

Subscribe to RSS
DOI: 10.1055/s-0045-1813716
Comparison Between Endoscopic and Microsurgical Fenestration for Subarachnoid Cysts: A Systematic Review and Meta-Analysis
Comparação entre Fenestração Endoscópica e Microcirúrgica para Cistos Aracnóides: Revisão Sistemática e Meta-AnáliseAuthors
Funding This research was not supported.


Abstract
Introduction
Intracranial arachnoid cysts are cerebrospinal fluid–filled lesions present in 1.2–1.4% of the population. They are often asymptomatic but may cause headache, seizures, deficits, or hydrocephalus. Surgery is indicated in symptomatic cases, yet the optimal technique—endoscopic fenestration or microsurgery—remains debated.
Objective
To compare efficacy and safety of endoscopic fenestration versus microsurgery for symptomatic intracranial arachnoid cysts through systematic review and meta-analysis.
Methods
PubMed, Embase, Scopus, Web of Science, and Cochrane Library were searched up to March 2024, following PRISMA 2020. Comparative studies reporting cyst volume reduction (>50%) or postoperative complications (hematoma, cranial nerve palsy, mortality) were included. Data were analyzed with Review Manager 5.4 and R. Pooled relative risks (RR) with 95% confidence intervals (CI) were calculated using Hartung-Knapp adjustments and Paule-Mandel variance. Publication bias was assessed with funnel plots and Egger's test.
Results
Sixteen studies (1,157 patients; 596 endoscopic, 561 microsurgery) were included. Eight studies (n = 441) showed no significant difference in cyst reduction (RR = 0.92; 95% CI: 0.77–1.10; p = 0.325; I2 = 63.4%). Twelve studies (n = 716) suggested fewer hematomas with endoscopy, though not significant (RR = 0.61; 95% CI: 0.32–1.17; p = 0.139; I2 = 0%). Cranial nerve palsy was rare (<3%), and no mortality was reported.
Conclusion
Endoscopic fenestration and microsurgery provide similar efficacy and safety. Choice should be guided by cyst anatomy and surgeon expertise. Further randomized trials are warranted.
Resumo
Introdução
Cistos aracnóides intracranianos são lesões preenchidas por líquido cerebrospinal, presentes em 1,2%–1,4% da população. Embora geralmente assintomáticos, podem causar cefaleia, crises epilépticas, déficits neurológicos ou hidrocefalia. A cirurgia é indicada nos casos sintomáticos, mas a escolha entre fenestração endoscópica e microcirurgia ainda é debatida.
Objetivo
Comparar eficácia e segurança da fenestração endoscópica em relação à microcirurgia para cistos aracnóides sintomáticos por meio de revisão sistemática e meta-análise.
Métodos
Realizou-se busca em PubMed, Embase, Scopus, Web of Science e Cochrane Library até março de 2024, seguindo PRISMA 2020. Foram incluídos estudos comparativos que relataram redução de volume do cisto (>50%) ou complicações pós-operatórias (hematoma, paresia de nervo craniano, mortalidade). Os dados foram analisados com Review Manager 5.4 e R. Calcularam-se riscos relativos (RR) com intervalos de confiança de 95% (IC), aplicando ajustes de Hartung-Knapp e variância de Paule-Mandel. O viés de publicação foi avaliado por funnel plots e teste de Egger.
Resultados
Dezesseis estudos (1.157 pacientes; 596 endoscopia, 561 microcirurgia) foram incluídos. Oito estudos (n = 441) não mostraram diferença significativa na redução do cisto (RR = 0,92; IC 95%: 0,77–1,10; p = 0,325; I2 = 63,4%). Doze estudos (n = 716) sugeriram menos hematomas na endoscopia, sem significância estatística (RR = 0,61; IC 95%: 0,32–1,17; p = 0,139; I2 = 0%). Paresia de nervo craniano foi rara (<3%), e não houve mortalidade.
Conclusão
Fenestração endoscópica e microcirurgia apresentam eficácia e segurança semelhantes. A escolha deve considerar fatores anatômicos e experiência do cirurgião. Ensaios randomizados adicionais são necessários.
Keywords
Arachnoid cyst - endoscopic fenestration - microsurgery - intracranial cysts - systematic review - meta-analysisPalavras-chave
Cisto aracnóide - fenestração endoscópica - microcirurgia - cistos intracranianos - revisão sistemática - meta-análiseIntroduction
Arachnoid cysts are extra-axial collections of cerebrospinal fluid encapsulated between the arachnoid layers, present in ∼1.2% to 1.4% of the general population, as evidenced by magnetic resonance imaging studies on large adult population samples.[1] [2] [3] They are more prevalent in males and are most frequently located in the middle cranial fossa (∼34%) and the posterior fossa (33%).[1] [4] Although typically asymptomatic, arachnoid cysts can cause symptoms such as headache, seizures, focal neurological deficits, or hydrocephalus, particularly when located in critical regions of the central nervous system.[2] [4]
However, the current literature remains inconclusive regarding the optimal surgical approach. Comparative studies between endoscopic fenestration and microsurgical techniques report conflicting results depending on the anatomical location of the cyst. For instance, in suprasellar, quadrigeminal, and posterior fossa cysts, endoscopic fenestration has demonstrated clinical success rates approaching 90%, comparable to microsurgery, whereas its efficacy has been lower for sylvian fissure cysts.[5] [6] [7]
Given this gap in evidence and the methodological variability among studies, there is a need for a systematic review and meta-analysis that critically synthesizes the available data. By pooling information from multiple comparative cohorts, it is possible to enhance statistical precision and more clearly evaluate the efficacy and safety of surgical techniques, thereby contributing to evidence-based practice.
Therefore, this systematic review and meta-analysis was conducted with the objective of directly comparing endoscopic fenestration and microsurgical approaches for the treatment of intracranial arachnoid cysts. The data included in this review and meta-analysis involve patients with intracranial arachnoid cysts who underwent endoscopic fenestration and those who underwent microsurgical treatment, with primary outcomes defined as cyst volume reduction (>50%) and secondary outcomes including clinical complications (hematoma, cranial nerve palsy, and mortality).
Methods
Protocol and Registration
This systematic review and meta-analysis was conducted in accordance with the PRISMA 2020 guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). This study is registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the ID CRD420251149264, and the results are reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.[8] [9]
Eligibility Criteria
Comparative observational studies (retrospective and prospective cohorts, as well as case series with a control group) and randomized clinical trials that directly investigated the efficacy and/or safety of endoscopic fenestration compared with microsurgery for the treatment of intracranial arachnoid cysts were considered eligible. Studies were required to provide quantitative data allowing the extraction of at least one of the outcomes of interest 1: cyst volume reduction, defined as a reduction greater than 50% on postoperative imaging 2; postoperative complications, such as hematomas (subdural, epidural, or intraparenchymal), cranial nerve palsy, or mortality.
Studies without a comparator group, those investigating only one surgical technique, narrative reviews, letters to the editor, single case reports, studies lacking usable numerical data for analysis and studies not written in english were excluded. Studies with overlapping populations were carefully screened, retaining only the publication with the most complete data or the most robust methodological design. Studies exclusively involving neonatal populations or with specific secondary etiologies (e.g., post-traumatic, infectious, or neoplastic cysts) were excluded due to the lack of adequate comparability with other data.
Search Strategy
A systematic literature search was performed in the PubMed, Embase, Scopus, Web of Science, and Cochrane Library databases from their inception until March 2024. The search strategy combined free-text terms and controlled descriptors (MeSH), using the Boolean operators AND and OR. The primary terms used included: “arachnoid cyst,” “endoscopic fenestration,” “microsurgery,” “neurosurgical treatment,” among other equivalent variations. No restrictions were applied regarding language or publication date. The electronic search was complemented by a manual review of reference lists from selected studies to identify additional relevant publications.
Study Selection and Data Extraction
Study screening was performed independently by two reviewers, initially through the analysis of titles and abstracts, followed by full-text assessment of potentially eligible articles. Disagreements were resolved by consensus or by consulting a third reviewer. Data extraction was performed using a standardized spreadsheet, collecting the following information: first author, year of publication, country of origin, methodological design, number of participants per group, surgical technique used, anatomical location of the cysts, mean follow-up time, and clinical outcomes assessed.
Methodological Quality Assessment
The methodological quality of the included studies was evaluated by two independent reviewers using the Cochrane risk of bias tool (ROBINS-I), adapted for comparative observational studies.
Data Synthesis and Statistical Analysis
Statistical analysis was performed using Review Manager (RevMan) version 5.4 and R software (using the metabin() function from the meta package). Pooled effects were expressed as relative risks (RR) with 95% confidence intervals (95% CI). The choice between fixed-effects or random-effects models was based on the magnitude of statistical heterogeneity, assessed using Cochran's Q test and the I2 statistic.
For the primary outcome, referring to cyst volume reduction, eight studies (n = 441) were included, showing moderate heterogeneity (Q = 19.14; p = 0.0078; I2 = 63.4%), which justified the use of a random-effects model. Between-study variance (τ2) was estimated using the Paule-Mandel method, and confidence intervals for τ2 and τ were determined using the Q-Profile method. Additionally, Hartung-Knapp adjustment was applied to enhance the robustness of the pooled estimates. The combined relative risk for this outcome was 0.92 (95% CI: 0.77–1.10; p = 0.325), with no statistical significance.
For the secondary outcome, related to the occurrence of intracranial hematomas, twelve studies (n = 716) were included, with no significant heterogeneity (Q = 9.91; p = 0.5382; I2 = 0%), allowing the use of a fixed-effects model. The pooled relative risk was 0.61 (95% CI: 0.32–1.17; p = 0.1392). In cases with zero-event cells, a standard continuity correction of 0.5 was applied. The results were presented using forest plots and descriptive tables. A p-value <0.05 was considered statistically significant. Publication bias was visually assessed through funnel plots and statistically tested using Egger's regression method. The incidence of cranial nerve palsy was reported in ten studies (n = 29), in all of the included studies cranial nerve palsy was sporadically reported and was not correlated to the technique. No mortality was reported in all of the included studies.
Results
A total of 1,265 records were initially identified through electronic database searches. After the removal of 243 duplicates, 1,022 articles were screened by title and abstract. Of these, 976 were excluded for not meeting eligibility criteria, resulting in 46 articles selected for full-text review. Ultimately, 16 studies fulfilled all inclusion criteria and were incorporated into this systematic review and meta-analysis. The selection process is detailed in the PRISMA flow diagram ([Fig. 1]).

The 16 included studies encompassed 1,157 patients who underwent surgical treatment for intracranial arachnoid cysts, of which 596 were treated with endoscopic fenestration (experimental group) and 561 with conventional microsurgery (control group). The mean number of participants per study ranged from 15 to 93 individuals. The methodological designs were primarily retrospective cohort studies and comparative case series. The evaluated interventions included endoscopic fenestration (via transventricular or transcystic approaches) and microsurgery (craniotomy with fenestration or partial cyst resection). Most studies were conducted in Europe and Asia, reflecting a wide geographical diversity. The primary outcomes analyzed were significant cyst volume reduction (>50%) and clinical improvement, while secondary outcomes included complications such as intracranial hematomas, cranial nerve palsy, and mortality.
Detailed methodological characteristics are summarized in [Table 1], and cyst location data are presented in [Table 2]. The summary of risk of bias assement tool for non-randomized studies ROBINS-I) is described in [Table 3]
|
Author, year |
Journal |
Mean Age (years, SD) |
Follow-up time (years, SD) |
N = 1126 |
Publication Type |
Endoscopy Fenestration |
Shunt |
Microneurosurgery Fenestration |
|---|---|---|---|---|---|---|---|---|
|
Soleman et al, 2021[10] |
J Neurosurg Pediatrics |
0.51 ± 0.43 |
5.1 ± 4.6 |
35 |
Retrospective Cohort |
23 |
4 |
10 |
|
Deopujari et al, 2020[18] |
J Neurol Surg A Cent Eur Neurosurg |
14.8 |
3 |
56 |
Retrospective study |
35 |
10 |
11 |
|
Turhan et al, 2011[11] |
Childs Nerv System |
7.4 |
5.9 |
29 |
Retrospective study |
16 |
0 |
13 |
|
Choi et al, 2015[12] |
Childs Nerv System |
5.8 |
4.4 |
75 |
Retrospective study |
30 |
2 |
45 |
|
Oertel et al, 2010[17] |
Neurosurgery |
28 |
3.3 |
61 |
Retrospective Cohort |
66 |
1 |
4 |
|
Nowosławska et al, 2006[19] |
Childs Nerv System |
5.6 |
1.4 |
106 |
Retrospective study |
44 |
27 |
29 |
|
Shim et al, 2009[13] |
Childs Nerv System |
12.7 |
6.9 |
209 |
Retrospective study |
84 |
29 |
49 |
|
Duz et al, 2012[20] |
Turkish Neurosurgery |
20.02 |
2.2 |
75 |
Retrospective study |
15 |
35 |
25 |
|
Pesaresi et al, 2024[21] |
Acta Neurochirurgica |
3.2 ± 3.7 |
1 |
50 |
Retrospective study |
14 |
6 |
20 |
|
Jaradat et al, 2024[22] |
Clinical Neurology and Neurosurgery |
7.4 ± 2.8 |
1 |
39 |
Retrospective study |
11 |
20 |
8 |
|
Damaty et al, 2023[14] |
World Neurosurgery |
7.1 |
5.6 |
61 |
Retrospective study |
18 |
10 |
33 |
|
Schulz et al, 2021[23] |
J Neurosurg Pediatrics |
5.1 ± 2.3 |
1.3 |
113 |
Retrospective Cohort |
98 |
3 |
15 |
|
Masoudi et al, 2021[24] |
World Neurosurgery |
6.94 ± 8.62 |
3.7 ± 1.4 |
29 |
Retrospective study |
26 |
1 |
2 |
|
Kim et al, 2020[15] |
J Neurosurg Pediatrics |
5.2 |
7.6 |
60 |
Retrospective study |
9 |
5 |
24 |
|
Wang et al, 2013[25] |
Neurology India |
35.0 |
3.8 |
68 |
Case series |
36 |
3 |
29 |
|
Sprung et al, 2011[16] |
Acta Neurochir |
30 |
3.5 |
60 |
Clinical article |
7 |
3 |
13 |
|
Total |
– |
– |
– |
1126 |
– |
532 |
159 |
330 |
Meta-Analysis Findings
The meta-analysis for the primary outcome of cyst volume reduction included eight studies (n = 441). The significant volumetric response rate was 60.2% in patients undergoing endoscopic fenestration and 64.1% in those treated with microsurgery. The pooled relative risk was 0.92 (95% CI: 0.77–1.10; p = 0.325), indicating no statistically significant difference. Heterogeneity among studies was considered moderate (Q = 19.14; p = 0.0078; I2 = 63.4%). Between-study variance (τ2) was estimated using the Paule-Mandel method, with Hartung-Knapp adjustment applied to the confidence intervals. These results are illustrated in [Fig. 2]. Cranial nerve palsy was reported sporadically in ten studies (n = 29) and none mortality was reportes in all of the selected studies.

Postoperative Complications
With regard to postoperative complications, intracranial hematomas (predominantly subdural hygromas) were reported in 12 studies (n = 716). The overall hematoma rate was 7.6% in the endoscopic group and 13.5% in the microsurgical group, resulting in a pooled relative risk of 0.61 (95% CI: 0.32–1.17; p = 0.1392), with no statistically significant difference. Heterogeneity was negligible (Q = 9.91; p = 0.5382; I2 = 0%), allowing the use of a fixed-effects model. Cranial nerve palsy was reported sporadically, with a low incidence (<3%), precluding pooled analysis. None of the included studies reported mortality, as depicted in the forest plot ([Fig. 3]).

Descriptive Findings
In addition to quantitative outcomes, several relevant descriptive data were extracted and analyzed. The anatomical location of cysts was reported by most studies, with the middle cranial fossa being the most frequently affected region. Some authors used the Galassi classification for middle fossa cysts[10] [11] [12] [13] [14] [15] [16]; however, methodological inconsistencies precluded a unified categorization. Follow-up duration varied widely, ranging from a few months to several years, with no standardization in measurement (mean, median, or range). The need for reoperation was mentioned in multiple studies, reflecting cases of recurrence or initial treatment failure, although criteria for re-intervention were not consistently reported. No mortality was reported and CN palsy was not correlacted to any type of technique in the selected studies
In the study by Oertel et al., among 66 patients who underwent endoscopic surgery, five experienced cyst recurrence following the initial endoscopic treatment.[17] Specific complications such as subdural hygromas were occasionally associated with microsurgery, but diagnostic criteria were not uniformly defined. For example, Turhan et al. reported that 23% of patients treated with microsurgery developed postoperative complications.[11]
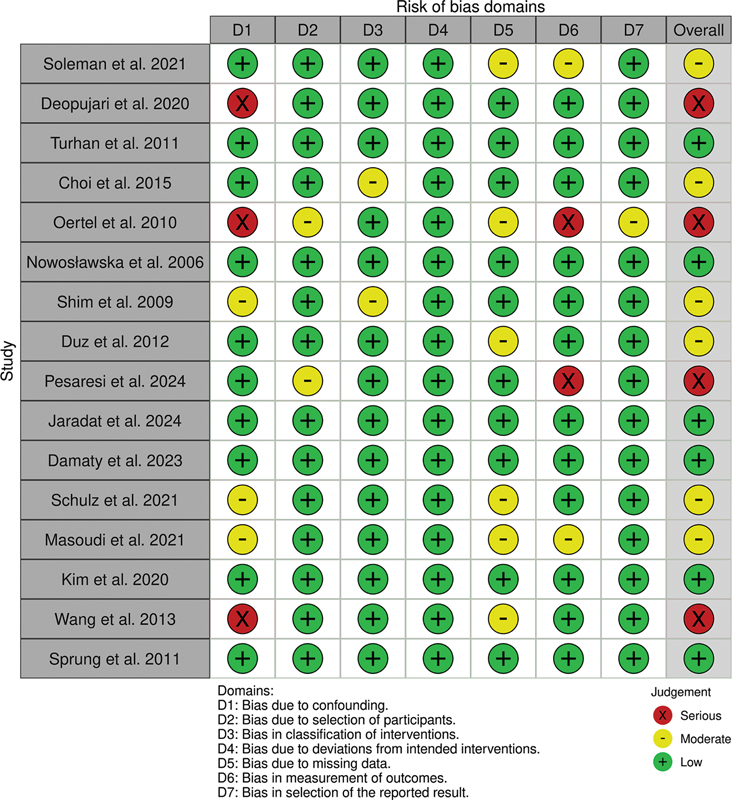
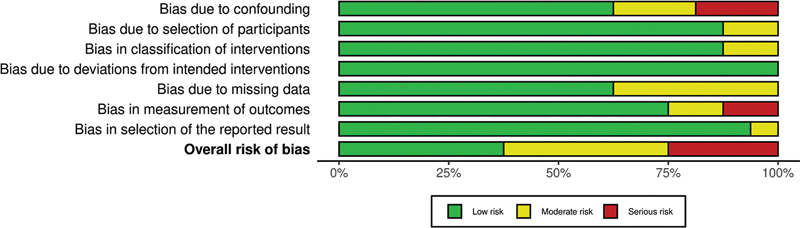
These findings highlight the need for standardized methods for collecting and reporting clinical outcomes in future studies, to enable more accurate comparisons across different surgical strategies. The risk of bias assessment for the included studies is presented in [Figs. 4] and [5], which show that while most studies exhibited a low risk of bias, the study by Oertel et al. demonstrated high risk across multiple domains.
Discussion
This meta-analysis, based on 16 studies and 1,157 patients, represents one of the most comprehensive comparisons between endoscopic fenestration and microsurgery for the treatment of intracranial arachnoid cysts to date. The data demonstrated that both techniques exhibit similar efficacy in terms of cyst volume reduction, with no statistically significant difference between the groups. Regarding postoperative complications, a favorable trend was observed for the endoscopic approach concerning the incidence of intracranial hematomas, although this difference was not statistically significant. The incidence of cranial nerve palsy was low in both groups, and none of the studies reported procedure-related mortality. These findings suggest that the two techniques are comparable in terms of efficacy and safety, allowing therapeutic choice to be guided by anatomical factors, surgeon expertise, and patient profile.
When comparing these results with previously published literature, a consistent pattern emerges, with earlier studies reporting similar clinical success rates between approaches, particularly for suprasellar, posterior fossa, and quadrigeminal cysts.[5] [6] Studies such as those conducted by Gangemi et al. demonstrated the effectiveness of endoscopic fenestration in deep ventricular regions, which corroborates the findings of the present analysis.[5] [6] Conversely, studies focusing on sylvian fissure cysts indicated more favorable outcomes with microsurgery, possibly due to the technical challenges associated with endoscopic access and the complex anatomy of this region.[7] This meta-analysis contributes a robust quantitative assessment by consolidating heterogeneous evidence under a uniform methodological framework, offering an updated synthesis of the surgical landscape.
It is important to note that the included studies exhibit methodological heterogeneity, which may influence the pooled estimates. Nonetheless, the rigorous application of advanced statistical tools (e.g., Hartung-Knapp adjustment, Paule-Mandel variance estimation) and strict adherence to PRISMA guidelines enhance the reliability of the findings.[9]
From a clinical perspective, the results reinforce that both endoscopic fenestration and microsurgery are viable and safe strategies for managing symptomatic intracranial arachnoid cysts. The choice between these techniques should consider factors such as cyst location, institutional expertise, anatomical risk, and patient preferences. Future research, ideally in the form of multicenter randomized controlled trials, should aim for standardization of outcomes, diagnostic criteria, and clinical assessment scales, thereby refining the current body of evidence. Studies with long-term follow-up and postoperative functional evaluation will be essential to support more personalized and evidence-based clinical decision-making.
Limitations
While this meta-analysis provides one of the most comprehensive comparisons between endoscopic fenestration and microsurgery for intracranial arachnoid cysts, certain inherent limitations should be considered. Most included studies were observational and retrospective, which may introduce selection bias and restrict the ability to fully account for confounding factors. Furthermore, there was moderate methodological variability, particularly regarding the definition of outcomes, imaging protocols for volumetric analysis, and follow-up duration, which may have contributed to statistical heterogeneity. Although these factors can influence pooled estimates, the application of advanced statistical techniques—including random-effects modeling, Paule-Mandel variance estimation, and Hartung-Knapp adjustments—aimed to mitigate such effects. The relatively small sample sizes in some studies and the rarity of certain complications (e.g., cranial nerve palsy and mortality) may also limit the precision of subgroup analyses. Finally, the absence of randomized controlled trials underscores the need for future prospective and multicenter studies to further strengthen the evidence base. Nonetheless, the consistency of findings across diverse cohorts and geographic regions supports the robustness of the conclusions drawn.
Conclusions
This systematic review and meta-analysis concludes that there is no statistically significant difference between endoscopic fenestration and microsurgery for the treatment of arachnoid cysts. Both techniques demonstrate comparable profiles of efficacy and safety. The choice of surgical approach should take into account factors such as cyst location, the patient's clinical condition, and the surgical team's expertise. Future studies with prospective designs and standardized clinical outcomes are recommended to strengthen the available evidence.
Conflict of Interest
The authors declare that they have no conflicts of interest to disclose.
-
References
- 1 Al-Holou WN, Terman S, Kilburg C, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in adults. J Neurosurg 2013; 118 (02) 222-231
- 2 Hall S, Smedley A, Sparrow O. et al. Natural history of intracranial arachnoid cysts. World Neurosurg 2019; 126: e1315-e1320
- 3 Reinshagen K, Katzman GL, Dagher AP, Patronas NJ. Incidental findings in MRI of asymptomatic volunteers. JAMA 1999; 282 (01) 36-39
- 4 Carbone J, Sadasivan AP. Intracranial arachnoid cysts: Review of natural history and proposed treatment algorithm. Surg Neurol Int 2021; 12: 621
- 5 Gangemi M, Seneca V, Colella G, Cioffi V, Imperato A, Maiuri F. Endoscopy versus microsurgical cyst excision and shunting for treating intracranial arachnoid cysts. J Neurosurg Pediatr 2011; 8 (02) 158-164
- 6 Gangemi M, Colella G, Magro F, Maiuri F. Suprasellar arachnoid cysts: endoscopy versus microsurgical cyst excision and shunting. Br J Neurosurg 2007; 21 (03) 276-280
- 7 Gui SB, Wang XS, Zong XY, Li CZ, Li B, Zhang YZ. Assessment of endoscopic treatment for middle cranial fossa arachnoid cysts. Childs Nerv Syst 2011; 27 (07) 1121-1128
- 8 Leite P, Andrade OÍ. Comparison between endoscopic and microsurgical fenestration for subarachnoid cysts: a systematic review and meta-analysis. PROSPERO 2025 CRD420251149264. Published 2025. Accessed September 17, 2025. https://www.crd.york.ac.uk/PROSPERO/view/CRD420251149264
- 9 Page MJ, McKenzie JE, Bossuyt PM. et al. statement: an updated guideline for reporting systematic reviews. BMJ 2020; 2021 (71)
- 10 Soleman J, Schmid K, Kamenova M, Guzman R, Mariani L, Soleman J. Neuroendoscopic treatment of intracranial arachnoid cysts in children: clinical and radiological outcome. J Neurosurg Pediatr 2021; 28 (05) 544-552
- 11 Turhan T, Ersahin Y, Mutluer S. Endoscopic treatment of intracranial arachnoid cysts in children. Childs Nerv Syst 2012; 28 (02) 229-235
- 12 Choi JU, Kim DS, Huh R. Endoscopic approach to arachnoid cysts. Childs Nerv Syst 2015; 31 (01) 77-86
- 13 Shim KW, Lee YH, Park EK, Park YS, Kim DS. Neuroendoscopic fenestration of intracranial arachnoid cysts: a review of 84 cases. Childs Nerv Syst 2009; 25 (11) 1459-1466
- 14 Damaty A, Oertel JM, Baldauf J. et al. Endoscopic and microsurgical treatment of arachnoid cysts: a comparative study. World Neurosurg X 2023; 19: 100195
- 15 Kim SK, Cho BK, Chung YN. et al. Neuroendoscopic fenestration for arachnoid cysts in children. J Neurosurg Pediatr 2020; 26 (03) 221-227
- 16 Sprung C, Wimmer C, Fellner FA. et al. Endoscopic versus microsurgical treatment of arachnoid cysts: a comparative study. Acta Neurochir (Wien) 2011; 153 (01) 75-84
- 17 Oertel JM, Wagner W, Mondorf Y, Baldauf J, Schroeder HW, Gaab MR. Endoscopic treatment of arachnoid cysts: a detailed account of surgical techniques and results. Neurosurgery 2010; 67 (03) 824-836
- 18 Deopujari CE, Karmarkar VS, Shaikh ST, Manglani KV. Neuroendoscopic management of intracranial arachnoid cysts: a series of 35 cases. J Neurol Surg A Cent Eur Neurosurg 2021; 82 (01) 43-52
- 19 Nowosławska E, Polis L, Kaniewska D, Bonicki W, Roszkowski M. Neuroendoscopic treatment of arachnoid cysts in children. Childs Nerv Syst 2006; 22 (06) 599-604
- 20 Duz B, Gocmen S, Secer HI, Bas NS, Gonul E. The surgical management of intracranial arachnoid cysts in adults. Turk Neurosurg 2012; 22 (05) 622-628
- 21 Pesaresi A, Taddei G, Forcato S. et al. Endoscopic treatment of middle cranial fossa arachnoid cysts: long-term results and literature review. Acta Neurochir (Wien) 2024; 166: 428-437
- 22 Jaradat M, Abdel-Razeq R, Al Nuaimi H. et al. Surgical management of intracranial arachnoid cysts: outcomes of endoscopic fenestration and microsurgery. Clin Neurol Neurosurg 2024; 242: 108317
- 23 Schulz M, Goelz L, Hopf NJ. Long-term results of endoscopic treatment of intracranial arachnoid cysts in children. J Neurosurg Pediatr 2021; 28 (01) 102-112
- 24 Masoudi MS, Shafiee A, Aghamohammadi M. et al. Endoscopic fenestration versus open microsurgical treatment of intracranial arachnoid cysts: a comparative study. World Neurosurg 2021; 149: e30-e40
- 25 Wang Y, Wang L, Wang H. et al. Management of intracranial arachnoid cysts: experience with 68 cases. Neurol India 2013; 61 (01) 35-40
Address for correspondence
Publication History
Received: 20 September 2025
Accepted: 10 November 2025
Article published online:
29 December 2025
© 2025. Sociedade Brasileira de Neurocirurgia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua Rego Freitas, 175, loja 1, República, São Paulo, SP, CEP 01220-010, Brazil
-
References
- 1 Al-Holou WN, Terman S, Kilburg C, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in adults. J Neurosurg 2013; 118 (02) 222-231
- 2 Hall S, Smedley A, Sparrow O. et al. Natural history of intracranial arachnoid cysts. World Neurosurg 2019; 126: e1315-e1320
- 3 Reinshagen K, Katzman GL, Dagher AP, Patronas NJ. Incidental findings in MRI of asymptomatic volunteers. JAMA 1999; 282 (01) 36-39
- 4 Carbone J, Sadasivan AP. Intracranial arachnoid cysts: Review of natural history and proposed treatment algorithm. Surg Neurol Int 2021; 12: 621
- 5 Gangemi M, Seneca V, Colella G, Cioffi V, Imperato A, Maiuri F. Endoscopy versus microsurgical cyst excision and shunting for treating intracranial arachnoid cysts. J Neurosurg Pediatr 2011; 8 (02) 158-164
- 6 Gangemi M, Colella G, Magro F, Maiuri F. Suprasellar arachnoid cysts: endoscopy versus microsurgical cyst excision and shunting. Br J Neurosurg 2007; 21 (03) 276-280
- 7 Gui SB, Wang XS, Zong XY, Li CZ, Li B, Zhang YZ. Assessment of endoscopic treatment for middle cranial fossa arachnoid cysts. Childs Nerv Syst 2011; 27 (07) 1121-1128
- 8 Leite P, Andrade OÍ. Comparison between endoscopic and microsurgical fenestration for subarachnoid cysts: a systematic review and meta-analysis. PROSPERO 2025 CRD420251149264. Published 2025. Accessed September 17, 2025. https://www.crd.york.ac.uk/PROSPERO/view/CRD420251149264
- 9 Page MJ, McKenzie JE, Bossuyt PM. et al. statement: an updated guideline for reporting systematic reviews. BMJ 2020; 2021 (71)
- 10 Soleman J, Schmid K, Kamenova M, Guzman R, Mariani L, Soleman J. Neuroendoscopic treatment of intracranial arachnoid cysts in children: clinical and radiological outcome. J Neurosurg Pediatr 2021; 28 (05) 544-552
- 11 Turhan T, Ersahin Y, Mutluer S. Endoscopic treatment of intracranial arachnoid cysts in children. Childs Nerv Syst 2012; 28 (02) 229-235
- 12 Choi JU, Kim DS, Huh R. Endoscopic approach to arachnoid cysts. Childs Nerv Syst 2015; 31 (01) 77-86
- 13 Shim KW, Lee YH, Park EK, Park YS, Kim DS. Neuroendoscopic fenestration of intracranial arachnoid cysts: a review of 84 cases. Childs Nerv Syst 2009; 25 (11) 1459-1466
- 14 Damaty A, Oertel JM, Baldauf J. et al. Endoscopic and microsurgical treatment of arachnoid cysts: a comparative study. World Neurosurg X 2023; 19: 100195
- 15 Kim SK, Cho BK, Chung YN. et al. Neuroendoscopic fenestration for arachnoid cysts in children. J Neurosurg Pediatr 2020; 26 (03) 221-227
- 16 Sprung C, Wimmer C, Fellner FA. et al. Endoscopic versus microsurgical treatment of arachnoid cysts: a comparative study. Acta Neurochir (Wien) 2011; 153 (01) 75-84
- 17 Oertel JM, Wagner W, Mondorf Y, Baldauf J, Schroeder HW, Gaab MR. Endoscopic treatment of arachnoid cysts: a detailed account of surgical techniques and results. Neurosurgery 2010; 67 (03) 824-836
- 18 Deopujari CE, Karmarkar VS, Shaikh ST, Manglani KV. Neuroendoscopic management of intracranial arachnoid cysts: a series of 35 cases. J Neurol Surg A Cent Eur Neurosurg 2021; 82 (01) 43-52
- 19 Nowosławska E, Polis L, Kaniewska D, Bonicki W, Roszkowski M. Neuroendoscopic treatment of arachnoid cysts in children. Childs Nerv Syst 2006; 22 (06) 599-604
- 20 Duz B, Gocmen S, Secer HI, Bas NS, Gonul E. The surgical management of intracranial arachnoid cysts in adults. Turk Neurosurg 2012; 22 (05) 622-628
- 21 Pesaresi A, Taddei G, Forcato S. et al. Endoscopic treatment of middle cranial fossa arachnoid cysts: long-term results and literature review. Acta Neurochir (Wien) 2024; 166: 428-437
- 22 Jaradat M, Abdel-Razeq R, Al Nuaimi H. et al. Surgical management of intracranial arachnoid cysts: outcomes of endoscopic fenestration and microsurgery. Clin Neurol Neurosurg 2024; 242: 108317
- 23 Schulz M, Goelz L, Hopf NJ. Long-term results of endoscopic treatment of intracranial arachnoid cysts in children. J Neurosurg Pediatr 2021; 28 (01) 102-112
- 24 Masoudi MS, Shafiee A, Aghamohammadi M. et al. Endoscopic fenestration versus open microsurgical treatment of intracranial arachnoid cysts: a comparative study. World Neurosurg 2021; 149: e30-e40
- 25 Wang Y, Wang L, Wang H. et al. Management of intracranial arachnoid cysts: experience with 68 cases. Neurol India 2013; 61 (01) 35-40