

Subscribe to RSS
DOI: 10.1055/s-0045-1813720
Optic Nerve Sheath Diameter Monitoring in Case of Blast Head Injury Complicated by Posttraumatic Occlusive Hydrocephaly: Case Report
Monitorização do diâmetro da bainha do nervo óptico em um caso de traumatismo craniano causado por explosão e complicado por hidrocefalia oclusiva pós-traumática: Relato de casoAuthors


Abstract
The presence of posttraumatic hydrocephaly signs and symptoms in conjunction with those of the primary injury sometimes makes diagnosis challenging. There is a paucity of literature about the correlation between optic nerve sheath diameter (ONSD) and the outcome of cerebral spinal fluid diversion procedures in adults with posttraumatic hydrocephaly. The present case report illustrates the efficacy of ONSD monitoring in evaluating intracranial hypertension after blast head injury complicated by occlusive hydrocephaly and in assessing the efficacy of cerebrospinal fluid diversion procedures.
Resumo
A presença de sinais e sintomas de hidrocefalia pós-traumática em conjunto com os da lesão primária torna por vezes o diagnóstico difícil. Existe uma escassez de literatura sobre a correlação entre o diâmetro da bainha do nervo óptico (DBNO) e o resultado dos procedimentos de desvio do líquido cefalorraquidiano em adultos com hidrocefalia pós-traumática. Este relato de caso ilustra a eficácia da monitorização do DBNO na avaliação da hipertensão intracraniana após traumatismo craniano causado por explosão e complicado por hidrocefalia oclusiva e na avaliação da eficácia dos procedimentos de desvio do líquido cefalorraquidiano.
Keywords
optic nerve sheath diameter - blast head injury - posttraumatic occlusive hydrocephaly - neuroendoscopic third ventriculostomyPalavras-chave
diâmetro da bainha do nervo óptico - traumatismo cranioencefálico por explosão - hidrocefalia oclusiva pós-traumática - terceiroventriculostomia por via endoscópicaIntroduction
Despite the existence of several proposed diagnostic criteria, there is no consensus on the most appropriate approach for the diagnosis of posttraumatic occlusive hydrocephaly (PTOHC).[1] [2] A notable gap in the literature exists regarding PTOHC following blast traumatic brain injury (BTBI). Novel examination techniques may facilitate more accurate diagnostic, particularly when the diagnosis is uncertain based on clinical assessment and routine radiological findings.[2]
The ultrasonographic measurement of the optic nerve sheath diameter (ONSD) can be used to predict the presence of elevated intracranial pressure (ICP)[3] and represents a reliable option for the noninvasive measurement of ICP dynamics.[4] There is a significant difference between internal and external ONSDs in subjects with elevated and nonelevated ICP. External ONSD (eONSD) gives more accurate prediction of intracranial hypertension.[3] [5] However, the inability to reflect the rapid changes in ICP is a significant disadvantage of ONSD measurement. There is a paucity of literature about the correlation between ONSD and the outcome of cerebrospinal fluid (CSF) diversion procedures in adults with hydrocephalus, particularly in the context of BTBI.[4] The present case report illustrates the potential value of ONSD monitoring in evaluating intracranial hypertension and assessing the outcome of CSF diversion procedures in a case of complicated BTBI.
Clinical Case
We present the case of a 36-year-old male with blast injury, namely tangential, nonpenetrating shrapnel traumatic brain injury (TBI) in the right occipital region with a linear fracture of the occipital bone scale, severe brain contusion with an acute subdural hematoma over the right cerebellar hemisphere and a focus of hemorrhagic contusion in it, occlusive hydrocephalus, and hematorrhachis.
Surgical care was performed in the tertiary military medical center: primary wound washing; external drainage of the anterior horn of the right lateral ventricle; right sided suboccipital craniectomy, evacuation of the subdural hematoma of the posterior fossa and the removal of the contusion focus on the right cerebellar hemisphere.
On the 7th day, the patient was evacuated to our institution with external ventricular drain (EVD). On admission, the patient had reduced consciousness to the level of Glasgow coma scale (GCS) 13 (E3, V4, M6), with left-sided hemiparesis and bulbar syndrome that required the use of a nasogastric feeding tube. Other vital signs were within normal range, including SpO2 level of 98% in room air, blood pressure of 120/85 mmHg, and heart rate of 84 bpm.
The Fujifilm Sonosite M-Turbo Portable Ultrasound Machine (Fujifilm), configured for ophthalmic examinations, was used with a 10-5MHz linear transducer probe. The eONSD was measured externally to the dura mater at a depth of 3 mm behind the retina ([Fig. 1D]) from images obtained at both the transverse and sagittal planes of each eye.[3] [5] The mean value of the eONSD (mONSD) was then calculated from all 4 views, measuring 0.76 cm on admission. On the 9th day following the injury, it decreased to 0.7 cm, and the EVD was removed.

On the morning of the 10th day, the patient status deteriorated with motor aphasia, vertical nystagmus, vomiting, and neck stiffness, with a reduced level of consciousness to the level of GCS 9 (E2, V1, M6), hypertension (160/100 mmHg), and tachycardia (118 bpm). The mONSD was enlarged to 0.91 cm ([Fig. 1D]). The third ventricle hydrocephaly was found on a computed tomography (CT) scan ([Fig. 1]). The left-sided neuroendoscopic third ventriculostomy (ETV) was performed urgently with EVD insertion for the management of elevated ICP. The antimicrobial treatment was escalated to a combination of meropenem and linezolid. The mONSD decreased to 0.74 cm under conditions of controlled mechanical ventilation and propofol sedation on the 4th hour after surgery.
On the 11th day, the signs of intracranial hypertension reversed and the mONSD decreased to 0.69 cm. The patient was successfully extubated. The laboratory tests of CSF revealed a white blood cell (WBC) count of 110 cells/mm3, protein concentration of 2,500mg/dL, and glucose level of 57.6mg/dL. Posttraumatic meningitis was suspected.
On the morning of the 14th day, the EVD was clamped, but an increase of mONSD to 0.77cm was detected ([Fig. 2D]). The EVD was reopened for 24 hours. The results of bacteriological tests revealed Staphylococcus epidermidis, resistant to erythromycin and ciprofloxacin, but sensitive to linezolid, clindamycin, moxifloxacin, tetracycline and rifampicin.
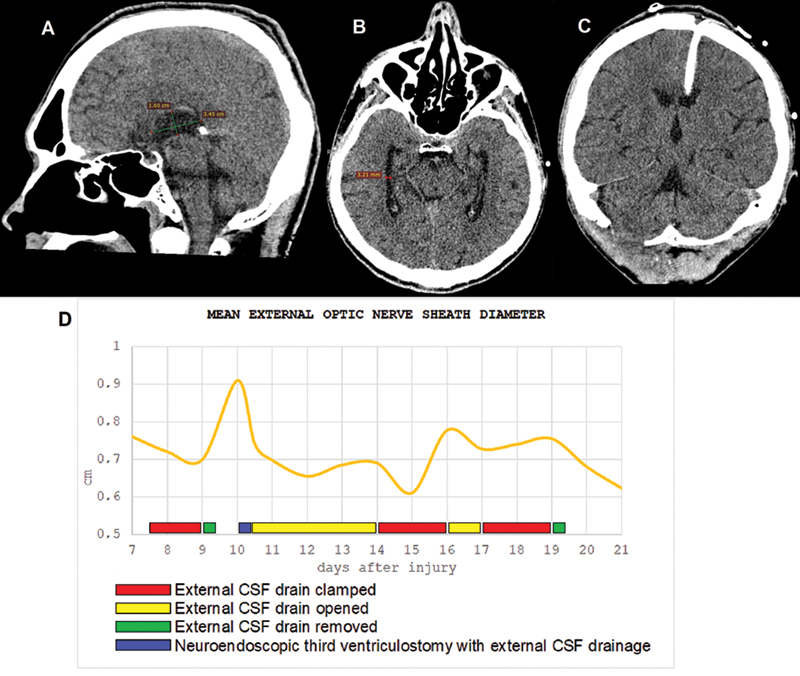
On the 17th day, a CT scan evidenced the resolution of hydrocephalus ([Fig. 2]); the mONSD was 0.73cm. The EVD was clamped for 2 days and was successfully removed. On the 19th day, CSF laboratory tests indicated a WBC count of 6 cells/mm3, protein concentration of 35mg/dL and glucose level of 55.8mg/dL.
On the 23rd day of hospital stay, the rehabilitation program was expanded, and on the 28th day the patient was discharged from the intensive care unit.
Discussion
The presence of PTOHC signs and symptoms in conjunction with those of the primary injury sometimes makes diagnosis challenging.[2] [6] [7] Several studies have been conducted to investigate the relationship between ONSD and intracranial hypertension, with varying cutoff values observed in different populations.[3] However, there is a paucity of similar studies in the context of BTBI.
The absence of an opportunity to reflect the rapid changes in ICP is a significant disadvantage of ONSD measurement due to the discontinuous nature of this method. For any monitoring device, a combination of clinical examination and interpretation conducted in the context of a comprehensive review of available data is a fundamental aspect.[8]
According to previous data, the cutoff value of eONSD for ICP > 22mmHg is 0.67cm.[5] In our case, the eONSD level was 36% higher than this value with clinical signs of severe ICH ([Fig. 2D]). Neuroendoscopic third ventriculostomy is less effective for the treatment of OHC in previously shunted patients, but its combination with concurrent shunting may prevent treatment failure.[9] Therefore, the decision was made to combine ETV with EVD. The ventricular-peritoneal shunting in the context of a septic complication of a shrapnel BTBI is a challenging decision. The present case report demonstrates that ONSD monitoring can be a reliable tool to reflect changes in ICP in conditions such as PTOHC when high amplitude changes in ICP are suspected. The implementation of noninvasive methods for the screening of elevated ICP could potentially enhance the quality of care for these patients.[5]
Conclusion
The present case report demonstrates that ONSD monitoring in PTOHC can facilitate the evaluation of the outcomes achieved by CSF diversion procedures. It can serve as an additional noninvasive, easy, cheap, and reproducible bedside tool for guiding the management of increased ICP in cases of blast TBI with complicated CSF dynamics. Nevertheless, further randomized studies are required in order to ascertain accurate threshold values of the ONSD regarding the enhancement of the decision-making process regarding specific interventions for CSF diversion procedures.
Conflict of Interests
The authors have no conflict of interests to declare.
-
References
- 1 Kammersgaard LP, Linnemann M, Tibæk M. Hydrocephalus following severe traumatic brain injury in adults. Incidence, timing, and clinical predictors during rehabilitation. NeuroRehabilitation 2013; 33 (03) 473-480
- 2 Heinonen A, Rauhala M, Isokuortti H. et al. Incidence of surgically treated post-traumatic hydrocephalus 6 months following head injury in patients undergoing acute head computed tomography. Acta Neurochir (Wien) 2022; 164 (09) 2357-2365
- 3 Sitanaya SN, Kamayanti F, Nugroho HA, Prabowo B. Comparing ultrasonographic optic nerve sheath diameter to head computed tomography scan to predict intracranial pressure elevation. SAGE Open Med 2022; 10: 20 503121221077834
- 4 Salih MSM, Sethuramachandran A, Bidkar PU. et al. Comparison of Optic Nerve Sheath Diameter (ONSD) Measurements Obtained from USG Before and After Placement of Ventriculoperitoneal Shunt in Obstructive Hydrocephalus as a Surrogate Marker for Adequacy of Shunt Function: A Prospective Observational Study. Asian J Neurosurg 2024; 19 (02) 242-249
- 5 Pansell J, Bell M, Rudberg P, Friman O, Cooray C. Optic nerve sheath diameter in intracranial hypertension: Measurement external or internal of the dura mater?. J Neuroimaging 2023; 33 (01) 58-66
- 6 De Bonis P, Anile C. Post-traumatic hydrocephalus: the Cinderella of Neurotrauma. Expert Rev Neurother 2020; 20 (07) 643-646
- 7 Chen KH, Lee CP, Yang YH. et al. Incidence of hydrocephalus in traumatic brain injury: A nationwide population-based cohort study. Medicine (Baltimore) 2019; 98 (42) e17568
- 8 Lilly CM, Boyle WA, Irwin RS, Rippe JM. Irwin & Rippe's Intensive Care Medicine. 9th ed. Lippincott Williams & Wilkins; 2024
- 9 Woodworth G, McGirt MJ, Thomas G, Williams MA, Rigamonti D. Prior CSF shunting increases the risk of endoscopic third ventriculostomy failure in the treatment of obstructive hydrocephalus in adults. Neurol Res 2007; 29 (01) 27-31
Address for correspondence
Publication History
Received: 12 January 2025
Accepted: 09 September 2025
Article published online:
29 December 2025
© 2025. Sociedade Brasileira de Neurocirurgia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua Rego Freitas, 175, loja 1, República, São Paulo, SP, CEP 01220-010, Brazil
-
References
- 1 Kammersgaard LP, Linnemann M, Tibæk M. Hydrocephalus following severe traumatic brain injury in adults. Incidence, timing, and clinical predictors during rehabilitation. NeuroRehabilitation 2013; 33 (03) 473-480
- 2 Heinonen A, Rauhala M, Isokuortti H. et al. Incidence of surgically treated post-traumatic hydrocephalus 6 months following head injury in patients undergoing acute head computed tomography. Acta Neurochir (Wien) 2022; 164 (09) 2357-2365
- 3 Sitanaya SN, Kamayanti F, Nugroho HA, Prabowo B. Comparing ultrasonographic optic nerve sheath diameter to head computed tomography scan to predict intracranial pressure elevation. SAGE Open Med 2022; 10: 20 503121221077834
- 4 Salih MSM, Sethuramachandran A, Bidkar PU. et al. Comparison of Optic Nerve Sheath Diameter (ONSD) Measurements Obtained from USG Before and After Placement of Ventriculoperitoneal Shunt in Obstructive Hydrocephalus as a Surrogate Marker for Adequacy of Shunt Function: A Prospective Observational Study. Asian J Neurosurg 2024; 19 (02) 242-249
- 5 Pansell J, Bell M, Rudberg P, Friman O, Cooray C. Optic nerve sheath diameter in intracranial hypertension: Measurement external or internal of the dura mater?. J Neuroimaging 2023; 33 (01) 58-66
- 6 De Bonis P, Anile C. Post-traumatic hydrocephalus: the Cinderella of Neurotrauma. Expert Rev Neurother 2020; 20 (07) 643-646
- 7 Chen KH, Lee CP, Yang YH. et al. Incidence of hydrocephalus in traumatic brain injury: A nationwide population-based cohort study. Medicine (Baltimore) 2019; 98 (42) e17568
- 8 Lilly CM, Boyle WA, Irwin RS, Rippe JM. Irwin & Rippe's Intensive Care Medicine. 9th ed. Lippincott Williams & Wilkins; 2024
- 9 Woodworth G, McGirt MJ, Thomas G, Williams MA, Rigamonti D. Prior CSF shunting increases the risk of endoscopic third ventriculostomy failure in the treatment of obstructive hydrocephalus in adults. Neurol Res 2007; 29 (01) 27-31