

Subscribe to RSS
DOI: 10.1055/s-0045-1814090
Randomized Controlled Trial on the Reduction of Scattered Radiation Exposure to Primary Operator, Secondary Operator, and Primary Technician by Radiation Protection Drape in Cath Lab Procedures
Authors
Funding None.



Abstract
Background
Scattered radiation during cath laboratory procedures poses occupational risks to medical staff, including primary operators, secondary operators, and technicians. It is associated with DNA damage, cataracts, and other complications. Although radiation protection drapes are recommended, their effectiveness across different personnel requires further evaluation.
Objective
This study assessed the efficacy of radiation protection drapes in reducing scattered radiation exposure for cath laboratory staff.
Materials and Methods
A single-center, open-label, parallel-group randomized controlled trial included 216 patients undergoing cath laboratory procedures. Patients were randomized into two groups: one with radiation protection drapes and another with standard radiation protection. Personnel exposure was measured via personal dosimeters attached to chest pockets, evaluating air kerma (AK), dose area product (DAP), and cine-adjusted screen time (CAST).
Results
Radiation protection drapes significantly reduced exposure across all personnel during femoral and radial procedures. Primary operators saw reductions of 63.65% (dose/AK), 51.94% (dose/DAP), and 44.27% (dose/CAST). Secondary operators experienced reductions of 46.54, 36.42, and 35.93%, while technicians recorded reductions of 44.51, 34.26, and 35.61%, respectively. In pectoral procedures, primary and secondary operators benefited, with exposure reductions of up to 62% (dose/AK), 49% (dose/DAP), and 52% (dose/CAST), while no significant reduction was observed for technicians.
Conclusion
Radiation protection drapes effectively reduced scattered radiation exposure for primary and secondary operators, with primary operators benefiting the most.
Keywords
scattered radiation - radiation protection drapes - cath laboratory procedures - randomized controlled trial - occupational exposureIntroduction
The introduction of ionizing radiation in medicine has revolutionized disease diagnosis and treatment, particularly in interventional cardiology, where fluoroscopy-guided procedures are essential for managing cardiovascular diseases.[1] These procedures have greatly enhanced patient care by allowing for more accurate and minimally invasive interventions. However, they also expose healthcare providers and patients to radiation risks, including both deterministic and stochastic effects.[2]
Healthcare personnel in cath laboratories, particularly interventional cardiologists, face higher incidences of radiation-induced health issues such as somatic DNA damage, chromosomal abnormalities, and posterior sub-capsular lens opacities. Notably, disproportionate radiation exposure on the left side of the head has been linked to an elevated risk of cataracts among cath laboratory workers.[3] [4] [5] Even anesthesiologists in cath laboratories experience greater radiation exposure compared with those in operating rooms.[6] Several factors influence radiation exposure in the cath laboratory, including the complexity and length of procedures, patient-specific characteristics, the availability of protective equipment, and the operator's level of experience.[7]
The growing awareness of these risks has led to a stronger emphasis on the “as low as reasonably achievable” (ALARA) principle, which focuses on minimizing radiation exposure while maintaining diagnostic accuracy. Efforts to reduce radiation exposure in the cath laboratory are critical not only for patient safety but also for safeguarding the health of medical personnel.[8] Radiation protection strategies encompass both passive and active elements. Passive components include protective equipment such as radiation protection aprons, thyroid protection collars, glasses, caps, and supplementary devices like mobile acrylic shields and under-table lead curtains. Active processes rely on the effective utilization of these tools.[9] [10] Among these, radiation protection drapes, made from sterile surgical material embedded with radiation-absorbing elements such as bismuth and barium, serve as a crucial barrier against scattered radiation. Positioned strategically between the image intensifier and the operator, these drapes significantly mitigate radiation dispersion.[11]
Despite the availability of radiation protection devices, there is limited literature comparing exposure levels among cath laboratory personnel and evaluating the efficacy of radiation protection drapes in reducing exposure. Moreover, previous studies have reported inconsistent results regarding their effectiveness. This study aims to address these gaps by systematically assessing the role of radiation protection drapes in reducing radiation exposure to primary operators, secondary operators, and technicians during cath laboratory procedures.
Materials and Methods
Study Objectives
This study aimed to assess the relative radiation exposure experienced by different cath laboratory personnel (primary operator, secondary operator, and technician) and evaluate the efficacy of radiation protection drapes in reducing exposure, thereby preventing occupational hazards in interventional cardiology settings.
Study Design
This was a single-center, parallel, open-label randomized controlled trial (RCT) with a 1:1 allocation ratio. The trial was conducted over 18 months, from November 2022 to April 2024, to evaluate the effectiveness of radiation protection drapes in reducing scattered radiation exposure during cardiac catheterization procedures.
Study Participants
Participants included adults aged 18 years or older undergoing catheterization procedures at the study center. Inclusion criteria included patients weighing more than 50 kg. Patients undergoing hybrid therapies or procedures involving multiple sites were excluded. Other exclusion criteria included procedures with multiple primary operators, those lacking a secondary operator, or cases where the secondary operator or technician was changed midway through the procedure. Patients with incomplete procedures for any reason were also excluded.
The study adhered to institutional protocols for radiation protection, including the use of standard personal protective equipment (PPE) such as lead aprons and thyroid shields. Additionally, a ceiling-suspended radiation shield was employed to minimize scatter radiation exposure to operators.
Sample Size Calculation and Randomization
The sample size was calculated based on a prior study by Shah et al[12] with a 95% confidence interval and 80% power; the minimum required sample size was determined to be 28 participants per group. Adjusting for a 10% error rate, the target sample size was increased to 33 participants per group. However, enrolment was extended until 216 patients (108 in each group) were included to ensure robust analysis within the study's timeframe.
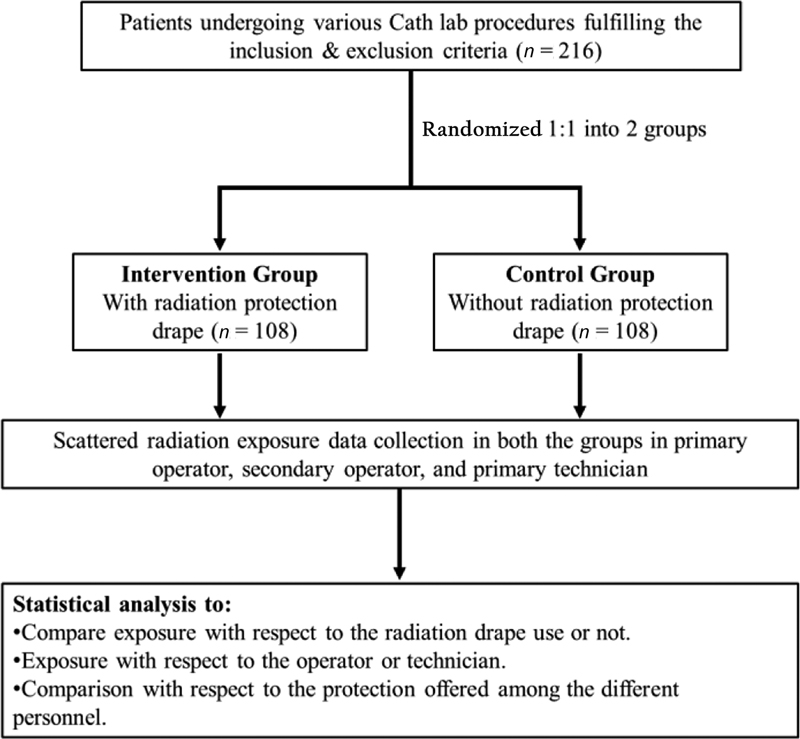
Patients meeting the inclusion and exclusion criteria were randomized into two groups: the intervention group (radiation protection drape) and the control group (standard radiation protection measures without drape) using a computer-based algorithm that assigned participants unique identifiers to ensure unbiased allocation. The randomization process employed a pseudorandom number generator, providing equal chances of assignment to either the intervention or control group. The allocation flow is depicted in [Fig. 1].
Interventions
The intervention group used a radiopaque bismuth radiation protection drape (RADPAD) to attenuate scattered radiation. The drape was positioned strategically depending on the vascular access route. For radial artery access, the drape was placed craniomedially on the patient's forearm near the sheath insertion point. For femoral artery access, it was placed cranially on the groin above the insertion site. In pectoral access procedures, the drape was positioned between the incision site and the operator on the patient's left side. In the control group, standard radiation protection protocols were followed without the use of a radiation protection drape.
Outcome Measures
Radiation exposure was quantified using personal dosimeters (MYDOSE mini PDM127, Hitachi Aloka Medical Ltd., Japan), which were clipped to the chest pockets of the cath laboratory personnel and remained in place for the entire procedure. Radiation parameters recorded included air kerma (AK), dose area product (DAP), and cine-adjusted screen time (CAST). CAST was calculated by multiplying the number of cine acquisitions by 15 (average cine emits 15 times more radiation than fluoroscopy) and then by 4 (average cine duration in seconds). These parameters were used to compare radiation exposure among primary operators, secondary operators, and technicians in both groups.
Statistical Analysis
All statistical analyses were performed using SPSS v.21 (IBM, Chicago, Illinois). Continuous variables were presented as mean ± standard deviation (SD) or as medians if data were unevenly distributed, while categorical variables were expressed as frequencies and percentages. A paired Student's t-test was used to compare continuous variables between the groups, and one-way ANOVA was utilized for comparisons across groups. For non-normally distributed variables, the Mann-Whitney U test was applied. A p-value of <0.05 was considered statistically significant.
Ethical Considerations
Approval for the study was obtained from the Institutional Ethics Committee, and the trial was registered with the Clinical Trials Registry of India (CTRI/2022/11/047008). All participants provided informed consent.
Results
A total of 216 patients were included in this study between November 2022 and April 2024. Participants were randomized in a 1:1 ratio into two groups: one group receiving the radiation protection drape and the other following standard protocols without the drape, with 108 patients in each group. [Table 1] summarizes the demographic characteristics of the patients, including sex, age, weight, and distribution of vascular access. The most performed procedure was percutaneous transluminal coronary angioplasty (PTCA) (51.3%), followed by dual-chamber pacemaker implantation (DDDR) (23%), as depicted in [Fig. 2].

Radiation Exposure in Radial and Femoral Procedures
For primary operators (PO), the mean radiation dose was 21.88 µSv in the drape group compared with 47.38 µSv in the control group, reflecting a numerical reduction. Although this difference was not statistically significant, adjustments for AK, DAP, and CAST yielded statistically significant reductions (p < 0.05; [Fig. 3]). Similarly, for secondary operators (SO), the mean dose was reduced from 12.41 µSv in the control group to 8.98 µSv in the drape group. Although the numerical reduction did not reach statistical significance, the adjusted results for AK, DAP, and CAST showed significant reductions (p < 0.05; [Fig. 4]). For technicians, the mean radiation dose decreased from 3.12 µSv in the control group to 2.41 µSv in the drape group. Despite low absolute exposure levels, the adjusted results demonstrated statistical significance (p < 0.05; [Fig. 5]).



Radiation Exposure in Pectoral Procedures
For primary operators, the mean radiation dose was significantly reduced from 96.75 µSv in the control group to 62.86 µSv in the drape group. Adjustments for AK, DAP, and CAST further confirmed the statistical significance of these reductions (p < 0.05; [Fig. 6]). Secondary operators experienced a reduction in mean dose from 34.22 µSv (control) to 23.50 µSv (drape), with adjusted parameters showing significant reductions (p < 0.05; [Fig. 7]). However, for technicians, the mean dose was slightly higher in the drape group (3.36 µSv) compared with the control group (2.80 µSv). Adjustments for AK, DAP, and CAST revealed no statistically significant differences between the groups ([Table 2]).
|
Patient group |
Tech—Dose/AK, µSv/mgy |
Tech—Dose/DAP, µSv/mgycm[2] |
Tech—Dose/CAST, µSv/min |
|---|---|---|---|
|
Control group |
0.01 |
0.01 |
0.104 |
|
Intervention group |
0.01 |
0.01 |
0.101 |
|
Reduction |
−2% |
−2% |
3% |
Abbreviations: AK, air kerma; CAST, cine-adjusted screen time; DAP, dose area product.


Comparative Analysis of Radiation Exposure
Across all procedures, the primary operators received the highest radiation exposure, followed by secondary operators, with technicians receiving the least. In radial and femoral procedures, the primary operator's exposure was consistently higher than that of secondary operators and technicians, as outlined in [Table 3]. The percentage differences in radiation exposure between groups, both with and without the radiation drape, are detailed in [Table 4]. Similarly, in pectoral procedures, the highest exposure was recorded for primary operators, followed by secondary operators and technicians, as summarized in [Table 5]. The percentage reductions in exposure for each group in the presence and absence of the drape are presented in [Table 6].
Abbreviations: PO, primary operator; SO, secondary operator; Tech, technician.
Abbreviations: PO, primary operator; SO, secondary operator; Tech, technician.
Abbreviations: PO, primary operator; SO, secondary operator; Tech, technician.
Abbreviations: PO, primary operator; SO, secondary operator; Tech, technician.
Discussion
Radiation protection in cath laboratories is paramount to mitigating the health risks associated with ionizing radiation. Although strategies such as the ALARA principle, personal protective equipment, and education in radiation safety are well-established,[8] [13] limited literature specifically addresses the exposure levels and associated risks for secondary operators and technicians. This study aimed to fill this gap by evaluating the efficacy of radiation protection drapes, such as RADPAD, in reducing exposure for all personnel categories.
The findings of this study show that radiation protection drapes effectively reduce exposure for primary and secondary operators in both radial/femoral and pectoral procedures. These results align with prior studies showing significant reductions in radiation exposure with the use of RADPAD during interventional procedures.[14] [15] In the RECAP trial, use of the RADPAD reduced operator exposure by 20% compared with standard protection and by 44% compared with a sham shield, with consistent benefits across subgroups such as obese patients and PCI cases. Notably, procedures performed with the sham shield alone resulted in higher operator exposure than standard practice, due to a false sense of security. These findings emphasize that the protective effect is not merely behavioral but directly attributable to the material properties of the drape.[16] A recent comparative study by Cammann et al further supports these findings by demonstrating the effectiveness of radiation protection systems, including RADPAD, in minimizing operator exposure during cardiac catheterization.[14] For technicians, the reductions were significant in radial and femoral procedures but not in pectoral procedures, consistent with prior studies that observed variable effectiveness depending on procedural type and operator position.[17] This discrepancy may be attributed to technicians' relative positioning during procedures, where the drape's protective effect is less pronounced.
When compared with earlier studies, such as the MILD study,[17] the reductions observed in this study are consistent with previously reported ranges. However, the study highlights the need for further exploration into strategies to enhance protection for technicians, especially during pectoral procedures, where exposure reductions remain limited. Importantly, evidence from outside the cardiac setting also supports the benefit of radiation-absorbing drapes: Jansen et al demonstrated that their use during endovascular treatment of peripheral artery disease significantly reduced occupational radiation exposure for operators, with reductions comparable to those seen in coronary interventions. The relative exposure of the primary operator was reduced by 66.5%, the relative exposure of the SO by 68.3%, and the relative exposure of the medical operator by 65.8%.[18]
Several factors may influence the variability in results, including operator behavior, procedural complexity, and the positioning of the radiation source.[19] Although adjustments for confounding factors like AK, DAP, and CAST improved the accuracy of comparisons, certain unmeasured variables, such as the operator's proximity to the radiation source, may have still affected the results. Furthermore, in this study the heightened awareness of radiation safety due to the presence of the drape may have altered operator behavior, potentially introducing bias.[19]
This study has several limitations. The lack of a sham drape introduces the possibility of performance bias. Additionally, despite randomization, baseline matching of patient and procedural characteristics between groups could not be ensured. Background radiation levels, which could influence technician exposure, were not accounted for. The single-center design may also limit generalizability. Moreover, the study primarily involved cardiac procedures, which may restrict extrapolation of the findings to other domains such as abdominal, neuro, or extremity work. Patients undergoing hybrid or multi-site therapies were excluded, which could represent a source of selection bias, as these procedures form a meaningful proportion of interventional practice. Finally, although blinding was attempted, complete operator blinding may not have been achievable, and any awareness of protective measures could have influenced operator technique. Future multicenter investigations addressing these aspects would be valuable to confirm and broaden the applicability of the results.
Conclusion
This study demonstrated that the use of radiation protection drapes significantly reduces radiation exposure for primary and secondary operators during radial, femoral, and pectoral procedures. The reductions were most notable in primary operators, reflecting their proximity to the radiation source, while secondary operators also benefitted substantially. These findings show the importance of incorporating radiation protection drapes into cath laboratory protocols to enhance occupational safety, particularly for personnel with the highest exposure risk.
Conflict of Interest
None declared.
Acknowledgments
The authors would like to express sincere gratitude to the Department of Cardiology at Vardhman Mahavir Medical College & Safdarjung Hospital for providing invaluable support and resources throughout the duration of this study. Special thanks are extended to their colleagues and staff members who contributed their expertise, dedication, and assistance in data collection, analysis, and patient care. Their collaboration and commitment were essential to the successful completion of this research.
Data Availability Statement
Data are available on request with Dr. Zubair Farooq (first author).
Authors' Contributions
All the authors equally conceptualized the study, designed the methodology, conducted data analysis, conducted research, contributed to data collection, drafted the manuscript, and visualized and wrote the review and did editing. All authors read and approved the final manuscript.
Ethical Approval
Approval for the study was obtained from the Institutional Ethics Committee, and the trial was registered with the Clinical Trials Registry of India (CTRI/2022/11/047008). All participants provided informed consent.
-
References
- 1 Al Kharji S, Connell T, Bernier M, Eisenberg MJ. Ionizing radiation in interventional cardiology and electrophysiology. Can J Cardiol 2019; 35 (04) 535-538
- 2 Williams MC, Stewart C, Weir NW, Newby DE. Using radiation safely in cardiology: what imagers need to know. Heart 2019; 105 (10) 798-806
- 3 Andreassi MG, Cioppa A, Botto N. et al. Somatic DNA damage in interventional cardiologists: a case-control study. FASEB J 2005; 19 (08) 998-999
- 4 Karatasakis A, Brilakis HS, Danek BA. et al. Radiation-associated lens changes in the cardiac catheterization laboratory: results from the IC-CATARACT (CATaracts Attributed to RAdiation in the CaTh lab) study. Catheter Cardiovasc Interv 2018; 91 (04) 647-654
- 5 Roguin A, Goldstein J, Bar O. Brain tumours among interventional cardiologists: a cause for alarm? Report of four new cases from two cities and a review of the literature. EuroIntervention 2012; 7 (09) 1081-1086
- 6 Mohapatra A, Greenberg RK, Mastracci TM, Eagleton MJ, Thornsberry B. Radiation exposure to operating room personnel and patients during endovascular procedures. J Vasc Surg 2013; 58 (03) 702-709
- 7 Vlastra W, Claessen BE, Beijk MA. et al. Cardiology fellows-in-training are exposed to relatively high levels of radiation in the cath lab compared with staff interventional cardiologists—insights from the RECAP trial. Neth Heart J 2019; 27 (06) 330-333
- 8 Hirshfeld Jr JW, Ferrari VA, Bengel FM. et al. 2018 ACC/HRS/NASCI/SCAI/SCCT expert consensus document on optimal use of ionizing radiation in cardiovascular imaging—best practices for safety and effectiveness, part 1: radiation physics and radiation biology: a report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol 2018; 71 (24) 2811-2828
- 9 Biso SMR, Vidovich MI. Radiation protection in the cardiac catheterization laboratory. J Thorac Dis 2020; 12 (04) 1648-1655
- 10 Koenig AM, Maas J, Viniol S. et al. Scatter radiation reduction with a radiation-absorbing pad in interventional radiology examinations. Eur J Radiol 2020; 132: 109245
- 11 Borghini A, Gianicolo EAL, Picano E, Andreassi MG. Ionizing radiation and atherosclerosis: current knowledge and future challenges. Atherosclerosis 2013; 230 (01) 40-47
- 12 Shah P, Khanna R, Kapoor A, Goel PK. Efficacy of RADPAD protection drape in reducing radiation exposure in the catheterization laboratory—first Indian study. Indian Heart J 2018; 70 (Suppl. 03) S265-S268
- 13 Simons GR, Orrison Jr WW. Use of a sterile, disposable, radiation-absorbing shield reduces occupational exposure to scatter radiation during pectoral device implantation. Pacing Clin Electrophysiol 2004; 27 (6 Pt 1): 726-729
- 14 Cammann VL, Schweiger V, Cieslik M. et al. Effectiveness of radiation protection systems in the cardiac catheterization laboratory: a comparative study. Clin Res Cardiol 2023; 112 (05) 605-613
- 15 Naidu SS, Abbott JD, Bagai J. et al. SCAI expert consensus update on best practices in the cardiac catheterization laboratory: this statement was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), and the Heart Rhythm Society (HRS) in April 2021. Catheter Cardiovasc Interv 2021; 98 (02) 255-276
- 16 Vlastra W, Delewi R, Sjauw KD. et al. Efficacy of the RADPAD protection drape in reducing operators' radiation exposure in the catheterization laboratory: a sham-controlled randomized trial. Circ Cardiovasc Interv 2017; 10 (11) e006058
- 17 Bhat KG, Guleria VS, Singla M. et al. Minimizing scattered radiation dose in cardiac catheterization laboratory during interventional procedures using lead free drape—MILD study. Indian Heart J 2022; 74 (03) 201-205
- 18 Jansen MM, Koster A, van Herwaarden JA, Hazenberg CEVB. Reduction of occupational radiation exposure during endovascular treatment of peripheral artery disease using radiation absorbing drapes. Ann Vasc Surg 2022; 84: 336-343
- 19 Jones MA, Cocker M, Khiani R. et al. The benefits of using a bismuth-containing, radiation-absorbing drape in cardiac resynchronization implant procedures. Pacing Clin Electrophysiol 2014; 37 (07) 828-833
Address for correspondence
Publication History
Article published online:
10 February 2026
© 2026. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Al Kharji S, Connell T, Bernier M, Eisenberg MJ. Ionizing radiation in interventional cardiology and electrophysiology. Can J Cardiol 2019; 35 (04) 535-538
- 2 Williams MC, Stewart C, Weir NW, Newby DE. Using radiation safely in cardiology: what imagers need to know. Heart 2019; 105 (10) 798-806
- 3 Andreassi MG, Cioppa A, Botto N. et al. Somatic DNA damage in interventional cardiologists: a case-control study. FASEB J 2005; 19 (08) 998-999
- 4 Karatasakis A, Brilakis HS, Danek BA. et al. Radiation-associated lens changes in the cardiac catheterization laboratory: results from the IC-CATARACT (CATaracts Attributed to RAdiation in the CaTh lab) study. Catheter Cardiovasc Interv 2018; 91 (04) 647-654
- 5 Roguin A, Goldstein J, Bar O. Brain tumours among interventional cardiologists: a cause for alarm? Report of four new cases from two cities and a review of the literature. EuroIntervention 2012; 7 (09) 1081-1086
- 6 Mohapatra A, Greenberg RK, Mastracci TM, Eagleton MJ, Thornsberry B. Radiation exposure to operating room personnel and patients during endovascular procedures. J Vasc Surg 2013; 58 (03) 702-709
- 7 Vlastra W, Claessen BE, Beijk MA. et al. Cardiology fellows-in-training are exposed to relatively high levels of radiation in the cath lab compared with staff interventional cardiologists—insights from the RECAP trial. Neth Heart J 2019; 27 (06) 330-333
- 8 Hirshfeld Jr JW, Ferrari VA, Bengel FM. et al. 2018 ACC/HRS/NASCI/SCAI/SCCT expert consensus document on optimal use of ionizing radiation in cardiovascular imaging—best practices for safety and effectiveness, part 1: radiation physics and radiation biology: a report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol 2018; 71 (24) 2811-2828
- 9 Biso SMR, Vidovich MI. Radiation protection in the cardiac catheterization laboratory. J Thorac Dis 2020; 12 (04) 1648-1655
- 10 Koenig AM, Maas J, Viniol S. et al. Scatter radiation reduction with a radiation-absorbing pad in interventional radiology examinations. Eur J Radiol 2020; 132: 109245
- 11 Borghini A, Gianicolo EAL, Picano E, Andreassi MG. Ionizing radiation and atherosclerosis: current knowledge and future challenges. Atherosclerosis 2013; 230 (01) 40-47
- 12 Shah P, Khanna R, Kapoor A, Goel PK. Efficacy of RADPAD protection drape in reducing radiation exposure in the catheterization laboratory—first Indian study. Indian Heart J 2018; 70 (Suppl. 03) S265-S268
- 13 Simons GR, Orrison Jr WW. Use of a sterile, disposable, radiation-absorbing shield reduces occupational exposure to scatter radiation during pectoral device implantation. Pacing Clin Electrophysiol 2004; 27 (6 Pt 1): 726-729
- 14 Cammann VL, Schweiger V, Cieslik M. et al. Effectiveness of radiation protection systems in the cardiac catheterization laboratory: a comparative study. Clin Res Cardiol 2023; 112 (05) 605-613
- 15 Naidu SS, Abbott JD, Bagai J. et al. SCAI expert consensus update on best practices in the cardiac catheterization laboratory: this statement was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), and the Heart Rhythm Society (HRS) in April 2021. Catheter Cardiovasc Interv 2021; 98 (02) 255-276
- 16 Vlastra W, Delewi R, Sjauw KD. et al. Efficacy of the RADPAD protection drape in reducing operators' radiation exposure in the catheterization laboratory: a sham-controlled randomized trial. Circ Cardiovasc Interv 2017; 10 (11) e006058
- 17 Bhat KG, Guleria VS, Singla M. et al. Minimizing scattered radiation dose in cardiac catheterization laboratory during interventional procedures using lead free drape—MILD study. Indian Heart J 2022; 74 (03) 201-205
- 18 Jansen MM, Koster A, van Herwaarden JA, Hazenberg CEVB. Reduction of occupational radiation exposure during endovascular treatment of peripheral artery disease using radiation absorbing drapes. Ann Vasc Surg 2022; 84: 336-343
- 19 Jones MA, Cocker M, Khiani R. et al. The benefits of using a bismuth-containing, radiation-absorbing drape in cardiac resynchronization implant procedures. Pacing Clin Electrophysiol 2014; 37 (07) 828-833