodynamic Therapy XXVII. Vol. 10476. Bellingham, WA: SPIE; 2018: 104760M
- 55 Souho T, Lamboni L, Xiao L, Yang G. Cancer hallmarks and malignancy features: gateway for improved targeted drug delivery. Biotechnol Adv 2018; 36 (07) 1928-1945
- 56 Pérez-Herrero E, Fernández-Medarde A. Advanced targeted therapies in cancer: drug nanocarriers, the future of chemotherapy. Eur J Pharm Biopharm 2015; 93: 52-79
- 57 Dai X, Yu L, Zhao X, Ostrikov KK. Nanomaterials for oncotherapies targeting the hallmarks of cancer. Nanotechnology 2020; 31 (39) 392001
- 58 Lee D, Kwon S, Jang SY, Park E, Lee Y, Koo H. Overcoming the obstacles of current photodynamic therapy in tumors using nanoparticles. Bioact Mater 2021; 8: 20-34
- 59 Huang L, Asghar S, Zhu T. et al. Advances in chlorin-based photodynamic therapy with nanoparticle delivery system for cancer treatment. Expert Opin Drug Deliv 2021; 18 (10) 1473-1500
- 60 Hong EJ, Choi DG, Shim MS. Targeted and effective photodynamic therapy for cancer using functionalized nanomaterials. Acta Pharm Sin B 2016; 6 (04) 297-307
- 61 Itoo AM, Paul M, Padaga SG, Ghosh B, Biswas S. Nanotherapeutic intervention in photodynamic therapy for cancer. ACS Omega 2022; 7 (50) 45882-45909
- 62 dos Santos AF, Arini GS, de Almeida DRQ, Labriola L. Nanophotosensitizers for cancer therapy: a promising technology?. JPhys Mater 2021; 4 (03) 034013
- 63 Wang D, Fei B, Halig LV. et al. Targeted iron-oxide nanoparticle for photodynamic therapy and imaging of head and neck cancer. ACS Nano 2014; 8 (07) 6620-6632
- 64 Jerjes W, Theodossiou TA, Hirschberg H. et al; From Basic Mechanisms to Clinical Research. Photochemical internalization for intracellular drug delivery: from basic mechanisms to clinical research. J Clin Med 2020; 9 (02) 528
- 65 O'Rourke C, Hopper C, MacRobert AJ, Phillips JB, Woodhams JH. Could clinical photochemical internalisation be optimised to avoid neuronal toxicity?. Int J Pharm 2017; 528 (1–2): 133-143
- 66 Sultan AA, Jerjes W, Berg K. et al. Disulfonated tetraphenyl chlorin (TPCS2a)-induced photochemical internalisation of bleomycin in patients with solid malignancies: a phase 1, dose-escalation, first-in-man trial. Lancet Oncol 2016; 17 (09) 1217-1229
- 67 Nguyen A, Bhandari C, Keown M. et al. Increasing the dye payload of cetuximab-IRDye800CW enables photodynamic therapy. Mol Pharm 2024; 21 (07) 3296-3309
- 68 Cognetti DM, Johnson JM, Curry JM. et al. Phase 1/2a, open-label, multicenter study of RM-1929 photoimmunotherapy in patients with locoregional, recurrent head and neck squamous cell carcinoma. Head Neck 2021; 43 (12) 3875-3887
- 69 Cognetti DM, Curry JM, Johnson J. et al. Safety and efficacy findings from a phase Ib/II study of ASP-1929 photoimmunotherapy with pembrolizumab in recurrent and/or metastatic head and neck squamous cell carcinoma. Head Neck 2025; 47 (01) 1-15
- 70 Lorenz KJ, Maier H. Photodynamic therapy with meta-tetrahydroxyphenylchlorin (Foscan) in the management of squamous cell carcinoma of the head and neck: experience with 35 patients. Eur Arch Otorhinolaryngol 2009; 266 (12) 1937-1944
- 71 Schweitzer VG. PHOTOFRIN-mediated photodynamic therapy for treatment of early stage oral cavity and laryngeal malignancies. Lasers Surg Med 2001; 29 (04) 305-313
- 72 Ikeda H, Ohba S, Egashira K, Asahina I. The effect of photodynamic therapy with talaporfin sodium, a second-generation photosensitizer, on oral squamous cell carcinoma: a series of eight cases. Photodiagnosis Photodyn Ther 2018; 21: 176-180
- 73 Ikeda H, Tobita T, Ohba S, Uehara M, Asahina I. Treatment outcome of Photofrin-based photodynamic therapy for T1 and T2 oral squamous cell carcinoma and dysplasia. Photodiagnosis Photodyn Ther 2013; 10 (03) 229-235
- 74 Kübler AC, de Carpentier J, Hopper C, Leonard AG, Putnam G. Treatment of squamous cell carcinoma of the lip using Foscan-mediated photodynamic therapy. Int J Oral Maxillofac Surg 2001; 30 (06) 504-509
- 75 Toratani S, Tani R, Kanda T, Koizumi K, Yoshioka Y, Okamoto T. Photodynamic therapy using Photofrin and excimer dye laser treatment for superficial oral squamous cell carcinomas with long-term follow up. Photodiagnosis Photodyn Ther 2016; 14: 104-110
- 76 Biel MA. Photodynamic therapy treatment of early oral and laryngeal cancers. Photochem Photobiol 2007; 83 (05) 1063-1068
- 77 Jerjes W, Upile T, Alexander Mosse C. et al. Prospective evaluation of 110 patients following ultrasound-guided photodynamic therapy for deep seated pathologies. Photodiagnosis Photodyn Ther 2011; 8 (04) 297-306
- 78 Hosokawa S, Takahashi G, Sugiyama KI. et al. Porfimer sodium-mediated photodynamic therapy in patients with head and neck squamous cell carcinoma. Photodiagnosis Photodyn Ther 2020; 29: 101627
- 79 Hopper C, Kübler A, Lewis H, Tan IB, Putnam G. mTHPC-mediated photodynamic therapy for early oral squamous cell carcinoma. Int J Cancer 2004; 111 (01) 138-146
- 80 Tan IB, Dolivet G, Ceruse P, Vander Poorten V, Roest G, Rauschning W. Temoporfin-mediated photodynamic therapy in patients with advanced, incurable head and neck cancer: a multicenter study. Head Neck 2010; 32 (12) 1597-1604
- 81 Carvalho AL, Salvajoli JV, Kowalski LP. A comparison of radiotherapy or radiochemotherapy with symptomatic treatment alone in patients with advanced head and neck carcinomas. Eur Arch Otorhinolaryngol 2000; 257 (03) 164-167
Address for correspondence
Publication History
Article published online:
31 December 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2024; 74 (03) 229-263
- 2 Kang H(T), Kennedy TA, Yu E. Head and neck squamous cell cancer: approach to staging and surveillance. In: Hodler J, Kubik-Huch RA, Roos JE. eds. Diseases of the Brain, Head and Neck, Spine 2024–2027: Diagnostic Imaging. Cham: Springer; 2024: 251-264
- 3 Johnson DE, Burtness B, Leemans CR, Lui VWY, Bauman JE, Grandis JR. Head and neck squamous cell carcinoma. Nat Rev Dis Primers 2020; 6 (01) 92
- 4 Pfister DG, Spencer S, Adelstein D. et al. Head and neck cancers, version 2.2020. J Natl Compr Canc Netw 2020; 18 (07) 873-898
- 5 Peng W, de Bruijn HS, Ten Hagen TLM. et al. Targeted photodynamic therapy of human head and neck squamous cell carcinoma with anti-epidermal growth factor receptor antibody cetuximab and photosensitizer IR700DX in the mouse skin-fold window chamber model. Photochem Photobiol 2020; 96 (03) 708-717
- 6 Rigual NR, Thankappan K, Cooper M. et al. Photodynamic therapy for head and neck dysplasia and cancer. Arch Otolaryngol Head Neck Surg 2009; 135 (08) 784-788
- 7 Kwiatkowski S, Knap B, Przystupski D. et al. Photodynamic therapy: mechanisms, photosensitizers and combinations. Biomed Pharmacother 2018; 106: 1098-1107
- 8 Agostinis P, Berg K, Cengel KA. et al. Photodynamic therapy of cancer: an update. CA Cancer J Clin 2011; 61 (04) 250-281
- 9 Zuluaga MF, Lange N. Combination of photodynamic therapy with anti-cancer agents. Curr Med Chem 2008; 15 (17) 1655-1673
- 10 O'Connor AE, Gallagher WM, Byrne AT. Porphyrin and nonporphyrin photosensitizers in oncology: preclinical and clinical advances in photodynamic therapy. Photochem Photobiol 2009; 85 (05) 1053-1074
- 11 Dave D, Desai U, Despande N. Photodynamic therapy: a view through light. J Orofac Res 2012; 2: 82-86
- 12 Allison RR, Huang Z, Dallimore I, Moghissi K. Tools of clinical photodynamic therapy (PDT): a mini compendium. Photodiagnosis Photodyn Ther 2024; 46: 104058
- 13 Kim MM, Darafsheh A. Light sources and dosimetry techniques for photodynamic therapy. Photochem Photobiol 2020; 96 (02) 280-294
- 14 Gunaydin G, Gedik ME, Ayan S. Photodynamic therapy for the treatment and diagnosis of cancer: a review of the current clinical status. Front Chem 2021; 9: 686303
- 15 D'Cruz AK, Robinson MH, Biel MA. mTHPC-mediated photodynamic therapy in patients with advanced, incurable head and neck cancer: a multicenter study of 128 patients. Head Neck 2004; 26 (03) 232-240
- 16 Vidujith AVA, Jayasinghe CD, De Costa MDP, Senthilnithy R. Photodynamic therapy: an overview and insights into a prospective mainstream anticancer therapy. J Turkish Chem Soc Sect Chem 2022; 9 (03) 821-848
- 17 Sarafoleanu C, Vuzitas A, Manea C. Difficulties in the surgical management of head and neck cancer patient. Rom J Rhinol 2017; 7 (27) 153-161
- 18 Embring A, Onjukka E, Mercke C, Lax I, Berglund A, Friesland S. Dose escalation of oropharyngeal cancer: long-time follow-up and side effects. Cancers (Basel) 2023; 15 (09) 2580
- 19 Stubblefield MD. Clinical evaluation and management of radiation fibrosis syndrome. Phys Med Rehabil Clin N Am 2017; 28 (01) 89-100
- 20 Lou PJ, Jäger HR, Jones L, Theodossy T, Bown SG, Hopper C. Interstitial photodynamic therapy as salvage treatment for recurrent head and neck cancer. Br J Cancer 2004; 91 (03) 441-446
- 21 Harréus U. Surgical errors and risks: the head and neck cancer patient. GMS Curr Top Otorhinolaryngol Head Neck Surg 2013; 12: Doc04
- 22 Stoker SD, Indrasari SR, Herdini C. et al. Photodynamic therapy as salvage therapy for patients with nasopharyngeal carcinoma experiencing local failures following definitive radiotherapy. Photodiagnosis Photodyn Ther 2015; 12 (03) 519-525
- 23 Singh MN, Kinhikar RA, Agarwal JP, Laskar SG. Principles and practice of radiation oncology. In: Kataki AC, Barmon D. eds. Fundamentals in Gynaecologic Malignancy. Singapore: Springer; 2022: 99-117
- 24 Melissant HC, Jansen F, Eerenstein SE. et al. Body image distress in head and neck cancer patients: what are we looking at?. Support Care Cancer 2021; 29 (04) 2161-2169
- 25 Ronen O, Robbins KT, Shaha AR. et al. Emerging concepts impacting head and neck cancer surgery morbidity. Oncol Ther 2023; 11 (01) 1-13
- 26 Brook I. Early side effects of radiation treatment for head and neck cancer. Cancer Radiother 2021; 25 (05) 507-513
- 27 Brook I. Late side effects of radiation treatment for head and neck cancer. Radiat Oncol J 2020; 38 (02) 84-92
- 28 Wright KE, Liniker E, Loizidou M, Moore C, Macrobert AJ, Phillips JB. Peripheral neural cell sensitivity to mTHPC-mediated photodynamic therapy in a 3D in vitro model. Br J Cancer 2009; 101 (04) 658-665
- 29 Kübler AC, Stenzel W, Rühling M, Meul B, Fischer JH. Experimental evaluation of possible side effects of intra-operative photodynamic therapy on rabbit blood vessels and nerves. Lasers Surg Med 2003; 33 (04) 247-255
- 30 Grant WE, Speight PM, MacRobert AJ, Hopper C, Bown SG. Photodynamic therapy of normal rat arteries after photosensitisation using disulphonated aluminium phthalocyanine and 5-aminolaevulinic acid. Br J Cancer 1994; 70 (01) 72-78
- 31 Lou PJ, Jäger HR, Jones L, Theodossy T, Bown SG, Hopper C. Interstitial photodynamic therapy as salvage treatment for recurrent head and neck cancer. Br J Cancer 2004; 91 (03) 441-446
- 32 Rigual NR, Thankappan K, Cooper M. et al. Photodynamic therapy for head and neck dysplasia and cancer. Arch Otolaryngol Head Neck Surg 2009; 135 (08) 784-788
- 33 Rigual NR, Shafirstein G, Frustino J. et al. Adjuvant intraoperative photodynamic therapy in head and neck cancer. JAMA Otolaryngol Head Neck Surg 2013; 139 (07) 706-711
- 34 The World Health Organization quality of life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med 1995; 41 (10) 1403-1409
- 35 Tonsbeek AM, Hundepool CA, Roubos J. et al. Quality of life in 583 head and neck cancer survivors assessed with the FACE-Q head and neck cancer module. Oral Oncol 2024; 153: 106813
- 36 Jerjes W, Stevenson H, Ramsay D, Hamdoon Z, Hopper C. Quality of life following photodynamic therapy for head and neck pathologies: an exploratory study. Photodiagnosis Photodyn Ther 2022; 38: 102800
- 37 Hung TM, Lin CR, Chi YC. et al. Body image in head and neck cancer patients treated with radiotherapy: the impact of surgical procedures. Health Qual Life Outcomes 2017; 15 (01) 165
- 38 Karakullukcu B, van Oudenaarde K, Copper MP. et al. Photodynamic therapy of early stage oral cavity and oropharynx neoplasms: an outcome analysis of 170 patients. Eur Arch Otorhinolaryngol 2011; 268 (02) 281-288
- 39 Abbas S, Jerjes W, Upile T, Vaz F, Hopper C. The palliative role of PDT in recurrent advanced nasopharyngeal carcinoma: case series. Photodiagnosis Photodyn Ther 2012; 9 (02) 142-147
- 40 Kübler A, Niziol C, Sidhu M, Dünne A, Werner JA. Analysis of cost effectiveness of photodynamic therapy with Foscan (Foscan-PDT) in comparison with palliative chemotherapy in patients with advanced head-neck tumors in Germany. Laryngorhinootologie 2005; 84 (10) 725-732
- 41 Hopper C, Niziol C, Sidhu M. The cost-effectiveness of Foscan mediated photodynamic therapy (Foscan-PDT) compared with extensive palliative surgery and palliative chemotherapy for patients with advanced head and neck cancer in the UK. Oral Oncol 2004; 40 (04) 372-382
- 42 Kato H, Okunaka T, Tsuchida T, Shibuya H, Fujino S, Ogawa K. Analysis of the cost-effectiveness of photodynamic therapy in early stage lung cancer. Diagn Ther Endosc 1999; 6 (01) 9-16
- 43 Cerrati EW, Nguyen SA, Farrar JD, Lentsch EJ. The efficacy of photodynamic therapy in the treatment of oral squamous cell carcinoma: a meta-analysis. Ear Nose Throat J 2015; 94 (02) 72-79
- 44 Gondivkar SM, Gadbail AR, Choudhary MG, Vedpathak PR, Likhitkar MS. Photodynamic treatment outcomes of potentially-malignant lesions and malignancies of the head and neck region: a systematic review. J Investig Clin Dent 2018; 9 (01) e12270
- 45 Liu W, Zhang X, Shen X, Liu L. Evaluating photodynamic therapy for oral precancerous lesions: highlighting outcome measure of malignant transformation. J Dent Sci 2024; 19 (01) 631-636
- 46 Jiang W, Liang M, Lei Q, Li G, Wu S. The current status of photodynamic therapy in cancer treatment. Cancers (Basel) 2023; 15 (03) 585
- 47 van Doeveren TEM, Karakullukçu MB, van Veen RLP, Lopez-Yurda M, Schreuder WH, Tan IB. Adjuvant photodynamic therapy in head and neck cancer after tumor-positive resection margins. Laryngoscope 2018; 128 (03) 657-663
- 48 Vander Poorten V, Meulemans J, Nuyts S. et al. Postoperative photodynamic therapy as a new adjuvant treatment after robot-assisted salvage surgery of recurrent squamous cell carcinoma of the base of tongue. World J Surg Oncol 2015; 13 (01) 214
- 49 Santos LL, Oliveira J, Monteiro E, Santos J, Sarmento C. Treatment of head and neck cancer with photodynamic therapy with redaporfin: a clinical case report. Case Rep Oncol 2018; 11 (03) 769-776
- 50 Wang X, Li N, Meng J, Wen N. The use of topical ALA-photodynamic therapy combined with induction chemotherapy for locally advanced oral squamous cell carcinoma. Am J Otolaryngol 2021; 42 (06) 103112
- 51 Hopper C, Tan B, Hasan T. et al. Developing world applications of PDT in head and neck cancer (conference presentation). In: Hasan T. ed. 17th International Photodynamic Association World Congress. Vol. 11070. Bellingham, WA: SPIE; 2019. :110703U
- 52 Petrucci B, Okerosi S, Patterson RH. et al. The global otolaryngology-head and neck surgery workforce. JAMA Otolaryngol Head Neck Surg 2023; 149 (10) 904-911
- 53 Patterson RH, Fischman VG, Wasserman I. et al. Global burden of head and neck cancer: economic consequences, health, and the role of surgery. Otolaryngol Head Neck Surg 2020; 162 (03) 296-303
- 54 Gollnick S, Anton K. Development of a registry for patients treated with photodynamic therapy (conference presentation). In: Kessel DH, Hasan T. eds. Optical Methods for Tumor Treatment and Detection: Mechanisms and Techniques in Photodynamic Therapy XXVII. Vol. 10476. Bellingham, WA: SPIE; 2018: 104760M
- 55 Souho T, Lamboni L, Xiao L, Yang G. Cancer hallmarks and malignancy features: gateway for improved targeted drug delivery. Biotechnol Adv 2018; 36 (07) 1928-1945
- 56 Pérez-Herrero E, Fernández-Medarde A. Advanced targeted therapies in cancer: drug nanocarriers, the future of chemotherapy. Eur J Pharm Biopharm 2015; 93: 52-79
- 57 Dai X, Yu L, Zhao X, Ostrikov KK. Nanomaterials for oncotherapies targeting the hallmarks of cancer. Nanotechnology 2020; 31 (39) 392001
- 58 Lee D, Kwon S, Jang SY, Park E, Lee Y, Koo H. Overcoming the obstacles of current photodynamic therapy in tumors using nanoparticles. Bioact Mater 2021; 8: 20-34
- 59 Huang L, Asghar S, Zhu T. et al. Advances in chlorin-based photodynamic therapy with nanoparticle delivery system for cancer treatment. Expert Opin Drug Deliv 2021; 18 (10) 1473-1500
- 60 Hong EJ, Choi DG, Shim MS. Targeted and effective photodynamic therapy for cancer using functionalized nanomaterials. Acta Pharm Sin B 2016; 6 (04) 297-307
- 61 Itoo AM, Paul M, Padaga SG, Ghosh B, Biswas S. Nanotherapeutic intervention in photodynamic therapy for cancer. ACS Omega 2022; 7 (50) 45882-45909
- 62 dos Santos AF, Arini GS, de Almeida DRQ, Labriola L. Nanophotosensitizers for cancer therapy: a promising technology?. JPhys Mater 2021; 4 (03) 034013
- 63 Wang D, Fei B, Halig LV. et al. Targeted iron-oxide nanoparticle for photodynamic therapy and imaging of head and neck cancer. ACS Nano 2014; 8 (07) 6620-6632
- 64 Jerjes W, Theodossiou TA, Hirschberg H. et al; From Basic Mechanisms to Clinical Research. Photochemical internalization for intracellular drug delivery: from basic mechanisms to clinical research. J Clin Med 2020; 9 (02) 528
- 65 O'Rourke C, Hopper C, MacRobert AJ, Phillips JB, Woodhams JH. Could clinical photochemical internalisation be optimised to avoid neuronal toxicity?. Int J Pharm 2017; 528 (1–2): 133-143
- 66 Sultan AA, Jerjes W, Berg K. et al. Disulfonated tetraphenyl chlorin (TPCS2a)-induced photochemical internalisation of bleomycin in patients with solid malignancies: a phase 1, dose-escalation, first-in-man trial. Lancet Oncol 2016; 17 (09) 1217-1229
- 67 Nguyen A, Bhandari C, Keown M. et al. Increasing the dye payload of cetuximab-IRDye800CW enables photodynamic therapy. Mol Pharm 2024; 21 (07) 3296-3309
- 68 Cognetti DM, Johnson JM, Curry JM. et al. Phase 1/2a, open-label, multicenter study of RM-1929 photoimmunotherapy in patients with locoregional, recurrent head and neck squamous cell carcinoma. Head Neck 2021; 43 (12) 3875-3887
- 69 Cognetti DM, Curry JM, Johnson J. et al. Safety and efficacy findings from a phase Ib/II study of ASP-1929 photoimmunotherapy with pembrolizumab in recurrent and/or metastatic head and neck squamous cell carcinoma. Head Neck 2025; 47 (01) 1-15
- 70 Lorenz KJ, Maier H. Photodynamic therapy with meta-tetrahydroxyphenylchlorin (Foscan) in the management of squamous cell carcinoma of the head and neck: experience with 35 patients. Eur Arch Otorhinolaryngol 2009; 266 (12) 1937-1944
- 71 Schweitzer VG. PHOTOFRIN-mediated photodynamic therapy for treatment of early stage oral cavity and laryngeal malignancies. Lasers Surg Med 2001; 29 (04) 305-313
- 72 Ikeda H, Ohba S, Egashira K, Asahina I. The effect of photodynamic therapy with talaporfin sodium, a second-generation photosensitizer, on oral squamous cell carcinoma: a series of eight cases. Photodiagnosis Photodyn Ther 2018; 21: 176-180
- 73 Ikeda H, Tobita T, Ohba S, Uehara M, Asahina I. Treatment outcome of Photofrin-based photodynamic therapy for T1 and T2 oral squamous cell carcinoma and dysplasia. Photodiagnosis Photodyn Ther 2013; 10 (03) 229-235
- 74 Kübler AC, de Carpentier J, Hopper C, Leonard AG, Putnam G. Treatment of squamous cell carcinoma of the lip using Foscan-mediated photodynamic therapy. Int J Oral Maxillofac Surg 2001; 30 (06) 504-509
- 75 Toratani S, Tani R, Kanda T, Koizumi K, Yoshioka Y, Okamoto T. Photodynamic therapy using Photofrin and excimer dye laser treatment for superficial oral squamous cell carcinomas with long-term follow up. Photodiagnosis Photodyn Ther 2016; 14: 104-110
- 76 Biel MA. Photodynamic therapy treatment of early oral and laryngeal cancers. Photochem Photobiol 2007; 83 (05) 1063-1068
- 77 Jerjes W, Upile T, Alexander Mosse C. et al. Prospective evaluation of 110 patients following ultrasound-guided photodynamic therapy for deep seated pathologies. Photodiagnosis Photodyn Ther 2011; 8 (04) 297-306
- 78 Hosokawa S, Takahashi G, Sugiyama KI. et al. Porfimer sodium-mediated photodynamic therapy in patients with head and neck squamous cell carcinoma. Photodiagnosis Photodyn Ther 2020; 29: 101627
- 79 Hopper C, Kübler A, Lewis H, Tan IB, Putnam G. mTHPC-mediated photodynamic therapy for early oral squamous cell carcinoma. Int J Cancer 2004; 111 (01) 138-146
- 80 Tan IB, Dolivet G, Ceruse P, Vander Poorten V, Roest G, Rauschning W. Temoporfin-mediated photodynamic therapy in patients with advanced, incurable head and neck cancer: a multicenter study. Head Neck 2010; 32 (12) 1597-1604
- 81 Carvalho AL, Salvajoli JV, Kowalski LP. A comparison of radiotherapy or radiochemotherapy with symptomatic treatment alone in patients with advanced head and neck carcinomas. Eur Arch Otorhinolaryngol 2000; 257 (03) 164-167