

Subscribe to RSS
DOI: 10.1055/s-0045-1813740
Case Report of Urachal Remnant Causing Extensive Fistulization between the Sigmoid Colon and Bilateral Adnexae with Cyst-Cutaneous Fistula
Authors

Abstract
Case report
We present the case of a 20-year-old female with purulent umbilical drainage.
Materials and Methods
Workup initially included a contrast-enhanced computed tomography scan of the abdomen and pelvis, which revealed large bilateral tubo-ovarian abscesses communicating with a tract to the umbilicus, with concern regarding involvement of the sigmoid colon. A drain was placed, and cultures from the abscess demonstrated growth of α-hemolytic streptococci and Trueperella (Arcanobacterium) bernardiae.
Results
Colonoscopy was normal. During preparation for colonoscopy, the patient noted passage of high volume of clear fluid from the umbilicus. A fistulogram through the umbilical opening revealed a complex fistulous network involving the umbilicus, bilateral adnexa and rectosigmoid, with concern for small bowel involvement. Magnetic resonance enterography was unremarkable for bowel inflammation, but the study suggested the possibility of an underlying urachal remnant. Diagnostic laparoscopy was performed, which excluded presence of any small bowel involvement, and demonstrated dense adhesions of the omentum and left adnexa to the abdominal wall. Ultimately, the patient underwent a multi-disciplinary robotic-assisted urachal remnant excision, with en-bloc left oophorectomy and sigmoidectomy.
Conclusion
Urachal and omphalomesenteric remnants outside of the pediatric population are rare. To the best of our knowledge, this is the first report of such complication of a urachal remnant, with a complex fistula involving the rectosigmoid colon, adnexa and bladder. Here, we present the diagnostic and operative approach.
Introduction
The urachus is a structure between the bladder and umbilicus that allows the fetus to drain urine while developing in utero.[1] Typically, this channel obliterates by the end of gestation, leaving behind the median umbilical ligament.[1] However, incomplete atresia of this structure results in various urachal remnants, such as urachal cysts, sinuses, and diverticula. These remnants can be complicated by infection, fistulization, and neoplasm. We present the case of a 20-year-old female who presented with an infected urachal remnant that required excision of the urachal remnant, as well as a left oophorectomy and sigmoidectomy due to extensive fistulization.
Case Presentation & Diagnostic Work-Up
A 20-year-old patient presented to the emergency department with new umbilical drainage. She described the drainage as feculent, with passage of gas and food particles. Work-up initially included a contrast-enhanced computed tomography scan of the abdomen and pelvis as well as a transvaginal ultrasound, which revealed large bilateral tubo-ovarian abscesses communicating with a tract to the umbilicus, with concern regarding involvement of the sigmoid colon. A percutaneous drain was placed, and cultures from the abscess demonstrated growth of α-hemolytic streptococci and Trueperella (Arcanobacterium) bernardiae.
Due to the finding of such a complex fistula in a young, not sexually active woman, the differential diagnosis included Crohn's disease and urachal remnant. Colonoscopy was performed, including ileal intubation, with normal results. During preparation for colonoscopy, however, the patient noted passage of a high volume of clear fluid from the umbilicus, presumed to represent the precolonoscopy preparation solution.
A fistulogram was then performed through the umbilical opening, which revealed a complex fistulous network involving the umbilicus, bilateral adnexa, and rectosigmoid colon, with concern regarding small bowel involvement ([Fig. 1]). Computed tomography scans of the abdomen and pelvis, and a magnetic resonance enterography were unremarkable for bowel inflammation, but the studies suggested the possibility of an underlying urachal remnant ([Fig. 2]). The possibility was raised given the typical anterior, prevesical location of the fistulous tract, which extended from the superior bladder to the umbilicus, the anatomical location of the urachus ([Fig. 2]).


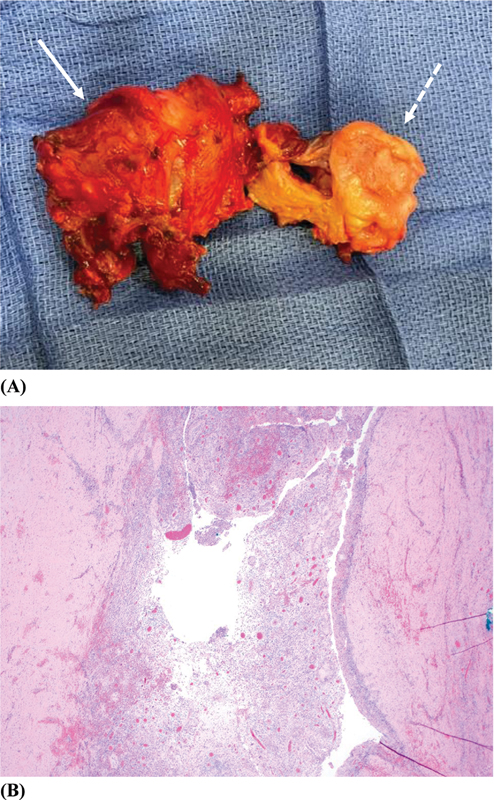
Diagnostic laparoscopy was performed to assess the involvement of the adnexa to aid in surgical planning in this patient as well as to assess for small bowel involvement versus Crohn's disease. The findings of the laparoscopy excluded the presence of any small bowel involvement and demonstrated dense adhesions of the omentum and left adnexa to the abdominal wall. Subsequently, the patient underwent a multi-disciplinary robotic-assisted urachal remnant excision from the urinary bladder wall, with en-bloc left oophorectomy and sigmoidectomy ([Fig. 3A]). Histological examination showed a urachal remnant cyst with dense, acute chronic inflammation attached to smooth musculatures from the urinary bladder wall ([Fig. 3B]).
Discussion
Urachal anomalies outside of the pediatric population are rare. Although the exact incidence is unknown due to a significant portion of them being asymptomatic or undiagnosed, some autopsy studies have shown a 1 in 5,000 prevalence rate.[2] With respect to symptoms, patients typically present with umbilical drainage, lower abdominal pain, palpable mass, or an infection, which can be easily mistaken for appendicitis or Meckel's diverticulum.[3] [4] Cases have been reported of infected urachal remnants that have grown various bacterial strains, including Actinomyces turicensis, Proteus mirabilis, and Escherichia coli.[5] [6]
Urachal infections can lead to complications such as cellulitis, abscess, necrotizing soft-tissue infection, sepsis, malignancy, and, in rare cases, death. Historically, all urachal anomalies were recommended to be surgically resected; however, this has since been somewhat challenged given the low incidence of urachal anomalies overall coupled with a low prevalence of urachal carcinoma.[7] [8] [9] [10] [11] If managing urachal anomalies non-operatively, it is imperative that the patient and family be counseled on the possibility of malignancy, as there have also been cases reported of biopsy-proven benign disease converting into aggressive forms of urachal carcinoma several years later, ultimately requiring oncologic resection and adjuvant chemotherapy.[12] There currently is not a standardized surveillance plan for cases of non-operatively managed urachal anomalies; thus, a follow-up plan should be made in a multi-disciplinary manner, which includes the patient.
In cases of urachal carcinoma, presenting symptoms may include hematuria, followed by pain, lower urinary tract symptoms, mass, and mucinuria.[12] Significant predictors of malignancy include age over 55 years and hematuria. Furthermore, there is a poor 5-year prognosis of less than 50% survival rate due to a high rate of locally-advanced or metastatic disease at the time of diagnosis.[12] [13] [14] As such, patients who present with urachal anomalies are still generally recommended to undergo a surgical resection.
Although there have been reports of infected urachal remnants requiring surgical resection in the adult population before, to the best of our knowledge, this is the first report of such an extensive fistulous network requiring surgical resection of the urachal remnant as well as the ovary and sigmoid. Ultimately, our patient had a robotic-assisted urachal remnant excision, with en-bloc left oophorectomy and sigmoidectomy. Her final pathology was consistent with fistulous urachal cyst with dense and chronic inflammation. Her left ovary, fallopian tube, and sigmoid also showed chronic inflammation with remnants of healed fistulous tracts. Postoperatively, the patient did well and was discharged tolerating a diet and an indwelling foley. She then had the catheter removed during her postoperative appointment following a negative cystogram. She continues to do well today.
Conflict of Interests
The authors have no conflict of interests to declare.
Authors' Contributions
-
References
- 1 Briggs KB, Rentea RM. Patent Urachus. Treasure Island (FL): StatPearls Publishing; 2025. . Available from: https://www.ncbi.nlm.nih.gov/books/NBK557723/
- 2 Mahato NK, Mittal MM, Aggarwal R, Munjal KM. Encysted Urachal Abscess Associated With a Premalignant Lesion in an Adult Male. Urotoday Int J 2010; 3 (05)
- 3 Ramdani H, Benelhosni K, MoatassimBillah N, Nassar I. Infected Urachal Sinus in an Adult. Cureus 2021; 13 (06) e15693
- 4 Özel LZ, Talu M, User Y, Aydin N, Marur T. Coexistence of a Meckel's diverticulum and a urachal remnant. Clin Anat 2005; 18 (08) 609-612
- 5 Xu L, Sun B, Gao Z, Bu X, Wan Y, Chen J. Urachal Remnant Infection Caused by Actinomyces Turicensis. Clin Lab 2023; 69 (12) •••
- 6 Tazi F, Ahsaini M, Khalouk A, Mellas S, Stuurman-Wieringa RE, Elfassi MJ, Farih MH. Abscess of urachal remnants presenting with acute abdomen: a case series. J Med Case Rep 2012; 6: 226
- 7 Gleason JM, Bowlin PR, Bagli DJ, Lorenzo AJ, Hassouna T, Koyle MA, Farhat WA. A comprehensive review of pediatric urachal anomalies and predictive analysis for adult urachal adenocarcinoma. J Urol 2015; 193 (02) 632-636
- 8 Ashley RA, Inman BA, Routh JC, Rohlinger AL, Husmann DA, Kramer SA. Urachal anomalies: a longitudinal study of urachal remnants in children and adults. J Urol 2007; 178 (4 Pt 2): 1615-1618
- 9 Copp HL, Wong IY, Krishnan C, Malhotra S, Kennedy WA. Clinical presentation and urachal remnant pathology: implications for treatment. J Urol 2009; 182 (04) 1921-1924
- 10 Lipskar AM, Glick RD, Rosen NG, Layliev J, Hong AR, Dolgin SE, Soffe SZ. Nonoperative management of symptomatic urachal anomalies. J Pediatr Surg 2010; 45 (05) 1016-1019
- 11 Nogueras-Ocaña M, Rodríguez-Belmonte R, Uberos-Fernández J, Jiménez-Pacheco A, Merino-Salas S, Zuluaga-Gómez A. Urachal anomalies in children: surgical or conservative treatment?. J Pediatr Urol 2014; 10 (03) 522-526
- 12 Rhudd A, Moghul M, Nair G, McDonald J. Malignant transformation of a urachal cyst-a case report and literature review. J Surg Case Rep 2018; 2018 (03) rjy056
- 13 Ashley RA, Inman BA, Sebo TJ, Leibovich BC, Blute ML, Kwon ED, Zincke H. Urachal carcinoma: clinicopathologic features and long-term outcomes of an aggressive malignancy. Cancer 2006; 107 (04) 712-720
- 14 Bruins HM, Visser O, Ploeg M, Hulsbergen-van de Kaa CA, Kiemeney LA, Witjes JA. The clinical epidemiology of urachal carcinoma: results of a large, population based study. J Urol 2012; 188 (04) 1102-1107
Address for correspondence
Publication History
Received: 16 February 2025
Accepted: 11 August 2025
Article published online:
29 December 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution 4.0 International License, permitting copying and reproduction so long as the original work is given appropriate credit (https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda.
Rua Rego Freitas, 175, loja 1, República, São Paulo, SP, CEP 01220-010, Brazil
Yaeji Park, Carla Harmath, Gladell P. Paner, Hillary McLaren, Obianuju Sandra Madueke-Laveaux, Sarah Faris, Kinga S. Olortegui. Case Report of Urachal Remnant Causing Extensive Fistulization between the Sigmoid Colon and Bilateral Adnexae with Cyst-Cutaneous Fistula. Journal of Coloproctology 2025; 45: s00451813740.
DOI: 10.1055/s-0045-1813740
-
References
- 1 Briggs KB, Rentea RM. Patent Urachus. Treasure Island (FL): StatPearls Publishing; 2025. . Available from: https://www.ncbi.nlm.nih.gov/books/NBK557723/
- 2 Mahato NK, Mittal MM, Aggarwal R, Munjal KM. Encysted Urachal Abscess Associated With a Premalignant Lesion in an Adult Male. Urotoday Int J 2010; 3 (05)
- 3 Ramdani H, Benelhosni K, MoatassimBillah N, Nassar I. Infected Urachal Sinus in an Adult. Cureus 2021; 13 (06) e15693
- 4 Özel LZ, Talu M, User Y, Aydin N, Marur T. Coexistence of a Meckel's diverticulum and a urachal remnant. Clin Anat 2005; 18 (08) 609-612
- 5 Xu L, Sun B, Gao Z, Bu X, Wan Y, Chen J. Urachal Remnant Infection Caused by Actinomyces Turicensis. Clin Lab 2023; 69 (12) •••
- 6 Tazi F, Ahsaini M, Khalouk A, Mellas S, Stuurman-Wieringa RE, Elfassi MJ, Farih MH. Abscess of urachal remnants presenting with acute abdomen: a case series. J Med Case Rep 2012; 6: 226
- 7 Gleason JM, Bowlin PR, Bagli DJ, Lorenzo AJ, Hassouna T, Koyle MA, Farhat WA. A comprehensive review of pediatric urachal anomalies and predictive analysis for adult urachal adenocarcinoma. J Urol 2015; 193 (02) 632-636
- 8 Ashley RA, Inman BA, Routh JC, Rohlinger AL, Husmann DA, Kramer SA. Urachal anomalies: a longitudinal study of urachal remnants in children and adults. J Urol 2007; 178 (4 Pt 2): 1615-1618
- 9 Copp HL, Wong IY, Krishnan C, Malhotra S, Kennedy WA. Clinical presentation and urachal remnant pathology: implications for treatment. J Urol 2009; 182 (04) 1921-1924
- 10 Lipskar AM, Glick RD, Rosen NG, Layliev J, Hong AR, Dolgin SE, Soffe SZ. Nonoperative management of symptomatic urachal anomalies. J Pediatr Surg 2010; 45 (05) 1016-1019
- 11 Nogueras-Ocaña M, Rodríguez-Belmonte R, Uberos-Fernández J, Jiménez-Pacheco A, Merino-Salas S, Zuluaga-Gómez A. Urachal anomalies in children: surgical or conservative treatment?. J Pediatr Urol 2014; 10 (03) 522-526
- 12 Rhudd A, Moghul M, Nair G, McDonald J. Malignant transformation of a urachal cyst-a case report and literature review. J Surg Case Rep 2018; 2018 (03) rjy056
- 13 Ashley RA, Inman BA, Sebo TJ, Leibovich BC, Blute ML, Kwon ED, Zincke H. Urachal carcinoma: clinicopathologic features and long-term outcomes of an aggressive malignancy. Cancer 2006; 107 (04) 712-720
- 14 Bruins HM, Visser O, Ploeg M, Hulsbergen-van de Kaa CA, Kiemeney LA, Witjes JA. The clinical epidemiology of urachal carcinoma: results of a large, population based study. J Urol 2012; 188 (04) 1102-1107