

Subscribe to RSS
DOI: 10.1055/s-0045-1814379
A journey through the anatomy of the cerebellum
Authors

Abstract
The present narrative review delves into the multifaceted roles of the cerebellum, highlighting its significance beyond traditional motor functions to encompass cognitive and behavior-related processes, as evidenced by advancements in functional neuroimaging. We provide a comprehensive summary of the cerebellum's embryological development, intricate microanatomy, macroanatomy, and vascular anatomy of the cerebellum, revealing how these aspects contribute to its unique circuitry and operational capabilities. A non-systematic literature search was conducted using the PubMed database, focusing on landmark and recent studies addressing the embryology, anatomy, clinical correlations and radiological aspects of the cerebellum. Ultimately, this review underscores the cerebellum's complex structure and diverse function, advocating for a deeper understanding to improve diagnostic and therapeutic approaches for cerebellar disorders.
INTRODUCTION
The word cerebellum, derived from Latin and meaning “little brain,” was first coined in the early sixteenth century. However, despite its name, this fascinating structure is anything but little in terms of organization, circuitry and its expanding role within the nervous system, becoming a focal point in contemporary neuroscience.
Classically considered a cornerstone for motor information processing and control, the cerebellum has emerged as an important player in cognitive and behavioral functions, as demonstrated by advancements in functional neuroimaging. A deeper understanding of its extensive connectivity, both intrinsic and extrinsic, can be better achieved through a careful study of its early developmental stages and topographic organization.
Therefore, the present review aims to provide a comprehensive overview of the cerebellum's embryological, anatomical and radiological features, emphasizing its unique role in neurological function and the impact of its dysfunction in various cerebellar disorders.
METHODS
We performed the current narrative review based on a non-systematic literature search conducted in the PubMed database up to April 30th. We included landmark studies, review articles, and recent publications related to cerebellar embryology, anatomy, function, and clinical correlations. The selection criteria prioritized relevance, scientific impact, and contribution to the anatomical and functional understanding of the cerebellum. Articles in English and Portuguese were considered, allowing the inclusion of both classical and updated references.
THE EMBRYOLOGIC DEVELOPMENT OF THE CEREBELLUM AND CEREBELLAR PATHWAYS
The cerebellum is a crucial structure within the central nervous system, playing a vital role in the coordination of voluntary movements, maintaining balance and posture, and regulating cognitive and emotional processes.[1] Understanding the embryologic development of the cerebellum and its associated pathways is essential for comprehending the full scope of its functions and potential disruptions.[2] Moreover, the study of cerebellar embryogenesis offers insights into the complex cellular and molecular mechanisms that govern the formation of this intricate brain region, providing a foundation for understanding cerebellar function and dysfunction.[1] [3]
The formation of the central nervous system in the embryo begins with the neural tube.[4] [5] Portions of the neural tube start secreting signaling molecules which further induce the differentiation of specific regions into particular structures.[6] In that sense, with adequate molecular stimuli, the hindbrain, or rhombencephalon, one of the primary vesicles of the neural tube, further differentiates into 7 rhombomeres. Amongst those, rhombomere 1 (r1) plays an important role as a precursor of the cerebellum.
Another important structure for cerebellar development is the isthmus, a constriction at the midbrain-hindbrain boundary positioned immediately rostral to r1.[7] This region plays a crucial role as an organizing center, orchestrating the development of the mid- and hindbrain through the secretion of signaling molecules, most notably Fgf8.[7] Specifically, Fgf8 exerts its influence by establishing gradients of morphogens, which, in turn, regulate gene expression and cell fate determination, which, ultimately, contribute to the development of r1 into the cerebellum.[6]
Also derived from the r1 is the rhombic lip (RL). The RL, mostly through expression of the transcription factor Atoh1, is essential for the generation of several important glutamatergic cell populations, including the granule cell precursors of the cerebellum, as well as neurons of pontine nucleus.[6] [8]
Alongside the RL, the ventricular zone (VZ) is of importance for neurogenesis. The VZ, which lines the fourth ventricle and is marked by Ptf1a expression, serves as the primary source of Purkinje cells, the principal neurons of the cerebellar cortex, as well as other important neurons, such as GABAergic interneurons.[9] Those cells are also important in providing trophic support to the RL-derived cells.[10]
While the VZ and the RL are generated by ventrally and intermediately located parts of the neuroepithelium, the roof plate (RP) is generated by dorsal portions of the neuroepithelium.[11] Specifically, the RP is associated with promoting signals for VZ cell proliferation and differentiation as well as the formation of the RL in itself.[12]
With the intricate interactions between the RP, RL, VZ and r1 and its molecular signaling events, briefly described above, the cerebellum can successfully develop with each of its proper components. However, several abnormalities can take place in this process, leading to important cerebellar dysfunction and associated clinical manifestations.[11]
Amongst the cerebellar malformations, the most common one consists of the Dandy-Walker malformation (DWM). DWM is present in 6.8 in every 100 thousand live births,[13] and its main characteristics consist of cystic dilatation of the fourth ventricle and hypoplasia or agenesis of the cerebellar vermis ([Figure 1]).[14] The condition presents with macrocephaly, hydrocephaly, developmental delay and/or ataxia.[14] Specifically, 80% of DWM patients present with hydrocephalus which frequently manifests with intracranial hypertension, macrocephaly, downward deviation of the eyeballs with retraction of the upper eyelids (setting sun sign), bulging of the fontanelle, dilation and congestion of the scalp veins and upward vertical gate paralysis.[15] Furthermore, ocular findings are common among DWS patients and also include lateral gaze palsy, nystagmus and strabismus, frequently presenting as diplopia.[16] Up to 40% of patient present with motor alternations including spasticity and around 20% with ataxia.[16]

The etiopathogenesis of DWM is not completely clear. It is believed to be related to both genetic and environmental causes.[17] Particularly, in a study by Sun et al. chromosomal abnormalities were found in 32.9% of patients, whereas other authors have identified subchromossomal alterations, including FOXC1 and ZIC1/4 deletion.[17] [18] [19] Pre-natal intracerebral hemorrhage has also been associated with DWM.[20] Furthermore, animal evidence suggests that the etiology of DWM is associated with disturbed molecular signaling and, therefore, abnormal migration of RL and VZ derived cells, leading to vermian hypoplasia.[19] [21]
Another important group of cerebellar malformations consists of Joubert Syndrome and related disorders (JSRD), which have an incidence of 1 in 80 thousand live births[22] and are characterized by agenesis or hypoplasia of the cerebellar vermis, thickened superior cerebellar peduncles, and an enlarged interpeduncular fossa, resulting in a distinctive molar tooth sign on axial magnetic resonance imaging (MRI) or computed tomography (CT) scans ([Figure 1]).[23] Clinically wise, JSRD presents with a combination of hypotonia, ataxia, developmental delay, intellectual disability, abnormal eye movements and breathing abnormalities. Particularly, JSRD patients frequently present with neonatal hypotonia which, when associated with irregular breathing pattern and altered eye movements, should suggest the diagnosis of JSRD.[24] Around 95% of patients present with global developmental delay and up ataxia is a common finding as well.[24] [25] Joubert Syndrome and related disorders have been associated with several genetic variants related to cilia formation and function.[26] Moreover, previous studies have suggested that JSRD are associate with impaired granule cell proliferation in the RL, suggesting alterations in important molecular signaling pathways.[27] [28]
Cerebellar hypoplasia (CH) is another important group of cerebellar malformations, characterized by a reduction in the overall size of the cerebellum. It can manifest in various forms, including unilateral (affecting only one side), global (affecting the entire cerebellum), vermian (affecting the vermis), or pontocerebellar (affecting both the cerebellum and the pons) ([Figure 1]). Ponto-cerebellar hypoplasia likely arises from the shared developmental origin of granule cells in the cerebellum and neurons in the pontine nuclei, both of which originate in the RL.[29] [30] Patients frequently present with cognitive and motor alterations. In detail, up to 87% of patients present with developmental delay, which frequently include speech alterations, hypotonia and ataxia in around 50%, ocular findings including nystagmus, strabismus, or abnormal ocular movements in 40%, spasticity in 30 and seizures in up to 20%.[31]
With regards to the etiology of CH, it is also associated with genetic and environmental factors. Several genes, including CASK, DAB1, OPHN1, RELN, CHD7, various tubulin genes, and several TSEN genes, have been linked to CH.[11] These genes play crucial roles in different stages of cerebellar development, such as progenitor cell proliferation, neuronal migration, and cell survival. Disruptions in these genes can lead to developmental defects and ultimately CH. In addition to genetic causes, CH can also result from non-genetic factors like congenital cytomegalovirus infection and perinatal exposure to alcohol and drugs like cocaine.[11]
In the extreme of the cerebellar malformations, there is cerebellar agenesis (CA), which is characterized by complete or near-complete agenesis of the cerebellum and is a rare malformation.[11] While individuals with CA may experience notable neurological deficits, especially in movement and speech, their overall functioning can be preserved.[32] Particularly, the symptoms overlap with those of CH neonatal hypotonia, delayed motor development, ataxia, oculomotor abnormalities and cognitive disfunctions[33] Regarding etiology, it has been associated with Ptf1a deletions.[34] Particularly, as previously described, Ptf1a is important in the VZ to the development of Purkinje cells and other GABAergic neurons. Without those neurons, RL cells do not have trophic support and are also lost.[10] Therefore, the result is cerebellar agenesis.
It is possible to comprehend how the intricate relationship between the VZ, RL, RP and r1, and its respective molecular markers, is important for proper cerebellar formation and how any disturbance in these complex relations can lead to cerebellar malformation and dysfunction.
MICROANATOMY AND CIRCUITRY OF THE CEREBELLUM
Despite representing only 10% of the brain's weight, the cerebellum contains up to 80% of the brain's neurons.[35] This discrepancy can be justified by its tightly folded structure, consisting of an inner white matter core covered by gray matter. This organization enables the cerebellum to have a unique and complex circuitry both within itself and in its connections to other parts of central nervous system.[36]
The cerebellar gray matter is organized into three layers: the internal granular layer, the middle Purkinje cell layer, and the external molecular layer ([Figure 2]). The internal granular layer has cell bodies, Golgi cells, Lugaro cells, unipolar brush cells and Purkinje cell axons and consists of the input layer for the cerebellar cortex.[35] The middle layer is predominantly composed of Purkinje and Bergmann cells and performs the function of the output layer.[35] Finally, the outmost layer, the molecular layer, consists of stellate cells, basket cells, granule cells axons and Purkinje cells dendrites.[37] While Purkinje, Golgi, stellate and basket cells tends to be inhibitory, the granule and unipolar brush cells are excitatory.[37]

The highly ramified white matter of the cerebellum resembles a tree in a sagittal section, an association first described by the Danish anatomist Benigmus Winslow in 1740, who named it arbor vitae (Latin for “tree of life”) ([Figure 3]). This structure is embedded by three pairs of deep cerebellar nuclei: fastigial, interposed (consisting of globose and emboliform nuclei) and dentate nuclei, the largest one ([Figure 4]).[35] All outputs from the cerebellum originate from those nuclei.[38]


The cerebellar peduncles play a major role connecting the cerebellum to other organs. Afferent pathways to the cerebellum are primarily transmitted through the inferior and middle cerebellar peduncles, while efferent pathways are conveyed through the superior cerebellar peduncle ([Figure 5]).[39] [40] Regarding the afferent input, the mossy and climbing fibers constitute the majority of cerebellar input. The former originate from pontine nuclei, spinal cord, brainstem reticular formation and vestibular nuclei and the latter originates exclusively in the inferior olive, both making excitatory projections. On the other hand, Purkinje cells are the sole source of output from the cerebellar cortex.[35] [36] [38] [40]

Functionally, the cerebellum can be divided in cerebro-, spino-, and vestibulocerebellum. The cerebrocerebellum is the largest division consisting mainly of lateral portions of the cerebellar hemispheres. It receives input from the cerebral cortex information via pontine nuclei and sends it to the thalamus and red nucleus. The spinocerebellum is formed by the anterior lobe, vermis and fastigial and interposed nuclei. It receives proprioceptive information from the dorsal column of the spinal cord and sends processed information back to adjust fine-tune movements. The vestibulocerebellum includes the flocculonodular lobe and paravermis. It receives inputs from vestibular nuclei and sends that information to both vestibular nuclei and the spinal cord to maintain trunk stability and balance.[35] [36] [37] [38] [40]
MACROANATOMY OF THE CEREBELLUM
The macroscopic organization of the cerebellum is essential for its proper function. In that sense, knowledge of its basic anatomy is of utmost importance to the practicing neurologist.
The cerebellum is located posterior to the brainstem and the fourth ventricle and is separated from the cerebrum by the tentorium ([Figure 3]). Macroscopically, it can be divided into two hemispheres with a midline vermis ([Figure 4]). Superficially, it presents several thin transverse folds named folia.[35] Each hemisphere can be divided into three lobes by two transverse fissures. The primary fissure separates the anterior from the posterior lobes, whereas the posterolateral fissure separates the posterior and flocculonodular lobes.[35] The cerebellum can be further divided by several fissures into 10 lobules using the Schmahmann classification.[41] [42] Particularly, this classification arranges the lobules in numerical order, from I to X, radially in the sagittal plane.[41] For each lobule there is a central portion, in the vermis, and two lateral portions, in each hemisphere.[35]
There are three pairs of white matter tracts that connect the cerebellum to the brainstem.[35] These structures, named cerebellar peduncles, contain cerebellar afferent and efferent tracts.[43] The middle cerebellar peduncle is composed mostly of pontocerebellar fibers that connect the contralateral pontine nuclei to cerebellar structures.[44] Medially to the middle cerebellar peduncle is the inferior cerebellar peduncle which contains afferent and efferent fibers.[35] As for the superior cerebellar peduncles, it is mainly composed of efferent pathways which originate from the dentate, interposed and fastigial nucleus, but also receives input from the ventral spinocerebellar tract.[45]
CLINICAL CORRELATES OF THE CEREBELLUM ANATOMY
Regarding function, the cerebellum has roles associated with motor functions, language, working memory, executive function, autonomic function and affect.[42] The basic knowledge of the cerebellar anatomy and function allow for an adequate understanding of its lesions and associated clinical manifestations. In that sense, a hallmark of cerebellar lesions are the movement alterations, which include dysmetria, dysdiachokinesia, postural and kinetic tremor as well as decomposition of movement.[46] Specifically, action tremor is usually associated with ipsilateral anterior lobe alterations, whereas hypermetria and decomposition of multi-joint movements are frequently associated with alterations in the dentate nucleus.[46] Moreover, it is possible to notice a somatotopy of the superior cerebellar cortex in the sense that upper limb ataxia is associated with lesions of the lobules IV, V, and VI while lower limb ataxia is associated with lesions in lobule III and IV.[46] Furthermore, the Guillain-Mollaret triangle, which is composed of the dentate-rubro-olivary pathway has an important role in the genesis of various types of tremors.[46]
Particularly, concerning motor function, a complex circuitry is related to optimal movement execution. In that sense the cerebellum receives the motor planning and sensory proprioceptive information from its afferent pathways. This enables the cerebellum to compare the intended movement with what is being actually executed and perform the necessary corrections through its polysynaptic connections to the motor cortex.[47] The cerebellar areas involved in this complex movement orchestration, identified with functional magnetic resonance imaging in humans, include lobules I to VI and VIII.[47]
Still considering movement and coordination alterations, it is important to mention the cerebellar homunculus ([Figure 6]). Specifically, the cerebellum displays a particular somatotopic organization, similar to that of the motor and sensory cerebral cortices.[48] Furthermore, this somatotopic organization can be found clearly in the anterior lobe and, less evidently, in the posterior lobe.[48] [49] In that sense, in the anterior lobe, it is possible to notice a clear anterior-to-posterior somatotopic organization going from representation of the feet to the hands and the head.[48] [50] On the other hand, on the posterior lobe, several representations of body parts can be identified; however, the general organization varies between patients and studies.[48] [49] Furthermore, there is evidence that the anterior somatotopic map responds to both ipsilateral and contralateral activity, whereas the anterior representation responds only to ipsilateral movement. In general, the presence of a cerebellar homunculus further highlights the importance of the clinic-anatomic relations.

Other classic alterations of cerebellar function are related to gait and posture. In that sense, patients with cerebellar lesions might present with broad-based stance and gait, as well as difficult standing up.[46] Alterations in gait can be seen in alterations of the fastigial and interposed nuclei. In that sense, previous studies have identified a correlation between posture/gait scores and medial/intermedial cerebellar volume.[51] Furthermore, lesions in the posterior paravermis, nodulus and culmen can present with lateropulsion. Another manifestation of cerebellar dysfunction include decomposition. It is frequently associated with dentate nuclei lesion, which also present with hypermetria as well as lateral and intermediate parts of the cerebellum.[46]
Moreover, the alterations of ocular movements that are associated with cerebellar lesion encompass instability of gaze and nystagmus, hypermetria/hypometria of saccades, saccadic pursuit, skew deviation and disorders of vestibulo-ocular reflex as well as optokinetic responses.[46] The cerebellar structures which are necessary for adequate ocular movements include the lobules VI, VII, crus I and II of ansiform lobule, flocculus, paraflocculus, uvula and nodulus. Particularly, a nucleus of great importance for oculomotor function is the fastigial nucleus, which is important for head orientation, eye-head gaze shifts, saccades and smooth pursuit.[46] Previous studies have identified that reactive oculomotor functions are mostly related to medial cerebellar lesions, whereas voluntary action is affected in lateral lesions.[46]
Cerebellar lesions can also lead to speech alterations.[46] In that sense, in patients presenting with speech deficits due to cerebellar alterations, damage of the paravermal region, hemispheric lobules I and VI and dentate nucleus are commonly identified.[46] Previous research indicated that lesions on the left cerebellum would be more associated with language alterations; however, recent findings show that lesions of both sides may cause speech alterations.[46] Moreover, two networks seem to be associated with speech control:
-
the sensory motor cortex, the basal ganglia, thalamus and inferior cerebellum and;
-
the supplementary motor area, the dorsolateral frontal cortex, the anterior insula and the superior cerebellum.[52]
It is also important to notice that there is plentiful evidence pointing to the importance of the cerebellum in cognition.[53] The range of cognitive skills in which the cerebellum seems to play a role include verb generation, verbal working memory, verbal fluency, visuospatial tasks, executive functions, emotion, pain and addiction.[46] [54] [55] However, clinical signs of cognitive dysfunction associated with cerebellar lesion are usually subtle and mostly noticeable in acute settings or congenital disorders.[46] Regarding topography, previous studies have identified that right posterolateral cerebellar hemispheric lesions are associated with dysfunctions in verbal fluency, that paravermal lesions are associated with lower performance in total aphasia score and that bigger cerebellar lesions are associated with worse reading function when compared to smaller focal lesions.[55] [56] Moreover, extensive vermal damage has been associated with affective symptoms and personality changes, which include anxiety, aggression as well as hyperspontaneous and disinhibited behavior.[46] [56] [57] [58] In that sense, affective symptoms and personality changes are observed after vermal damage in children being subjected to cerebellar tumor resection. The vermis is connected to the limbic system, and its stimulation might modulate amygdala activity, which would suggest a pathway associated with emotional responsiveness.[46]
VASCULAR ANATOMY OF THE CEREBELLUM
Regarding the arterial supply of the cerebellum, there are three main arteries: the superior cerebellar artery (SCA), the anterior inferior cerebellar artery (AICA) and the posterior inferior cerebellar artery (PICA) ([Figure 7]). With regards to the SCA, it is the most constant of the cerebellar arteries and usually arises from the basilar artery or the first segment of the posterior cerebral artery.[59] The SCA usually supplies the rostral portion of the cerebellar hemispheres and vermis, as well as part of the white matter and dentate nucleus, as well as some portions of the brainstem ([Figure 8]).[60] Patients presenting with SCA infarct can be divided into two groups. In the first one, patients present with unilateral ataxia and brainstem dysfunction due to proximal SCA occlusion whereas, in the second, patients present exclusively with cerebellar signs, due to distal occlusion of the vessel.[61] In general, most common symptoms associated with SCA infarction include vertigo (60%), dysarthria (55%), nystagmus (50%), limb ataxia (48%), gait ataxia (45%) and dysmetria (43%).[62] Particularly, dysarthria is frequently associated with signs of infarction of the medial branch of the superior cerebellar artery.[46]

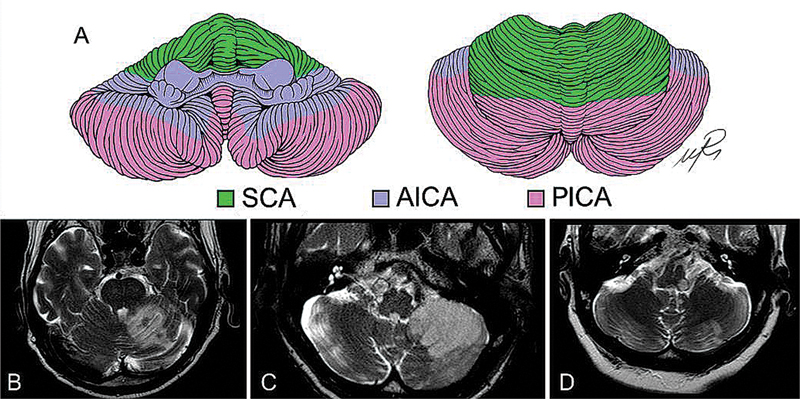
As for the AICA, it frequently arises from the lower third of the basilar trunk.[59] It is responsible for the irrigation of the anteroinferior region of the cerebellum, which includes the flocculus ([Figure 8]). It also supplies the middle cerebellar peduncle, the lateral portion of the pons and the inner ear.[60] However, it is important to notice there is important interpatient variability regarding the territory of the AICA.[59] Most common symptoms associated with AICA ischemia include vertigo, impaired hearing, gait ataxia, limb ataxia, nystagmus, diplopia and peripheral nerve palsy.[63] [64]
With regards to the PICA, it usually emerges from the vertebral arteries.[59] However, it can arise from a common trunk with the AICA from the basilar artery, from the extradural vertebral artery, from the ascending pharyngeal artery or from other origins.[59] As for the territory of irrigation of the PICA, it involves the caudal part of the cerebellar hemispheres and vermis ([Figure 8]).[65] It is also responsible for the irrigation of the dorsolateral region of the medulla oblongata.[60] It is important to notice that there is a reciprocal relation between the territories of the PICA and AICA.[60] In that sense, if the PICA is hypoplastic, the AICA assumes a larger territory.[60] Infarcts of the PICA usually manifest with vertigo, trunk and limb ataxia, nystagmus, dysmetria, and lateropulsion.[60] Particularly, PICA ischemia is usually more correlated with oculomotor signs than other cerebellar arteries infarction.[46] A classical manifestation of PICA ischemia is the lateral medullary syndrome, also known as Wallenberg syndrome.[66] Manifestation might include vertigo with nystagmus, nausea, vomiting, dysphagia, dysphonia, dysarthria, hiccup, ipsilateral ataxia, ipsilateral Horner syndrome, and impairment of pain and thermal sensation on the ipsilateral face and contralateral body.[66]
With regards to the venous drainage of the cerebellum, that are the groups of veins: the anterior, the posterior, and the superior.[67] [68] [69] The anterior, or petrous, group drains the anterior portion of the cerebellum into the superior and inferior petrous sinus. It consists of the anterior pontomesencefalic vein, the petrosal vein and the lateral mesencephalic vein.[69] The posterior group, also known as the tentorial group, includes the veins draining to the tentorium and is composed by the inferior vermian veins and its tributaries.[69] Finally, the superior, or vein of Galen, group drains the upper part of the cerebellar hemispheres, vermis and midbrain to the vein of Galen and the straight sinus.[69] These group consist of precentral cerebellar, superior vermian, and posterior mesencephalic vein.[69]
RADIOLOGICAL ASPECTS OF THE CEREBELLUM
Neuroimaging plays a pivotal part in the evaluation of the cerebellum and its associated pathologies, offering critical insights for the diagnosis, prognosis and understanding of clinical manifestation in cerebellar disorders.
Traditional imaging modalities such as prenatal and postnatal ultrasound, as well as MRI, are particularly effective in detecting early developmental anomalies, such as cerebellar hypoplasia, and malformations, including Dandy-Walker syndrome and Arnold-Chiari malformation.[70] Conventional MRI sequences—such as T1, T2, fluid-attenuated inversion recovery (FLAIR), short Tau inversion recovery (STIR), diffusion, susceptibility-weighted imaging (SWI), and magnetic resonance (MR) angiography—are effective not only for delineating the topography of cerebellar deficits but also for suggesting the underlying etiology, which may include degenerative, inflammatory, infectious, or metabolic causes.[70] [71]
Magnetic resonance imaging is highly useful in identifying focal cerebellar lesions (e.g., infarcts, tumor, demyelinating plaques), cerebellar atrophy patterns and metabolic disorders that preferentially affect the cerebellum. Regarding radiological-clinical correlation, for example, imaging that reveals anterior lobe atrophy can correlate with gait ataxia and lower limbs disfunction, whereas lesions in lobules VI and VII may be associate with oculomotor impairment and cognitive dysfunction.[72]
Moreover, functional imaging techniques, including single-photon emission CT (SPECT), positron emission tomography (PET), and functional MRI (fMRI), are enhancing our understanding of the complex cerebellar circuitry. These advances have been particularly useful in studying conditions such as the cerebellar cognitive affective syndrome.[73]
Considering that fMRI can be used to evaluate cerebellar activation patterns during motor, cognitive, or emotional task, studies have demonstrated that lobules VI, crus I and crus II are directly involved in cognitive functions such as working memory and language. Furthermore, resting-state fMRI has underscored cerebellar involvement in complex brain networks, including the default mode network and salience network, as well as its functional connectivity with the prefrontal cortex, parietal cortex and limbic system.[72]
On the other hand, PET and SPECT have been used to investigate cerebellar perfusion and metabolic activity in degenerative ataxias, cerebellar cognitive affective syndrome and cognitive-psychiatric disorders. For instance, hypometabolism in the posterior cerebellar hemisphere may be associated to language deficit and executive dysfunction.[74]
In conclusion, as a central hub for integrating sensory and motor information, the cerebellum is a structure that plays a central role in coordinating movement, maintaining postural stability, and supporting cognitive functions. Its intricate development from the embryonic stage, as well as its complex microanatomy, circuitry, microanatomy, and vascular supply highlight the importance of the continuous study of these subjects.
Moreover, a full comprehension of this remarkable structure is essential for adequate understanding of the diseases associated with its dysfunction and the profound clinical manifestations associated with it.
Conflict of Interest
The authors have no conflict of interest to declare.
Authors' Contributions
Conceptualization: JVGT, RPCH, FMRF, OGPB, JLP; Data curation: JVGT, RPCH, FMRF, OGPB, JLP; Formal analysis: JVGT, RPCH, FMRF, OGPB, JLP; Funding acquisition: JVGT, RPCH, FMRF, OGPB, JLP; Investigation: JVGT, RPCH, FMRF, OGPB, JLP; Methodology: JVGT, RPCH, FMRF, OGPB, JLP; Project administration: JVGT, RPCH, FMRF, OGPB, JLP; Resources: JVGT, RPCH, FMRF, OGPB, JLP; Software: JVGT, RPCH, FMRF, OGPB, JLP; Supervision: JVGT, RPCH, FMRF, OGPB, JLP; Validation: JVGT, RPCH, FMRF, OGPB, JLP; Visualization: JVGT, RPCH, FMRF, OGPB, JLP;Writing – original draft: JVGT, RPCH, LGBS, LFMB, FR, LAC, VRP, FCN, FMRF, OGPB, JLP;Writing – review & editing: JVGT, RPCH, LGBS, VRP, FCN, FMRF, OGPB, JLP. These authors contributed equally to this article: JVG, RPCH.
Data Availability Statement
Data will be available upon request to the corresponding author.
Editor-in-Chief: Hélio A. G. Teive. (https://orcid.org/0000-0003-2305-1073).
Associate Editor: Mariana Spitz. (https://orcid.org/0000-0001-7548-2313).
-
References
- 1 Singh R, Singh R. Cerebellum: Its Anatomy, Functions and Diseases. In: Tunalı NE. editor. Neurodegenerative Diseases - Molecular Mechanisms and Current Therapeutic Approaches. London: IntechOpen; 2020. ; Available from: https://www.intechopen.com/chapters/72599
- 2 Stoodley CJ. The Cerebellum and Neurodevelopmental Disorders. Cerebellum 2016; 15 (01) 34-37
- 3 Houk JC, Miller LE. Cerebellum: Movement Regulation and Cognitive Functions. In: Encyclopedia of Life Sciences. Hoboken, NJ: John Wiley & Sons, Ltd; 2003.
- 4 Hibi M, Shimizu T. Development of the cerebellum and cerebellar neural circuits. Dev Neurobiol 2012; 72 (03) 282-301
- 5 Jernigan TL, Stiles J. Construction of the human forebrain. Wiley Interdiscip Rev Cogn Sci 2017; 8 (1-2):10.1002/wcs.1409
- 6 Hashimoto M, Hibi M. Development and evolution of cerebellar neural circuits. Dev Growth Differ 2012; 54 (03) 373-389
- 7 Martinez S, Andreu A, Mecklenburg N, Echevarria D. Cellular and molecular basis of cerebellar development. Front Neuroanat 2013; 7: 18
- 8 Wu SR, Butts JC, Caudill MS. et al. Atoh1 drives the heterogeneity of the pontine nuclei neurons and promotes their differentiation. Sci Adv 2023; 9 (26) eadg1671
- 9 Huang X, Liu J, Ketova T. et al. Transventricular delivery of Sonic hedgehog is essential to cerebellar ventricular zone development. Proc Natl Acad Sci U S A 2010; 107 (18) 8422-8427
- 10 Hoshino M, Nakamura S, Mori K. et al. Ptf1a, a bHLH transcriptional gene, defines GABAergic neuronal fates in cerebellum. Neuron 2005; 47 (02) 201-213
- 11 Leto K, Arancillo M, Becker EBE. et al. Consensus Paper: Cerebellar Development. Cerebellum 2016; 15 (06) 789-828
- 12 Chizhikov VV. Roof plate in cerebellar neurogenesis. In: Manto M, Schmahmann JD, Rossi F, Gruol DL, Koibuchi N. editors. Handbook of the Cerebellum and Cerebellar Disorders. Dordrecht: Springer; 2013: 61-74
- 13 Santoro M, Coi A, Barišić I. et al. Epidemiology of Dandy-Walker Malformation in Europe: A EUROCAT Population-Based Registry Study. Neuroepidemiology 2019; 53 (3-4): 169-179
- 14 Parisi MA, Dobyns WB. Human malformations of the midbrain and hindbrain: review and proposed classification scheme. Mol Genet Metab 2003; 80 (1-2): 36-53
- 15 Ocampo-Navia MI, Perez-Mendez W, Rodriguez-Alvarez MP, Chadid-Contreras J, Vergara MF. Dandy-Walker syndrome: an updated literature review. Childs Nerv Syst 2025; 41 (01) 194
- 16 Osenbach RK, Menezes AH. Diagnosis and management of the Dandy-Walker malformation: 30 years of experience. Pediatr Neurosurg 1992; 18 (04) 179-189
- 17 Sun Y, Wang T, Zhang N, Zhang P, Li Y. Clinical features and genetic analysis of Dandy-Walker syndrome. BMC Pregnancy Childbirth 2023; 23 (01) 40
- 18 Grinberg I, Northrup H, Ardinger H, Prasad C, Dobyns WB, Millen KJ. Heterozygous deletion of the linked genes ZIC1 and ZIC4 is involved in Dandy-Walker malformation. Nat Genet 2004; 36 (10) 1053-1055
- 19 Aldinger KA, Lehmann OJ, Hudgins L. et al. FOXC1 is required for normal cerebellar development and is a major contributor to chromosome 6p25.3 Dandy-Walker malformation. Nat Genet 2009; 41 (09) 1037-1042
- 20 Limperopoulos C, Folkerth R, Barnewolt CE, Connolly S, Du Plessis AJ. Posthemorrhagic cerebellar disruption mimicking Dandy-Walker malformation: fetal imaging and neuropathology findings. Semin Pediatr Neurol 2010; 17 (01) 75-81
- 21 Haldipur P, Gillies GS, Janson OK. et al. Foxc1 dependent mesenchymal signalling drives embryonic cerebellar growth. eLife 2014; 3 •••
- 22 Parisi MA, Doherty D, Chance PF, Glass IA. Joubert syndrome (and related disorders) (OMIM 213300). Eur J Hum Genet 2007; 15 (05) 511-521
- 23 Maria BL, Quisling RG, Rosainz LC. et al. Molar tooth sign in Joubert syndrome: clinical, radiologic, and pathologic significance. J Child Neurol 1999; 14 (06) 368-376
- 24 Brancati F, Dallapiccola B, Valente EM. Joubert Syndrome and related disorders. Orphanet J Rare Dis 2010; 5 (01) 20
- 25 Dong Y, Zhang K, Yao H. et al. Clinical and genetic characteristics of 36 children with Joubert syndrome. Front Pediatr 2023; 11: 1102639
- 26 Romani M, Micalizzi A, Valente EM. Joubert syndrome: congenital cerebellar ataxia with the molar tooth. Lancet Neurol 2013; 12 (09) 894-905
- 27 Aguilar A, Meunier A, Strehl L. et al. Analysis of human samples reveals impaired SHH-dependent cerebellar development in Joubert syndrome/Meckel syndrome. Proc Natl Acad Sci U S A 2012; 109 (42) 16951-16956
- 28 Spassky N, Han YG, Aguilar A. et al. Primary cilia are required for cerebellar development and Shh-dependent expansion of progenitor pool. Dev Biol 2008; 317 (01) 246-259
- 29 Köster RW, Fraser SE. Direct imaging of in vivo neuronal migration in the developing cerebellum. Curr Biol 2001; 11 (23) 1858-1863
- 30 Wingate RJT, Hatten ME. The role of the rhombic lip in avian cerebellum development. Development 1999; 126 (20) 4395-4404
- 31 Wassmer E, Davies P, Whitehouse WP, Green SH. Clinical spectrum associated with cerebellar hypoplasia. Pediatr Neurol 2003; 28 (05) 347-351
- 32 Timmann D, Dimitrova A, Hein-Kropp C, Wilhelm H, Dörfler A. Cerebellar agenesis: clinical, neuropsychological and MR findings. Neurocase 2003; 9 (05) 402-413
- 33 Bouanani Z, Rhalem I, Lahnine G. et al. Total cerebellar agenesis: A case report of a very rare condition. Radiol Case Rep 2024; 19 (10) 4569-4571
- 34 Sellick GS, Barker KT, Stolte-Dijkstra I. et al. Mutations in PTF1A cause pancreatic and cerebellar agenesis. Nat Genet 2004; 36 (12) 1301-1305
- 35 Roostaei T, Nazeri A, Sahraian MA, Minagar A. The human cerebellum: a review of physiologic neuroanatomy. Neurol Clin 2014; 32 (04) 859-869
- 36 Van Essen DC, Donahue CJ, Glasser MF. Development and Evolution of Cerebral and Cerebellar Cortex. Brain Behav Evol 2018; 91 (03) 158-169
- 37 Consalez GG, Goldowitz D, Casoni F, Hawkes R. Origins, Development, and Compartmentation of the Granule Cells of the Cerebellum. Front Neural Circuits 2021; 14: 611841
- 38 Purves D, Augustine GJ, Fitzpatrick D. et al. Organization of the Cerebellum. In: ______, editors. Neuroscience. 2nd edition.. Sunderland, MA: Sinauer Associates; 2001. . Available from: https://www.ncbi.nlm.nih.gov/books/NBK11132/
- 39 Splittgerber R. Snell's Clinical Neuroanatomy. 8th edition.. Philadelphia: LWW; 2018
- 40 Perrini P, Tiezzi G, Castagna M, Vannozzi R. Three-dimensional microsurgical anatomy of cerebellar peduncles. Neurosurg Rev 2013; 36 (02) 215-224 , discussion 224–225
- 41 Schmahmann JD, Doyon J, McDonald D. et al. Three-dimensional MRI atlas of the human cerebellum in proportional stereotaxic space. Neuroimage 1999; 10 (3 Pt 1): 233-260
- 42 Lehman VT, Black DF, DeLone DR. et al. Current concepts of cross-sectional and functional anatomy of the cerebellum: a pictorial review and atlas. Br J Radiol 2020; 93 (1106) 20190467
- 43 Ahumada-Vizcaino JC, Wuo-Silva R, Hernández MM, Chaddad-Neto F. The art of combining neuroanatomy and microsurgical skills in modern neurosurgery. Front Neurol 2023; 13: 1076778
- 44 Tamanini JVG, Ribeiro GAS, Kimura AT, Borella LF, Freddi TA, Reis F. Hyperintense lesions of the middle cerebellar peduncle and beyond: a pictorial essay. Radiol Bras 2025; 57: e20240001
- 45 Dekeyzer S, Vanden Bossche S, De Cocker L. Anything but Little: a Pictorial Review on Anatomy and Pathology of the Cerebellum. Clin Neuroradiol 2023; 33 (04) 907-929
- 46 Grimaldi G, Manto M. Topography of cerebellar deficits in humans. Cerebellum 2012; 11 (02) 336-351
- 47 Prati JM, Pontes-Silva A, Gianlorenço ACL. The cerebellum and its connections to other brain structures involved in motor and non-motor functions: A comprehensive review. Behav Brain Res 2024; 465: 114933
- 48 Boillat Y, Bazin PL, Van der Zwaag W. Whole-body somatotopic maps in the cerebellum revealed with 7T fMRI. Neuroimage 2020; 211: 116624
- 49 Batson MA, Petridou N, Klomp DWJ, Frens MA, Neggers SFW. Single session imaging of cerebellum at 7 Tesla: obtaining structure and function of multiple motor subsystems in individual subjects. PLoS One 2015; 10 (08) e0134933
- 50 Schlerf JE, Verstynen TD, Ivry RB, Spencer RMC. Evidence of a novel somatopic map in the human neocerebellum during complex actions. J Neurophysiol 2010; 103 (06) 3330-3336
- 51 Timmann D, Konczak J, Ilg W. et al. Current advances in lesion-symptom mapping of the human cerebellum. Neuroscience 2009; 162 (03) 836-851
- 52 Riecker A, Mathiak K, Wildgruber D. et al. fMRI reveals two distinct cerebral networks subserving speech motor control. Neurology 2005; 64 (04) 700-706
- 53 Leiner HC, Leiner AL, Dow RS. Does the cerebellum contribute to mental skills?. Behav Neurosci 1986; 100 (04) 443-454
- 54 Strick PL, Dum RP, Fiez JA. Cerebellum and nonmotor function. Annu Rev Neurosci 2009; 32: 413-434
- 55 Richter S, Gerwig M, Aslan B. et al. Cognitive functions in patients with MR-defined chronic focal cerebellar lesions. J Neurol 2007; 254 (09) 1193-1203
- 56 Karaci R, Oztürk S, Özbakir S, Cansaran N. Evaluation of language functions in acute cerebellar vascular diseases. J Stroke Cerebrovasc Dis 2008; 17 (05) 251-256
- 57 Riva D, Giorgi C. The cerebellum contributes to higher functions during development: evidence from a series of children surgically treated for posterior fossa tumours. Brain 2000; 123 (Pt 5): 1051-1061
- 58 Levisohn L, Cronin-Golomb A, Schmahmann JD. Neuropsychological consequences of cerebellar tumour resection in children: cerebellar cognitive affective syndrome in a paediatric population. Brain 2000; 123 (Pt 5): 1041-1050
- 59 Delion M, Dinomais M, Mercier P. Arteries and Veins of the Cerebellum. Cerebellum 2017; 16 (5-6): 880-912
- 60 Barth A, Bogousslavsky J, Regli F. The clinical and topographic spectrum of cerebellar infarcts: a clinical-magnetic resonance imaging correlation study. Ann Neurol 1993; 33 (05) 451-456
- 61 Terao S, Sobue G, Izumi M, Miura N, Takeda A, Mitsuma T. Infarction of superior cerebellar artery presenting as cerebellar symptoms. Stroke 1996; 27 (09) 1679-1681
- 62 Kumral E, Kisabay A, Ataç C. Lesion patterns and etiology of ischemia in superior cerebellar artery territory infarcts. Cerebrovasc Dis 2005; 19 (05) 283-290
- 63 Ogawa K, Suzuki Y, Takahashi K, Akimoto T, Kamei S, Soma M. Clinical Study of Seven Patients with Infarction in Territories of the Anterior Inferior Cerebellar Artery. J Stroke Cerebrovasc Dis 2017; 26 (03) 574-581
- 64 Roquer J, Lorenzo JL, Pou A. The anterior inferior cerebellar artery infarcts: a clinical-magnetic resonance imaging study. Acta Neurol Scand 1998; 97 (04) 225-230
- 65 Hartkamp NS, De Cocker LJ, Helle M. et al. In vivo visualization of the PICA perfusion territory with super-selective pseudo-continuous arterial spin labeling MRI. Neuroimage 2013; 83: 58-65
- 66 Miao HL, Zhang DY, Wang T, Jiao XT, Jiao LQ. Clinical Importance of the Posterior Inferior Cerebellar Artery: A Review of the Literature. Int J Med Sci 2020; 17 (18) 3005-3019
- 67 Ota T. Functional Cerebral Venous Anatomy: A Perspective on Venous Collaterals Part II, Infratentorial Venous System. Stroke Vasc Intervent Neurol 2024; 4 (02) e001060
- 68 De Miquel MA. Posterior Fossa Venous Drainage. Front Neurol 2021; 12: 680515
- 69 Harrigan MR, Deveikis JP. Handbook of Cerebrovascular Disease and Neurointerventional Technique. 4th edition.. Totowa, NJ: Humana Press; 2023.
- 70 Rapalino O. Radiographic Features of Cerebellar Disease: Imaging Approach to Differential Diagnosis. In: Manto MU, Gruol DL, Schmahmann JD, Koibuchi N, Sillitoe RV. editors. Handbook of the Cerebellum and Cerebellar Disorders. 2nd edition.. Cham, Switzerland: Springer; 2022: V.3:721-37
- 71 Currie S, Hadjivassiliou M, Craven IJ, Wilkinson ID, Griffiths PD, Hoggard N. Magnetic resonance imaging biomarkers in patients with progressive ataxia: current status and future direction. Cerebellum 2013; 12 (02) 245-266
- 72 Stoodley CJ, Schmahmann JD. Functional topography in the human cerebellum: a meta-analysis of neuroimaging studies. Neuroimage 2009; 44 (02) 489-501
- 73 Timmann D, Daum I. Cerebellar contributions to cognitive functions: a progress report after two decades of research. Cerebellum 2007; 6 (03) 159-162
- 74 Schmahmann JD, Sherman JC. The cerebellar cognitive affective syndrome. Brain 1998; 121 (Pt 4): 561-579
Address for correspondence
Publication History
Received: 15 May 2025
Accepted: 03 October 2025
Article published online:
22 December 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution 4.0 International License, permitting copying and reproduction so long as the original work is given appropriate credit (https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda.
Rua Rego Freitas, 175, loja 1, República, São Paulo, SP, CEP 01220-010, Brazil
João Vitor Gerdulli Tamanini, Raphael Pinheiro Camurugy da Hora, Luís Gustavo Biondi Soares, Luiz Fernando Monte Borella, Fabiano Reis, Luis Ángel Canache, Victor Rebelo Procaci, Feres Chaddad-Neto, Flávio Moura de Rezende Filho, Orlando Graziani Povoas Barsottini, José Luiz Pedroso. A journey through the anatomy of the cerebellum. Arq Neuropsiquiatr 2025; 83: s00451814379.
DOI: 10.1055/s-0045-1814379
-
References
- 1 Singh R, Singh R. Cerebellum: Its Anatomy, Functions and Diseases. In: Tunalı NE. editor. Neurodegenerative Diseases - Molecular Mechanisms and Current Therapeutic Approaches. London: IntechOpen; 2020. ; Available from: https://www.intechopen.com/chapters/72599
- 2 Stoodley CJ. The Cerebellum and Neurodevelopmental Disorders. Cerebellum 2016; 15 (01) 34-37
- 3 Houk JC, Miller LE. Cerebellum: Movement Regulation and Cognitive Functions. In: Encyclopedia of Life Sciences. Hoboken, NJ: John Wiley & Sons, Ltd; 2003.
- 4 Hibi M, Shimizu T. Development of the cerebellum and cerebellar neural circuits. Dev Neurobiol 2012; 72 (03) 282-301
- 5 Jernigan TL, Stiles J. Construction of the human forebrain. Wiley Interdiscip Rev Cogn Sci 2017; 8 (1-2):10.1002/wcs.1409
- 6 Hashimoto M, Hibi M. Development and evolution of cerebellar neural circuits. Dev Growth Differ 2012; 54 (03) 373-389
- 7 Martinez S, Andreu A, Mecklenburg N, Echevarria D. Cellular and molecular basis of cerebellar development. Front Neuroanat 2013; 7: 18
- 8 Wu SR, Butts JC, Caudill MS. et al. Atoh1 drives the heterogeneity of the pontine nuclei neurons and promotes their differentiation. Sci Adv 2023; 9 (26) eadg1671
- 9 Huang X, Liu J, Ketova T. et al. Transventricular delivery of Sonic hedgehog is essential to cerebellar ventricular zone development. Proc Natl Acad Sci U S A 2010; 107 (18) 8422-8427
- 10 Hoshino M, Nakamura S, Mori K. et al. Ptf1a, a bHLH transcriptional gene, defines GABAergic neuronal fates in cerebellum. Neuron 2005; 47 (02) 201-213
- 11 Leto K, Arancillo M, Becker EBE. et al. Consensus Paper: Cerebellar Development. Cerebellum 2016; 15 (06) 789-828
- 12 Chizhikov VV. Roof plate in cerebellar neurogenesis. In: Manto M, Schmahmann JD, Rossi F, Gruol DL, Koibuchi N. editors. Handbook of the Cerebellum and Cerebellar Disorders. Dordrecht: Springer; 2013: 61-74
- 13 Santoro M, Coi A, Barišić I. et al. Epidemiology of Dandy-Walker Malformation in Europe: A EUROCAT Population-Based Registry Study. Neuroepidemiology 2019; 53 (3-4): 169-179
- 14 Parisi MA, Dobyns WB. Human malformations of the midbrain and hindbrain: review and proposed classification scheme. Mol Genet Metab 2003; 80 (1-2): 36-53
- 15 Ocampo-Navia MI, Perez-Mendez W, Rodriguez-Alvarez MP, Chadid-Contreras J, Vergara MF. Dandy-Walker syndrome: an updated literature review. Childs Nerv Syst 2025; 41 (01) 194
- 16 Osenbach RK, Menezes AH. Diagnosis and management of the Dandy-Walker malformation: 30 years of experience. Pediatr Neurosurg 1992; 18 (04) 179-189
- 17 Sun Y, Wang T, Zhang N, Zhang P, Li Y. Clinical features and genetic analysis of Dandy-Walker syndrome. BMC Pregnancy Childbirth 2023; 23 (01) 40
- 18 Grinberg I, Northrup H, Ardinger H, Prasad C, Dobyns WB, Millen KJ. Heterozygous deletion of the linked genes ZIC1 and ZIC4 is involved in Dandy-Walker malformation. Nat Genet 2004; 36 (10) 1053-1055
- 19 Aldinger KA, Lehmann OJ, Hudgins L. et al. FOXC1 is required for normal cerebellar development and is a major contributor to chromosome 6p25.3 Dandy-Walker malformation. Nat Genet 2009; 41 (09) 1037-1042
- 20 Limperopoulos C, Folkerth R, Barnewolt CE, Connolly S, Du Plessis AJ. Posthemorrhagic cerebellar disruption mimicking Dandy-Walker malformation: fetal imaging and neuropathology findings. Semin Pediatr Neurol 2010; 17 (01) 75-81
- 21 Haldipur P, Gillies GS, Janson OK. et al. Foxc1 dependent mesenchymal signalling drives embryonic cerebellar growth. eLife 2014; 3 •••
- 22 Parisi MA, Doherty D, Chance PF, Glass IA. Joubert syndrome (and related disorders) (OMIM 213300). Eur J Hum Genet 2007; 15 (05) 511-521
- 23 Maria BL, Quisling RG, Rosainz LC. et al. Molar tooth sign in Joubert syndrome: clinical, radiologic, and pathologic significance. J Child Neurol 1999; 14 (06) 368-376
- 24 Brancati F, Dallapiccola B, Valente EM. Joubert Syndrome and related disorders. Orphanet J Rare Dis 2010; 5 (01) 20
- 25 Dong Y, Zhang K, Yao H. et al. Clinical and genetic characteristics of 36 children with Joubert syndrome. Front Pediatr 2023; 11: 1102639
- 26 Romani M, Micalizzi A, Valente EM. Joubert syndrome: congenital cerebellar ataxia with the molar tooth. Lancet Neurol 2013; 12 (09) 894-905
- 27 Aguilar A, Meunier A, Strehl L. et al. Analysis of human samples reveals impaired SHH-dependent cerebellar development in Joubert syndrome/Meckel syndrome. Proc Natl Acad Sci U S A 2012; 109 (42) 16951-16956
- 28 Spassky N, Han YG, Aguilar A. et al. Primary cilia are required for cerebellar development and Shh-dependent expansion of progenitor pool. Dev Biol 2008; 317 (01) 246-259
- 29 Köster RW, Fraser SE. Direct imaging of in vivo neuronal migration in the developing cerebellum. Curr Biol 2001; 11 (23) 1858-1863
- 30 Wingate RJT, Hatten ME. The role of the rhombic lip in avian cerebellum development. Development 1999; 126 (20) 4395-4404
- 31 Wassmer E, Davies P, Whitehouse WP, Green SH. Clinical spectrum associated with cerebellar hypoplasia. Pediatr Neurol 2003; 28 (05) 347-351
- 32 Timmann D, Dimitrova A, Hein-Kropp C, Wilhelm H, Dörfler A. Cerebellar agenesis: clinical, neuropsychological and MR findings. Neurocase 2003; 9 (05) 402-413
- 33 Bouanani Z, Rhalem I, Lahnine G. et al. Total cerebellar agenesis: A case report of a very rare condition. Radiol Case Rep 2024; 19 (10) 4569-4571
- 34 Sellick GS, Barker KT, Stolte-Dijkstra I. et al. Mutations in PTF1A cause pancreatic and cerebellar agenesis. Nat Genet 2004; 36 (12) 1301-1305
- 35 Roostaei T, Nazeri A, Sahraian MA, Minagar A. The human cerebellum: a review of physiologic neuroanatomy. Neurol Clin 2014; 32 (04) 859-869
- 36 Van Essen DC, Donahue CJ, Glasser MF. Development and Evolution of Cerebral and Cerebellar Cortex. Brain Behav Evol 2018; 91 (03) 158-169
- 37 Consalez GG, Goldowitz D, Casoni F, Hawkes R. Origins, Development, and Compartmentation of the Granule Cells of the Cerebellum. Front Neural Circuits 2021; 14: 611841
- 38 Purves D, Augustine GJ, Fitzpatrick D. et al. Organization of the Cerebellum. In: ______, editors. Neuroscience. 2nd edition.. Sunderland, MA: Sinauer Associates; 2001. . Available from: https://www.ncbi.nlm.nih.gov/books/NBK11132/
- 39 Splittgerber R. Snell's Clinical Neuroanatomy. 8th edition.. Philadelphia: LWW; 2018
- 40 Perrini P, Tiezzi G, Castagna M, Vannozzi R. Three-dimensional microsurgical anatomy of cerebellar peduncles. Neurosurg Rev 2013; 36 (02) 215-224 , discussion 224–225
- 41 Schmahmann JD, Doyon J, McDonald D. et al. Three-dimensional MRI atlas of the human cerebellum in proportional stereotaxic space. Neuroimage 1999; 10 (3 Pt 1): 233-260
- 42 Lehman VT, Black DF, DeLone DR. et al. Current concepts of cross-sectional and functional anatomy of the cerebellum: a pictorial review and atlas. Br J Radiol 2020; 93 (1106) 20190467
- 43 Ahumada-Vizcaino JC, Wuo-Silva R, Hernández MM, Chaddad-Neto F. The art of combining neuroanatomy and microsurgical skills in modern neurosurgery. Front Neurol 2023; 13: 1076778
- 44 Tamanini JVG, Ribeiro GAS, Kimura AT, Borella LF, Freddi TA, Reis F. Hyperintense lesions of the middle cerebellar peduncle and beyond: a pictorial essay. Radiol Bras 2025; 57: e20240001
- 45 Dekeyzer S, Vanden Bossche S, De Cocker L. Anything but Little: a Pictorial Review on Anatomy and Pathology of the Cerebellum. Clin Neuroradiol 2023; 33 (04) 907-929
- 46 Grimaldi G, Manto M. Topography of cerebellar deficits in humans. Cerebellum 2012; 11 (02) 336-351
- 47 Prati JM, Pontes-Silva A, Gianlorenço ACL. The cerebellum and its connections to other brain structures involved in motor and non-motor functions: A comprehensive review. Behav Brain Res 2024; 465: 114933
- 48 Boillat Y, Bazin PL, Van der Zwaag W. Whole-body somatotopic maps in the cerebellum revealed with 7T fMRI. Neuroimage 2020; 211: 116624
- 49 Batson MA, Petridou N, Klomp DWJ, Frens MA, Neggers SFW. Single session imaging of cerebellum at 7 Tesla: obtaining structure and function of multiple motor subsystems in individual subjects. PLoS One 2015; 10 (08) e0134933
- 50 Schlerf JE, Verstynen TD, Ivry RB, Spencer RMC. Evidence of a novel somatopic map in the human neocerebellum during complex actions. J Neurophysiol 2010; 103 (06) 3330-3336
- 51 Timmann D, Konczak J, Ilg W. et al. Current advances in lesion-symptom mapping of the human cerebellum. Neuroscience 2009; 162 (03) 836-851
- 52 Riecker A, Mathiak K, Wildgruber D. et al. fMRI reveals two distinct cerebral networks subserving speech motor control. Neurology 2005; 64 (04) 700-706
- 53 Leiner HC, Leiner AL, Dow RS. Does the cerebellum contribute to mental skills?. Behav Neurosci 1986; 100 (04) 443-454
- 54 Strick PL, Dum RP, Fiez JA. Cerebellum and nonmotor function. Annu Rev Neurosci 2009; 32: 413-434
- 55 Richter S, Gerwig M, Aslan B. et al. Cognitive functions in patients with MR-defined chronic focal cerebellar lesions. J Neurol 2007; 254 (09) 1193-1203
- 56 Karaci R, Oztürk S, Özbakir S, Cansaran N. Evaluation of language functions in acute cerebellar vascular diseases. J Stroke Cerebrovasc Dis 2008; 17 (05) 251-256
- 57 Riva D, Giorgi C. The cerebellum contributes to higher functions during development: evidence from a series of children surgically treated for posterior fossa tumours. Brain 2000; 123 (Pt 5): 1051-1061
- 58 Levisohn L, Cronin-Golomb A, Schmahmann JD. Neuropsychological consequences of cerebellar tumour resection in children: cerebellar cognitive affective syndrome in a paediatric population. Brain 2000; 123 (Pt 5): 1041-1050
- 59 Delion M, Dinomais M, Mercier P. Arteries and Veins of the Cerebellum. Cerebellum 2017; 16 (5-6): 880-912
- 60 Barth A, Bogousslavsky J, Regli F. The clinical and topographic spectrum of cerebellar infarcts: a clinical-magnetic resonance imaging correlation study. Ann Neurol 1993; 33 (05) 451-456
- 61 Terao S, Sobue G, Izumi M, Miura N, Takeda A, Mitsuma T. Infarction of superior cerebellar artery presenting as cerebellar symptoms. Stroke 1996; 27 (09) 1679-1681
- 62 Kumral E, Kisabay A, Ataç C. Lesion patterns and etiology of ischemia in superior cerebellar artery territory infarcts. Cerebrovasc Dis 2005; 19 (05) 283-290
- 63 Ogawa K, Suzuki Y, Takahashi K, Akimoto T, Kamei S, Soma M. Clinical Study of Seven Patients with Infarction in Territories of the Anterior Inferior Cerebellar Artery. J Stroke Cerebrovasc Dis 2017; 26 (03) 574-581
- 64 Roquer J, Lorenzo JL, Pou A. The anterior inferior cerebellar artery infarcts: a clinical-magnetic resonance imaging study. Acta Neurol Scand 1998; 97 (04) 225-230
- 65 Hartkamp NS, De Cocker LJ, Helle M. et al. In vivo visualization of the PICA perfusion territory with super-selective pseudo-continuous arterial spin labeling MRI. Neuroimage 2013; 83: 58-65
- 66 Miao HL, Zhang DY, Wang T, Jiao XT, Jiao LQ. Clinical Importance of the Posterior Inferior Cerebellar Artery: A Review of the Literature. Int J Med Sci 2020; 17 (18) 3005-3019
- 67 Ota T. Functional Cerebral Venous Anatomy: A Perspective on Venous Collaterals Part II, Infratentorial Venous System. Stroke Vasc Intervent Neurol 2024; 4 (02) e001060
- 68 De Miquel MA. Posterior Fossa Venous Drainage. Front Neurol 2021; 12: 680515
- 69 Harrigan MR, Deveikis JP. Handbook of Cerebrovascular Disease and Neurointerventional Technique. 4th edition.. Totowa, NJ: Humana Press; 2023.
- 70 Rapalino O. Radiographic Features of Cerebellar Disease: Imaging Approach to Differential Diagnosis. In: Manto MU, Gruol DL, Schmahmann JD, Koibuchi N, Sillitoe RV. editors. Handbook of the Cerebellum and Cerebellar Disorders. 2nd edition.. Cham, Switzerland: Springer; 2022: V.3:721-37
- 71 Currie S, Hadjivassiliou M, Craven IJ, Wilkinson ID, Griffiths PD, Hoggard N. Magnetic resonance imaging biomarkers in patients with progressive ataxia: current status and future direction. Cerebellum 2013; 12 (02) 245-266
- 72 Stoodley CJ, Schmahmann JD. Functional topography in the human cerebellum: a meta-analysis of neuroimaging studies. Neuroimage 2009; 44 (02) 489-501
- 73 Timmann D, Daum I. Cerebellar contributions to cognitive functions: a progress report after two decades of research. Cerebellum 2007; 6 (03) 159-162
- 74 Schmahmann JD, Sherman JC. The cerebellar cognitive affective syndrome. Brain 1998; 121 (Pt 4): 561-579