

RSS-Feed abonnieren
DOI: 10.1055/s-0045-1814384
A Randomized Double-Blind Clinical Trial Comparing Mannitol-Based Regimens and Water as Oral Contrast Agents With a Psyllium Arm, for CT Enterography: Impact on Imaging Performance and Tolerability
Autor*innen
Funding None.


Abstract
Background
Adequate bowel distension is critical for optimal diagnostic accuracy in computed tomography (CT) enterography (CTE). Although mannitol is commonly used as a neutral oral contrast agent, the optimal concentration remains undefined. The role of fiber adjuncts such as psyllium has not been fully explored. This randomized trial aimed to compare the efficacy and tolerability of varying mannitol concentrations with and without psyllium versus water.
Methods
Three hundred patients undergoing CTE were randomized into six groups: water, 1% mannitol, 2% mannitol, 3% mannitol, 3% mannitol + post-CT water, and 3% mannitol + psyllium. Quantitative and qualitative bowel distension, fold visibility, homogeneity, and adverse events were assessed across groups. Statistical analysis was performed using “R” and statistical packages multcomp, dunn.test, ggstats2, ggstatsplot, dplyr, etc. were used to analyze and visualize the data. Continuous data of groups was compared using analysis of variance with post-hoc Tukey's honestly significant difference test. A p-value of less than 0.05 was taken as significant.
Results
3% mannitol + psyllium achieved superior mean luminal distension in the ileum (2.28 cm, 95% confidence interval [CI] 2.25–2.31) compared with 3% mannitol alone (2.12 cm, 95% CI 2.08–2.16), 2% mannitol (1.49 cm, 95% CI 1.46–1.52), 1% mannitol (1.30 cm, 95% CI 1.26–1.34), and water (0.67 cm, 95% CI 0.63–0.71) (p < 0.001). Similar trends were observed for the jejunum and terminal ileum (p < 0.001). Fold visibility and contrast homogeneity were significantly better with 3% mannitol + psyllium (p < 0.001). Diarrhea was most frequent with 3% mannitol alone (48%) and 3% mannitol + post-CT water (44%), but reduced to 28% with 3% mannitol + psyllium (p = 0.02). No severe adverse events were reported except for diarrhea, a feeling of fullness, nausea, vomiting, headache, and others with increasing concentration of mannitol.
Conclusion
3% mannitol with psyllium provides optimal bowel distension and mucosal visualization in CTE with improved tolerability compared with mannitol alone. This combination represents an effective and patient-friendly preparation for routine clinical use in small bowel imaging. Our study is the first to demonstrate the synergistic benefit of mannitol and psyllium in achieving optimal small bowel distension with reduced adverse effects in a randomized double-blind design with extended adverse event monitoring.
Trial Registration
Clinical Trials Registry of India (CTRI/2024/02/063015)
Keywords
CT enterography (CTE) - mannitol - psyllium adjunct - bowel distension - neutral contrast agents - patient tolerabilityIntroduction
The small intestine, anatomically divided into the duodenum, jejunum, and ileum, plays a vital role in digestion, nutrient absorption, and fluid-electrolyte homeostasis. Its considerable length, variable positioning, peristaltic movement, and overlapping loops make it a particularly challenging region to evaluate using conventional diagnostic techniques.[1] [2] [3]
Clinical Significance and Imaging Need
Conditions such as Crohn's disease, obscure gastrointestinal (GI) bleeding, neoplasms, and malabsorption syndromes often affect the small bowel and may present with nonspecific symptoms like abdominal pain, anemia, and weight loss. These characteristics necessitate effective imaging for early detection and management. Computed tomography (CT) enterography (CTE) has emerged as a pivotal modality for small bowel evaluation due to its ability to provide high-resolution, cross-sectional imaging with detailed visualization of the bowel wall, mucosa, mesentery, and adjacent structures.[2] [4] [5]
Role of Contrast Agents in CTE
The diagnostic quality of CTE relies heavily on adequate luminal distension, which enhances the detection of mucosal abnormalities. Historically, positive contrast agents like diluted barium and iodinated solutions have been used, but they tend to obscure mural details due to their high attenuation.[3] [6] [7] [8] [9] In contrast, neutral agents such as water, polyethylene glycol (PEG), mannitol, and psyllium provide better wall delineation with minimal artifacts.
Mannitol, due to its favorable osmotic properties and cost-effectiveness, is commonly used to achieve consistent bowel distension. However, higher concentrations may cause adverse effects like diarrhea and bloating.[10] [11] Psyllium, a natural soluble fiber with hygroscopic and gel-forming properties, has shown promise in enhancing intraluminal fluid retention and promoting more uniform bowel expansion with improved patient tolerance.[12] [13] Negative agents like air and CO2, though occasionally used, are generally unsuitable for routine small bowel imaging.[14] [15] [16] [17]
Study Rationale and Gap in Literature
Despite the routine use of mannitol and water in CTE, there is no established consensus on the optimal concentration of mannitol that maximizes diagnostic performance while minimizing patient discomfort. Additionally, the potential of adjunct agents like psyllium to reduce mannitol-induced adverse effects has not been systematically studied. Previous research, such as studies by Prakashini et al and Thati et al, highlighted mannitol's diagnostic superiority over other contrast agents but were limited by single-concentration protocols and lacked long-term adverse reaction monitoring. For example, while Wong et al reported suboptimal results using psyllium alone, its combination with mannitol remains underexplored.
Aims and Objectives
The primary aim of this study was to systematically evaluate the efficacy and tolerability of varying concentrations of mannitol, alone and in combination with psyllium, compared with water, as oral endoluminal contrast agents for CTE. The goal was to optimize both diagnostic image quality and patient comfort.
The primary objectives were to quantitatively and qualitatively assess small bowel distension, fold visibility, and luminal homogeneity using different contrast regimens and to compare their diagnostic efficacy across various small bowel segments (jejunum, ileum, and terminal ileum).
Secondary objectives included evaluating the incidence, severity, and timing of adverse drug reactions (ADRs), assessing patient tolerance through structured symptom questionnaires, and generating evidence-based recommendations for optimizing CTE contrast protocols.
Methodology
This prospective, randomized, double-blind clinical trial included a total of 300 adult patients aged 18 to 70 years, referred patients aged 18 to 70 years who were referred for contrast-enhanced CTE and able to complete the all study procedures were included. Patients with surgically altered gastrointestinal anatomy (e.g., bowel resection, stoma), strictures, stenosis, adhesions, gross ascites , known bowel malignancy or any active gastrointestinal disease that could affect bowel distension or image interpretation were excluded—at the Department of Radiodiagnosis, Jawaharlal Nehru Medical College and Hospital, Aligarh Muslim University, Aligarh, Uttar Pradesh, India. The study was approved by the Institutional Ethics Committee (IEC), and written informed consent was obtained from all participants prior to enrollment. Patients were consecutively recruited between February 2024 and May 2025.
Eligible patients were randomized into one of six groups using a computer-generated sequence and block randomization with variable block sizes to maintain balanced group allocation. The six study groups were water, 1% mannitol, 2% mannitol, 3% mannitol, 3% mannitol combined with post-CT water, and 3% mannitol combined with psyllium. Each group comprised 50 patients. Mannitol solutions were prepared from a 20% w/v stock as follows: 1% mannitol – 50 mL of 20% mannitol diluted in 950 mL water; 2% mannitol – 100 mL in 900 mL water; and 3% mannitol – 150 mL in 850 mL water (total vol. 1 L). For the psyllium subgroup, 2.5 g of psyllium husk was mixed immediately before ingestion to ensure uniform dispersion and prevent premature gelation. This low diagnostic dose, approximately 10% of the upper therapeutic limit (15–25 g), was chosen to balance viscosity and patient comfort.
Although initially designed as triple-blind, due to logistical constraints during allocation and follow-up, the trial was conducted in a double-blind format, which may introduce minimal observer or assessor bias. The radiologist interpreting the CTE images and the investigator assessing ADRs were blinded to group allocation. However, personnel administering the oral contrast were necessarily aware of its contents. Patients themselves were partially blinded, although differences in taste and texture may have provided clues regarding group allocation.
The sample size was calculated based on prior studies (Prakashini et al), anticipating a difference of approximately 0.5 cm in mean bowel diameter between groups, with a standard deviation of 0.8 cm. To achieve 80% power with a significance level of 0.05, a minimum of 42 patients per group was required; this was rounded up to 50 patients per group to allow for subgroup analyses and potential dropouts. Scoring system used was: 0 = fair, 1 = good, and 2 = excellent.
Each patient received 1 L of the assigned oral contrast agent, administered over 45 minutes in divided doses. In the 3% mannitol + psyllium group, psyllium was freshly mixed to ensure homogeneity. For the 3% mannitol + post-CT water group, an additional 500 mL of water was administered immediately after CTE. CT scans were performed using a Siemens 128-slice multidetector CT scanner, with enteric phase acquisition at 40 seconds postintravenous administration of iodinated contrast. Images were reconstructed in axial and coronal planes as shown in [Figs. 1] and [2].


For quantitative analysis, bowel distension was measured by assessing the maximum outer-to-outer diameter of two well-distended bowel loops –one on the right and one on the left side of the abdomen –on axial CT images. Measurements were standardized at specific anatomical landmarks. Jejunal loops were measured at the levels of the superior mesenteric artery (SMA), renal arteries, and inferior mesenteric artery (IMA); ileal loops were evaluated at the levels of the aortic bifurcation, common iliac bifurcation, and deep pelvis; and the terminal ileum was assessed just proximal to the ileocecal (IC) junction. Distension was graded as follows: Grade 0 for collapsed bowel or poor wall-to-lumen contrast, Grade I for distension ≤1.5 cm with incomplete fold visibility, and Grade II for distension >1.5 cm with complete fold visibility.
For qualitative analysis, images were evaluated on coronal planes based on three parameters: distension, fold visibility, and homogeneity of intraluminal content. Each was graded using a continuous 3-point scale: Grade 0 : good, Grade 1:fair, and Grade 2: excellent. ADRs –including diarrhea, abdominal fullness, nausea, headache, and vomiting –were monitored immediately postprocedure, at 2 hours, and at 48 hours postprocedure via telephone interview. Among them diarrhea was exclusively studied.
The study was prospectively registered with the Clinical Trials Registry of India (CTRI/2024/02/063015) and received ethical approval from the ICE. Statistical analysis is done using “R,” and statistical packages multcomp, dunn.test, ggstats2, ggstatsplot, dplyr, etc. were used for analysis and to visualize the data. Continuous data of groups was compared using analysis of variance (ANOVA) with post-hoc Tukey's honestly significant difference (HSD) test. A p-value of less than 0.05 was taken as significant.
Results
All continuous variables were analyzed using ANOVA with Tukey's HSD for post-hoc testing. Categorical variables (ADR frequencies) were compared using the chi-square test. Effect sizes are reported using Cohen's d (quantitative) and Cramer's V (qualitative/categorical).
-
Quantitative distension analysis:
Mean distension values were calculated for the jejunum, ileum, and terminal ileum across all six contrast groups.
-
1.1 Ileum: 3% mannitol + psyllium group achieved the highest mean diameter (2.28 ± 0.16 cm; 95% confidence interval [CI]: 2.24–2.32), followed by 3% mannitol (2.12 ± 0.18 cm; 95% CI: 2.08–2.17), 2% mannitol (1.49 ± 0.15 cm), 1% mannitol (1.30 ± 0.14 cm), and water (0.67 ± 0.11 cm) as shown in [Fig. 3].
-
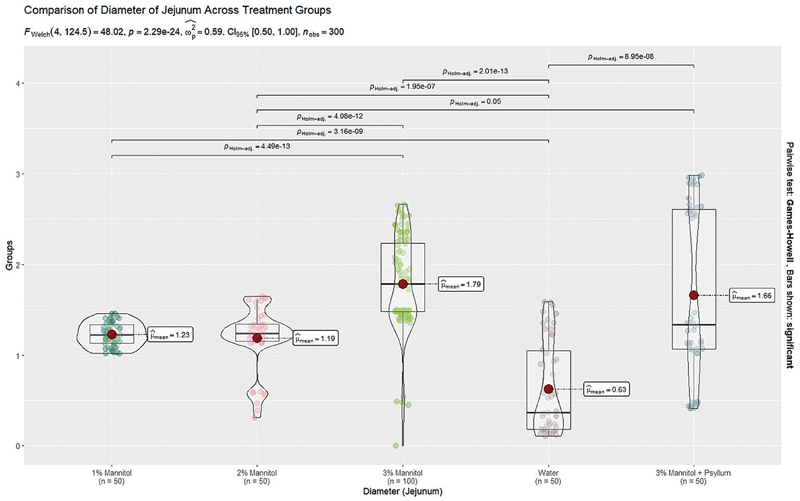
1.2 Jejunum: 3% mannitol alone showed slightly superior distension (1.79 ± 0.13 cm; 95% CI: 1.75–1.83), compared with 3% mannitol + psyllium (1.66 ± 0.12 cm), 2% mannitol (1.32 ± 0.14 cm), 1% mannitol (1.24 ± 0.15 cm), and water (0.63 ± 0.09 cm) as shown in [Fig. 4].
-
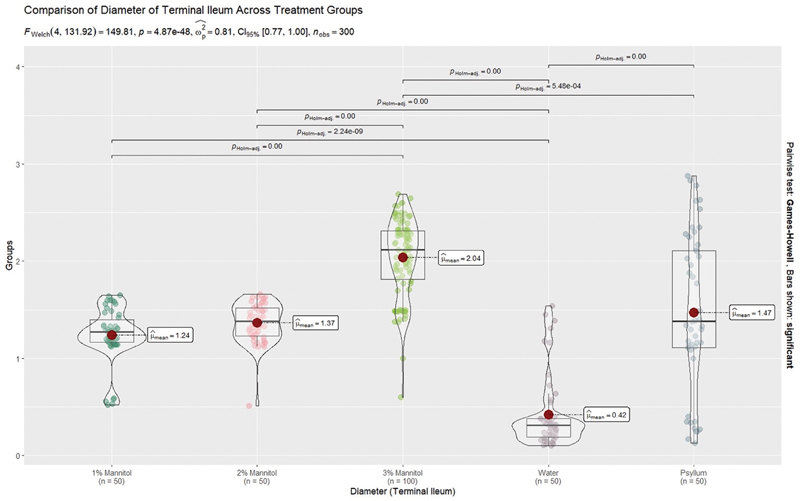
1.3 Terminal ileum: 3% mannitol achieved the best distension (2.04 ± 0.17 cm; 95% CI: 1.99–2.08), followed by 3% mannitol + psyllium (1.86 ± 0.14 cm), 2% mannitol (1.41 ± 0.12 cm), 1% mannitol (1.26 ± 0.13 cm), and water (0.72 ± 0.08 cm) as shown in [Fig. 5].
-

Although the mean luminal diameters for the 3% mannitol group were numerically higher than those for 3% mannitol + psyllium in most of the segments, the difference was not statistically significant (p > 0.05). Any apparent visual variation between the two groups likely reflects normal peristaltic variation rather than technical or labeling differences.
Qualitative Image Evaluation
Distension Score
Qualitative distention improved progressively with increasing mannitol concentration as shown in [Fig. 6]. In the ileum, 1% mannitol provided fair distention (mean score 1.52), while 2% achieved better consistency (1.80). Both 3% mannitol (1.94) and 3% mannitol with psyllium (1.96) demonstrated uniform and optimal diagnostic quality. Water, in contrast, performed poorly with a score of 0.46. The jejunum showed the highest variability, with water (0.34) and 1% mannitol (0.38) yielding frequent underdistention. However, 3% mannitol (1.18) and its psyllium combination (1.24) surpassed the diagnostic threshold. In the terminal ileum, water again underperformed (0.40), while 1% and 2% mannitol provided fair scores (0.7 and 1.52). Superior mural separation was noted with 3% mannitol (1.83) and 3% mannitol plus psyllium (1.82), making them ideal for detecting pathologies such as Crohn's disease. Overall, the findings indicate that higher mannitol concentrations, especially when combined with psyllium, substantially enhance bowel distention quality, whereas water and lower concentrations are diagnostically inadequate.

Fold visibility: A critical parameter for detecting early mucosal changes, improved progressively with increasing mannitol concentration, especially when combined with psyllium as shown in [Fig. 7]. In the ileum, fold clarity rose from 0.86 with 1% mannitol to a near-perfect 1.96 with 3% mannitol + psyllium, while water performed poorly (0.32), often obscuring fine mucosal detail. In the jejunum, overall visibility was lower, likely due to peristalsis. Water (0.5) and 1% mannitol (0.6) were inadequate; 2% mannitol improved clarity to 0.94, whereas 3% mannitol (1.31) and its combination with psyllium (1.34) reached diagnostically acceptable levels. The terminal ileum showed peak performance with 3% mannitol (1.80) and 3% mannitol + psyllium (1.82), correlating with sharply defined mucosal ridges. Water again fell below diagnostic thresholds (0.26). Overall, fold visibility correlated positively with contrast concentration, with optimal results in the highest mannitol groups.

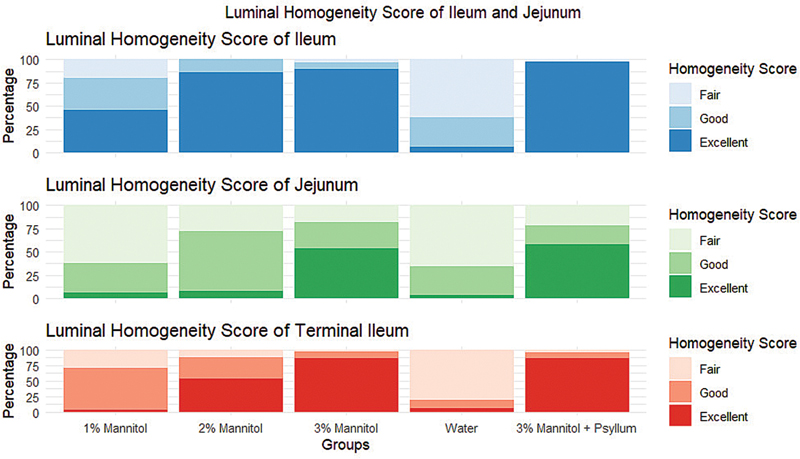
Homogeneity: Indicating even contrast distribution along the bowel wall, is essential for assessing mucosal pathologies such as inflammation or ulceration. In the ileum, homogeneity improved consistently with rising mannitol concentration, peaking with 3% mannitol + psyllium, which provided a uniform gel-like coating. Water and 1% mannitol often failed to achieve adequate coverage. The jejunum showed lower overall homogeneity due to increased peristalsis, though 3% mannitol and its combination with psyllium maintained fair to good consistency, while water exhibited pooling and disrupted clarity. In the terminal ileum, 3% mannitol (1.83) and 3% + psyllium (1.82) again showed excellent uniformity, while lower concentrations and water underperformed, often leading to incomplete mucosal visualization.
3% mannitol + psyllium demonstrated the best contrast layering with minimal pooling. Homogeneity scores were statistically better than all other groups (p < 0.001), as shown in [Fig. 8].
Adverse Drug Reactions
Immediate-Onset Adverse Reactions
As shown in [Fig. 9], the highest incidence of ADRs occurred immediately after contrast ingestion.
-
Diarrhea was most common in the 3% mannitol (48%), 3% mannitol + post-CT water (44%), and 3% mannitol + psyllium (28%) groups.
-
Fullness was highest in 3% mannitol + post-CT water (66%) and 3% mannitol (48%).
-
Headache and nausea were reported in 30 and 14% (3% mannitol), and 26% each (3% mannitol + post-CT water), respectively.
-
Minor symptoms included flatulence, abdominal discomfort, and fatigue.

ADRs at 2 Hours Post-CT
At 2 hours ([Fig. 10]), overall symptom frequency declined, notably in lower concentration groups.
-
Diarrhea persisted in 3% mannitol + post-CT water (46%), followed by 3% mannitol (18%) and 3% mannitol + psyllium (14%).
-
Headache remained in 2% mannitol (14%) and 3% mannitol + water (8%).
-
Nausea, fullness, and flatulence continued in higher concentration groups.

ADRs at 48 Hours Post-CT
By 48 hours ([Fig. 11]), most symptoms resolved.
-
Diarrhea persisted in 3% mannitol + post-CT water (24%), with minimal reports in other groups.
-
Headache, nausea, and fullness largely resolved.
-
Fever/chills occurred in 2 to 4% of patients in the 3% mannitol and 3% mannitol + psyllium groups.

Incidence: Diarrhea was most common in the 3% mannitol group (48%) and 3% mannitol + post-CT water group (44%). Other reported symptoms included nausea (15% in 3% mannitol), bloating (22%), and headache (5%). Water and 1% mannitol groups had the lowest incidence of ADRs as shown in [Tables 1] and [2].
Abbreviations: ADR, adverse drug reaction; CT, computed tomography.
Abbreviation: CT, computed tomography.
Mitigation with psyllium: The addition of psyllium to 3% mannitol significantly reduced the frequency of diarrhea to 28% (p = 0.02 vs. 3% mannitol alone), along with a general reduction in overall symptom burden. This suggests that psyllium mitigates the osmotic side effects of mannitol by increasing intraluminal viscosity and prolonging transit time as shown in [Tables 1] and [2].
Onset and duration: Most ADRs occurred within the first 2 hours post-CTE and typically resolved by 48 hours. No serious or persistent adverse events were noted during the study duration.
ADRs were most frequent with 3% mannitol alone, where diarrhea, nausea, and abdominal fullness were commonly reported. Unexpectedly, the 3% mannitol + post-CT water group exhibited higher and more prolonged ADRs, particularly diarrhea. This may be attributed to the additional volume enhancing osmotic shifts and accelerating gut motility. In contrast, the 3% mannitol + psyllium group demonstrated a clinically relevant reduction in both incidence and severity of ADRs, affirming psyllium's role in modulating the GI response to hyperosmolar contrast agents. Lower concentrations of mannitol (1 and 2%) were well tolerated, and water produced minimal side effects as shown in [Figs. 9]–[11].
Interpretation and clinical insight:
-
The incidence and severity of ADRs were clearly dose-dependent, with 3% mannitol and its combinations showing the highest frequencies.
-
The post-CT water group was included to assess whether additional hydration could reduce osmotic symptoms from mannitol. However, results indicated an increased incidence of diarrhea and fullness, likely due to augmented osmotic fluid shifts. These findings also suggest that low-volume oral contrast regimens (1 L) are better tolerated than high-volume (≥ 2 L) preparations, which may exacerbate diarrhea and reduce patient compliance.
-
Psyllium as an adjunct was associated with a reduction in ADRs, especially diarrhea and fullness, indicating potential benefit in improving tolerability.
Discussion and Conclusion
This randomized clinical trial clearly demonstrates that achieving optimal small bowel distension and image quality in CTE is dependent on both the concentration of mannitol and the use of adjuncts such as psyllium. Our results establish that 3% mannitol combined with psyllium outperformed other contrast protocols across multiple diagnostic parameters while offering an improved tolerability profile.
Quantitatively, the combination of 3% mannitol with psyllium resulted in superior distension of the ileum and consistently high performance in both the jejunum and terminal ileum. Psyllium's gel-forming properties appeared to enhance contrast retention, particularly in the jejunum, which is traditionally more difficult to distend adequately. In contrast, lower concentrations of mannitol and water resulted in suboptimal bowel distension.
Qualitatively, fold visibility and homogeneity of luminal contents were highest with the 3% mannitol plus psyllium group. This combination produced a stable, layered contrast column essential for accurate detection of subtle mucosal pathology. Conversely, water and 1% mannitol frequently resulted in pooling and artifacts that degraded image quality.
A significant contribution of our study is the systematic evaluation of ADRs. While 3% mannitol alone was associated with the highest rates of diarrhea and abdominal fullness, the lower incidence of diarrhea in the 3% mannitol + psyllium group likely reflects psyllium's gel-forming and water-retentive properties, which reduce osmotic load, slow intestinal transit, and stabilize luminal content—thereby improving tolerability without compromising diagnostic quality.
This finding is particularly relevant to clinical practice, as patient tolerance is a key consideration in imaging protocols. Interestingly, the 3% mannitol plus post-CT water group exhibited unexpectedly high and prolonged symptoms, suggesting that additional water administration after CTE may exacerbate osmotic effects rather than alleviate them. This finding suggests that additional post-CT water administration may accelerate osmotic shifts within the bowel lumen, counterintuitively increasing diarrhea risk. Prospective studies are needed to validate this observation regarding post-CT water exacerbating ADRs.
Comparing our findings with existing literature highlights several advancements. Previous studies by Prakashini et al and Thati et al confirmed the superiority of mannitol over water, but different concentration gradients or long-term side effects were not explored. Singla et al demonstrated that PEG provided superior distension but was poorly tolerated; our results suggest that 3% mannitol with psyllium nearly matches PEG in image quality while offering better tolerability. Wong et al had shown that psyllium alone was ineffective as a contrast agent; however, our study demonstrates that combining psyllium with mannitol synergistically improves homogeneity and reduces ADRs. All have used a single concentration of mannitol, whereas our multiconcentration design with adjunct strategies provides a more granular understanding of protocol optimization.
The clinical implications of this study are clear. Based on diagnostic performance and patient comfort, 3% mannitol with psyllium should be adopted as the default oral contrast agent for CTE, particularly for challenging cases such as IBD, suspected neoplasms, and obscure GI bleeding. When psyllium is unavailable, 3% mannitol remains a viable second option, though with increased ADR risk. For elderly or frail patients, 2% mannitol provides an acceptable compromise between image quality and tolerability. In contrast, 1% mannitol and water are not suitable for diagnostic enterography beyond basic screening applications. Importantly, mannitol combined with psyllium offers a cost-effective alternative to PEG-based preparations, with comparable or superior imaging performance and improved patient tolerability, making it particularly suitable for high-volume centers and resource-constrained settings.
Our study offers several strengths, including a large cohort size (n = 300), double-blind methodology, novel adjunct evaluation, extended ADR tracking (48 hours), and detailed segmental analysis. However, certain limitations warrant consideration. This was a single-center study, multicenter validation is needed to increase generalizability. We did not assess interobserver variability, which is relevant in the subjective interpretation of CTE images. Additionally, we did not directly compare our protocols against PEG, sorbitol, or methylcellulose, nor did we explore varying doses of psyllium. Functional motility imaging was not included, and pediatric and elderly extremes were excluded. Another limitation is that no interobserver agreement was assessed; future studies should include kappa analysis or similar methods to quantify reader variability. External validation across diverse populations is required before widespread adoption. Given the robust randomized design and large cohort, our findings are likely generalizable to routine CTE practice in similar clinical settings. Potential use in pediatric/adolescent populations remains unexplored, which will be an important focus of future work, particularly given the widespread use of CTE in resource-constrained settings.
Additional limitations include the fact that full triple-blinding was not feasible, as personnel preparing the oral contrast were aware of the group allocation. Furthermore, patients were only partially blinded, and differences in the taste or texture of contrast agents (particularly with psyllium) may have introduced reporting bias in adverse event assessments. Although a fixed oral contrast volume (1 L) was used based on prior recommendations, the optimal volume to balance efficacy and tolerability was not explored. We also did not perform subgroup analysis by body mass index, or specific clinical indication (e.g., IBD vs. neoplasm), which may influence bowel motility and contrast distribution. Finally, while mannitol + psyllium appears to be a cost-effective alternative to PEG, no formal cost-effectiveness analysis was conducted in this study.
In conclusion, this trial provides robust evidence supporting the use of 3% mannitol with psyllium as an optimal, patient-centered contrast protocol for CTE. Future research should focus on multicenter validation, psyllium dose optimization, comparisons with other modern agents, and broader population applicability as well as cost-effectiveness analysis to ensure feasibility in various clinical settings. By refining contrast protocols in this manner, we can further enhance the diagnostic yield and patient experience of CTE in routine clinical practice.
Conflict of Interest
None declared.
Acknowledgment
The authors gratefully acknowledge the institutional and technical support received during the study.
-
References
- 1 Ilangovan R, Burling D, George A, Gupta A, Marshall M, Taylor SA. CT enterography: review of technique and practical tips. Br J Radiol 2012; 85 (1015) 876-886
- 2 McCollough CH, Leng S, Yu L, Fletcher JG. Dual- and multi-energy CT: principles, technical approaches, and clinical applications. Radiology 2015; 276 (03) 637-653
- 3 Singla R, Ranjan P, Mehta D, Yadav V. Comparative performance of neutral oral contrast agents for CT enterography: a prospective randomized study. J Gastrointest Abdom Radiol ISGAR 2022; 5 (01) 16-22
- 4 Wong J, Roger M, Moore H. Performance of two neutral oral contrast agents in CT enterography. J Med Imaging Radiat Oncol 2015; 59 (01) 34-38
- 5 Minordi LM, Vecchioli A, Mirk P, Bonomo L. CT enterography with polyethylene glycol solution vs CT enteroclysis in small bowel disease. Br J Radiol 2011; Feb; 84 (998) 112-119
- 6 Pilleul F, Saurin JC, Ganne N. et al. Computed tomography enteroclysis: a valuable tool for evaluating patients with obscure gastrointestinal bleeding. AJR Am J Roentgenol 2006; 187 (03) 741-746
- 7 Patel A, Lalwani N, Kielar A. Use of oral contrast in 2024: primer for radiologists. Abdom Radiol (NY) 2024; 49 (08) 2953-2959
- 8 Ajaj W, Goehde SC, Schneemann H, Ruehm SG, Debatin JF, Lauenstein TC. Oral contrast agents for small bowel MRI: comparison of different additives to optimize bowel distension. Eur Radiol 2004; Mar; 14 (03) 458-464
- 9 Khan H, Shah SM, Ali S. et al. Comparison of mannitol, water and positive oral contrast. Pak J Med Health Sci 2021; 15 (04) 1054-1058
- 10 Prakashini K, Kakkar C, Sambhaji C, Shetty CM, Rao VR. Quantitative and qualitative bowel analysis using mannitol, water and iodine-based endoluminal contrast agent on 64-row detector CT. Indian J Radiol Imaging 2013; Oct; 23 (04) 373-378
- 11 Mohd Noor NA, Shamsudin SN, Hussain H. et al. Diagnostic value of pineapple juice and mannitol in CT enterography. Med J Malaysia 2023; 78 (06) 775-780
- 12 Parashari UC, Singh R, Kapoor S. et al. Quantitative and qualitative analysis of bowel with iodine and mannitol-based oral contrast agent. Healthc Bull 2023; 9 (02) 38-44
- 13 Maglinte DDT, Sandrasegaran K, Lappas JC. CT enteroclysis: technique and diagnostic utility. Radiology 2003; 228 (03) 647-652
- 14 Paulsen SR, Huprich JE, Fletcher JG. et al. CT enterography: noninvasive evaluation of Crohn's disease and obscure gastrointestinal bleeding. Radiographics 2006; 26 (03) 641-657
- 15 Rathi V. Feasibility of simple oral preparation contrast-enhanced CT colonography (SOP-CE-CTC) using mannitol as a neutral oral contrast agent. J Gastrointest Abdom Radiol 2022;5(12)
- 16 Thati SS, Nagegowda R, Sakalecha AK, Savagave SG, Patil DT. Comparison of mannitol, water, and iodine-based oral contrast in the evaluation of the bowel by multi-detector computed tomography. Cureus 2022; 14 (04) e24316
- 17 Zulkifle AF, Siti Soraya AR, Hamzaini AH. Comparison of pineapple juice and mannitol as oral contrast agents for magnetic resonance enterography. Med J Malaysia 2023; 78 (06) 774-779
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
24. Dezember 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Ilangovan R, Burling D, George A, Gupta A, Marshall M, Taylor SA. CT enterography: review of technique and practical tips. Br J Radiol 2012; 85 (1015) 876-886
- 2 McCollough CH, Leng S, Yu L, Fletcher JG. Dual- and multi-energy CT: principles, technical approaches, and clinical applications. Radiology 2015; 276 (03) 637-653
- 3 Singla R, Ranjan P, Mehta D, Yadav V. Comparative performance of neutral oral contrast agents for CT enterography: a prospective randomized study. J Gastrointest Abdom Radiol ISGAR 2022; 5 (01) 16-22
- 4 Wong J, Roger M, Moore H. Performance of two neutral oral contrast agents in CT enterography. J Med Imaging Radiat Oncol 2015; 59 (01) 34-38
- 5 Minordi LM, Vecchioli A, Mirk P, Bonomo L. CT enterography with polyethylene glycol solution vs CT enteroclysis in small bowel disease. Br J Radiol 2011; Feb; 84 (998) 112-119
- 6 Pilleul F, Saurin JC, Ganne N. et al. Computed tomography enteroclysis: a valuable tool for evaluating patients with obscure gastrointestinal bleeding. AJR Am J Roentgenol 2006; 187 (03) 741-746
- 7 Patel A, Lalwani N, Kielar A. Use of oral contrast in 2024: primer for radiologists. Abdom Radiol (NY) 2024; 49 (08) 2953-2959
- 8 Ajaj W, Goehde SC, Schneemann H, Ruehm SG, Debatin JF, Lauenstein TC. Oral contrast agents for small bowel MRI: comparison of different additives to optimize bowel distension. Eur Radiol 2004; Mar; 14 (03) 458-464
- 9 Khan H, Shah SM, Ali S. et al. Comparison of mannitol, water and positive oral contrast. Pak J Med Health Sci 2021; 15 (04) 1054-1058
- 10 Prakashini K, Kakkar C, Sambhaji C, Shetty CM, Rao VR. Quantitative and qualitative bowel analysis using mannitol, water and iodine-based endoluminal contrast agent on 64-row detector CT. Indian J Radiol Imaging 2013; Oct; 23 (04) 373-378
- 11 Mohd Noor NA, Shamsudin SN, Hussain H. et al. Diagnostic value of pineapple juice and mannitol in CT enterography. Med J Malaysia 2023; 78 (06) 775-780
- 12 Parashari UC, Singh R, Kapoor S. et al. Quantitative and qualitative analysis of bowel with iodine and mannitol-based oral contrast agent. Healthc Bull 2023; 9 (02) 38-44
- 13 Maglinte DDT, Sandrasegaran K, Lappas JC. CT enteroclysis: technique and diagnostic utility. Radiology 2003; 228 (03) 647-652
- 14 Paulsen SR, Huprich JE, Fletcher JG. et al. CT enterography: noninvasive evaluation of Crohn's disease and obscure gastrointestinal bleeding. Radiographics 2006; 26 (03) 641-657
- 15 Rathi V. Feasibility of simple oral preparation contrast-enhanced CT colonography (SOP-CE-CTC) using mannitol as a neutral oral contrast agent. J Gastrointest Abdom Radiol 2022;5(12)
- 16 Thati SS, Nagegowda R, Sakalecha AK, Savagave SG, Patil DT. Comparison of mannitol, water, and iodine-based oral contrast in the evaluation of the bowel by multi-detector computed tomography. Cureus 2022; 14 (04) e24316
- 17 Zulkifle AF, Siti Soraya AR, Hamzaini AH. Comparison of pineapple juice and mannitol as oral contrast agents for magnetic resonance enterography. Med J Malaysia 2023; 78 (06) 774-779