

Subscribe to RSS
DOI: 10.1055/s-0045-1813704
Imaging in Carcinoma Cervix Staging, Follow-up, and Surveillance: A Review
Authors


Abstract
Cervical cancer is a significant health concern globally and is the second most common cancer among women in India. Progress in awareness, hygiene, healthcare infrastructure, and interventions has led to decreasing incidence and mortality rates of cervical cancer, but remains alarmingly high, where delayed presentation is the most common reason. Until recently, cervical cancer was staged clinically with minimal investigations like ultrasonography (USG) and cystoscopy, leading to suboptimal evaluation and staging. In 2018, FIGO incorporated ‘Imaging’ for staging of cervical cancer to accurately delineate disease for treatment planning, further validated by the 2021 update. USG is often the first imaging test utilized, while magnetic resonance imaging (MRI) is the imaging modality of choice to delineate disease extent. It has the highest specificity, sensitivity, and accuracy in detecting the parametrial and stromal invasion. MRI is also used for treatment planning and response assessment. Contrast-enhanced computed tomography and positron emission tomography scans are reserved for distant staging. This review article aims to discuss the role of imaging in diagnosis, pretreatment staging, treatment planning, and surveillance.
Keywords
transvaginal USG - cervical cancer - dynamic contrast-enhanced MRI - FIGO - multiparametric MRI - staging imagingIntroduction
India accounts for approximately one-fifth of the global burden of cervical cancer, the second most common cancer among women, with high mortality, but with a declining trend.[1]
Adenocarcinoma and squamous cell carcinoma make up 25 and 70% of cervical cancer, respectively.[2] Adenosarcomas, adenosquamous carcinoma, adenoid cystic carcinoma, small-cell carcinoma, and lymphoma comprise 5%. Human papillomavirus genotypes 16 and 18 are linked to cervical cancer, are the main targets of vaccination.[2]
The ectocervix is lined by stratified squamous epithelium, and the endocervical canal by columnar epithelium. Metaplasia at this squamocolumnar junction results in squamous cell carcinoma. Its location varies with age and hormonal status; being near the external os in young, and receding superiorly into the endocervix with age, explaining why exophytic tumors are common in young women and endocervical tumors in older women.[3]
Improved disease control is seen with earlier-stage presentation and with advances in treatment. Imaging sets its place in appropriate staging, as management and its successful outcome are a direct measure of accurate staging.
FIGO 2009 staging was based essentially on clinical examination. Imaging did not have any role; thus, craniocaudal extension of tumor, parametrial involvement, and lymph node assessment were not possible, leading to inaccurate disease mapping, affecting prognostication and treatment outcomes.[4] [5] Accurate assessment of these is crucial for determining optimal therapeutic approaches, such as radiotherapy (RT), neoadjuvant chemotherapy, and surgery. Hence, imaging (ultrasonography [USG], computed tomography [CT], magnetic resonance imaging [MRI], and positron emission tomography [PET]-CT) and pathology assessments were incorporated in the revised FIGO staging system (2018) of cervical cancer[6] and enforced in the 2021 update to complement clinical evaluation.
Cervical cancer is more prevalent in a lower socioeconomic background, with poor availability of adequate health infrastructure. The 2018 update recognized the role of USG as an alternative primary imaging modality, particularly in low-resource countries, depending on the availability of equipment and expertise, with MRI being the primary imaging modality of choice wherever available.[7]
Imaging (USG and cross-sectional) plays a mainstay in staging of cervical cancer, determining craniocaudal extent of the lesion, depth of stromal invasion, parametrial invasion, pelvic sidewall, vagina, rectal/bladder involvement, and lymph node metastasis. With excellent soft tissue imaging characteristics, MRI additionally assists in planning and delivery of RT, in response assessment, and surveillance.
Role of Ultrasound
The diagnostic potential of USG was underestimated until recently, wherein it was reserved for screening of hydroureteronephrosis, a surrogate of lateral pelvic wall involvement. However, technological developments, especially endovaginal high-resolution probes, provide a wide field of view, depict detailed pelvic anatomy, yielding comparable results as MRI, with again a growing interest in using USG for diagnosis and preoperative staging of cervical cancer[6] [7] ([Fig. 1]).
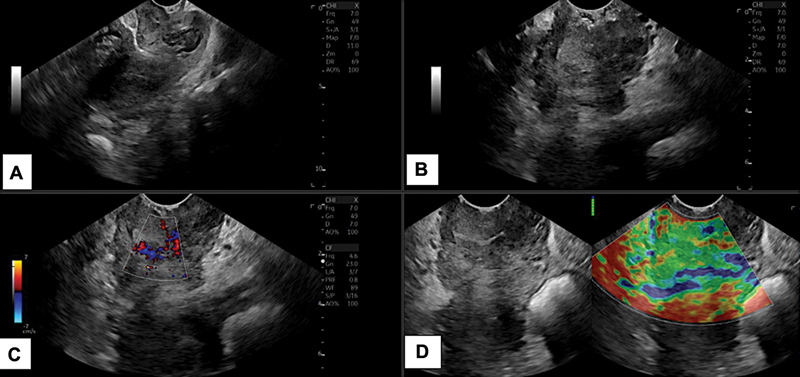
The endovaginal probe can be used transvaginally (TVS) or transrectally (TRUS) to detect, diagnose, stage, and offer a route for biopsy sampling. TRUS is preferred due to the decreased risk of bleeding from the tumor, and it allows better acoustics to visualize the distal cervix[7] ([Fig. 2]). It can determine the size, stromal invasion, and infiltration into the pericervical fascia, parametrium, bladder/rectum, as well as assess pelvic vasculature and muscles. 3D USG offers multiplanar coronal imaging similar to MRI.[7] It can determine eligibility for a fertility-sparing approach by providing accurate distance from the tumor to the cervical canal, estimating remaining length after conization. In the future, intraoperative US could assist a surgeon by ensuring tumor-free cervix length for women desiring pregnancy by determining the level of excision during conization.[6]

TVS Doppler enables tumor angiogenesis-related vascularity, with prediction of clinical response to definitive/neoadjuvant chemoradiation in patients with locally advanced cervical cancer.[7] TVS elastography explores the assessment of parametrial infiltration, staging, and predicting chemoradiotherapy treatment response in terms of differential increase in tissue stiffness. Transabdominal USG, in addition to hydroureteronephrosis, can detect parenchymal, retroperitoneal, and pelvic lymph nodal metastases, although at a lower sensitivity than cross-sectional imaging.[7]
Radiological Anatomy of Cervix
The cervix is a cylindrical, 3- to 4-cm-long structure made up of epithelium and stroma. Through the internal and external os, respectively, the endocervical canal is connected to the uterine cavity superiorly and the vagina inferiorly.[3]
Cervix on T2-weighted (W) shows four distinct zones from inside ([Fig. 3]):

-
Zone 1: central higher signal intensity (SI) mucous secretion in the cervical canal.
-
Zone 2: high SI endocervical mucosa.
-
Zone 3: hypointense fibrous stroma
-
Zone 4: outer intermediate SI of loose stroma.
The cervix is seen as an intermediate SI structure on T1W images, without clear demarcation of its zonal anatomy.[8]
Planning of MRI
A well planned and well acquired study is of utmost importance in improving diagnostic accuracy. [Table 1] refers to multiparamtric MRI protocol for cervical imaging.
Large field of view (FOV) T1W and T2W in true axial plane covering abdomen and pelvis for a global view of the abdomen and pelvic anatomy. Pertinent assessment in cervical cancer includes retroperitoneal, pelvic adenopathy, hydroureteronephrosis, and distant metastases.
Small FOV T2W offers improved spatial resolution and soft tissue characterization.
Sagittal images depict the craniocaudal extent of the tumor and its extension into the uterus and vagina. This important parameter was non-evaluable previously when imaging was not a part of staging, particularly in endophytic masses not visible on per speculum examination. Also assess anterior and posterior forniceal, vaginal, bladder, and bowel wall involvement.
Oblique coronal and oblique axial images are acquired in planes parallel and perpendicular to the longitudinal axis of the cervix ([Fig. 4]) or to the long axis of the tumor in cases where normal cervical anatomy is distorted or lost. Axial images assess lateral, anterior, and posterior parametrium; lateral pelvic wall; bladder; and bowel wall involvement, with nodal assessment.

Functional characteristics of the tumor are evaluated on diffusion-weighted imaging (DWI) and subtracted dynamic contrast-enhanced (sDCE)-MRI.
The incorporation of DWI with T2W imaging is referred to as “biparametric MRI.” Coupled appearance of tumor exhibiting high SI on high b-value (800–1,000 s/mm2) images and correspondingly low SI on ADC is called restricted diffusion, based on the cellularity of tumor, with greater restriction favoring malignancy. It assists T2W imaging, where T2 falls short in delineating edema from disease and locoregional infiltration. Ghardon et al stated that the range for ADC varies in the literature from 0.62 to 1.11 × 10−3 mm2/sec.”[9]
Further incorporation of sDCE-MRI is referred to as multiparametric MRI. We do not recommend sDCE in all patients, but reserve it for equivocal cases of parametrial infiltration, in the absence of metastatic pelvic nodes, where sequential arterial and venous enhancement of the parametrial vascular plexus helps delineate tumor spiculation versus vasculature-related linear abnormalities at the tumor parametrial interface, to decide on surgical intervention. It is useful for the evaluation of the depth of stromal invasion and bladder wall invasion, to differentiate from bullous edema. sDCE also helps distinguish tumor recurrence from post-treatment changes.[10] [11]
After administering a gadolinium-based contrast agent, multiple images are obtained in DCE-MRI. Cervical tumors enhance rapidly in the early arterial phase (30 seconds post-contrast) before becoming hypointense to the gradually enhancing normal cervix in the late venous phase (2 minutes post-contrast).[12] [13]
Revised FIGO Classification (2018) with 2021 Update:
Inclusion of optional cross-sectional imaging, wherever available in FIGO 2018 and updated in 2021, is a key change in appropriate staging.
Staging is based on the pattern of spread of cervical cancer, confined to and beyond the uterus, vagina, parametrium, lateral pelvic wall, bladder, rectum, and adjacent organs. It spreads to pelvic and para-aortic lymph nodes via lymphatic dissemination; hematogenous dissemination can also occur to distant organs—lungs, liver, and bones.[3]
Precise cancer staging plays a pivotal role in determining prognosis, offering accurate staging for appropriate stage-based treatment, response assessment, and evaluation for recurrence/residual disease. Uniformity in planning acquisition and standardized synoptic reporting provides reliable comparison and paves the way for easier communication with treating oncophysicians.[7]
Cervical cancer appears as T2 intermediate SI, not appreciable on T1W images, shows restricted diffusion on DWI, and shows early enhancement with early washout on DCE, compared to the rest of the normal cervical tissue.
FIGO cervical cancer staging[14] is as follows:
-
Stage I: Tumor confined to cervix.
-
IA: microscopic disease, not evaluable on MRI.
-
IB: invasive carcinoma with deepest invasion ≥5 mm.
-
○ IB1: <2 cm in maximum dimension.
-
○ IB2: ≥2 cm and <4 cm in maximum dimension.
-
○ IB3: ≥4 cm in maximum dimension.
-
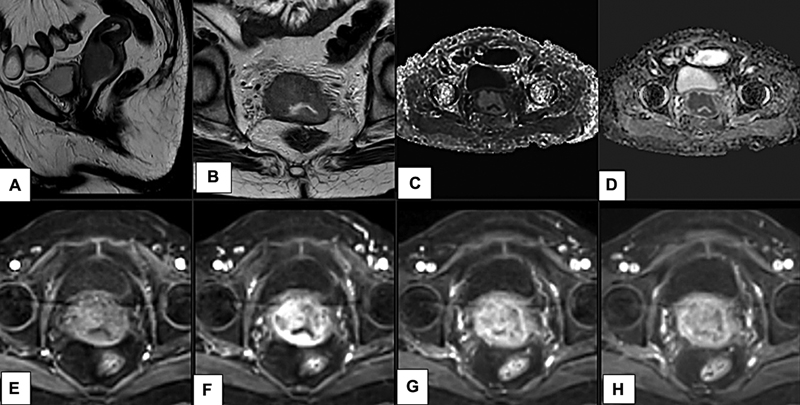
These lesions show intermediate SI compared to cervical stroma. The T2-hypointense rim of cervical stroma is preserved, indicating the T2-hypointense “cervical rim sign.” It excludes parametrial invasion ([Figs. 5] and [6]).


-
Stage II: Invasion beyond the uterus but not to the pelvic side walls/lower third vagina.
-
IIA: Upper two-thirds of vagina, without parametrial invasion.
On MRI, it is seen as a disruption of low SI vaginal wall/fornix by intermediate tumor SI ([Figs. 7] and [8]). The vagina is divided into three parts: upper, mid, and lower, according to its length.


This is further divided based on the maximum dimension of the tumor:
-
○ IIA1: tumor <4 cm.
-
○ IIA2: tumor ≥4 cm.
-
IIB: Tumor invades the parametrium without reaching up to the pelvic wall (limited/medial parametrial invasion).
Parametrium is divided into three parts: medial, mid, and lateral thirds. Extension to the medial third is referred to as limited parametrial invasion.
On MRI, it is seen as a disruption of the outer T2-hypointense cervical stroma with tumor extending into the parametrium ([Fig. 9]). It is seen as a spiculated tumor–parametrial interface ([Fig. 10]), extension along the uterine ligaments, or as encasement of periuterine vessels and retraction of cervix to the side of invaded parametrium.


Large tumors may exhibit challenges in differentiating peritumoral edema or engorged vascularity from neoplastic parametrial invasion on T2W images. Correlation with DWI and sDCE often assists in better evaluation in such cases. This precision is essential as the presence or absence of parametrial infiltration is a pivotal change in management from surgery to radiation therapy ([Fig. 10]).
-
Stage III: Tumor extends to the pelvic sidewall and/or involves the lower one-third of the vagina and/or causes hydronephrosis/non-functioning kidney and/or involves pelvic/para-aortic nodes.
-
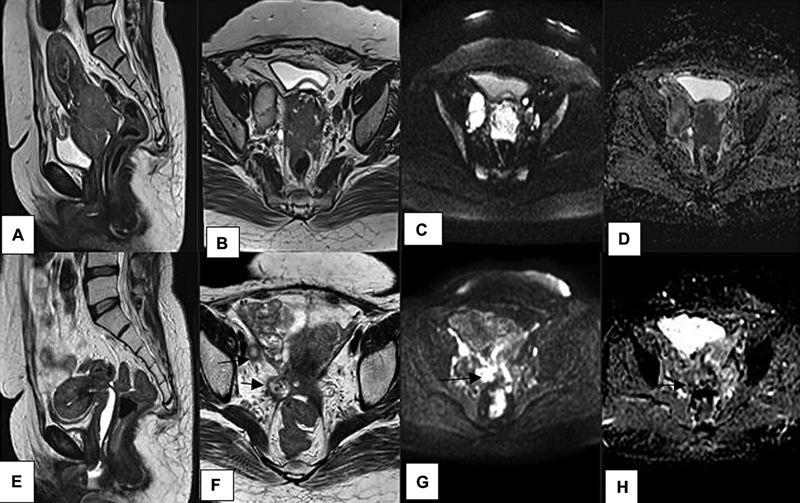
IIIA: lower one-third of vagina involved without pelvic wall invasion. On MRI, there is loss of lower SI of the vaginal wall, intermediate signal extending into the lower third ([Fig. 11]).
-
IIIB: tumor involves pelvic sidewalls (beyond the limited parametrium) or causes hydronephrosis/nonfunctioning kidney.[2] On MRI, seen as:
-
○ Tumor infiltrating pelvic muscles and cardinal ligaments.
-
○ Presence of tumor within 3 mm of the internal obturator, levator ani, pyriformis muscles, or iliac vessels.
-
○ Infiltration into distal ureters with/without proximal hydroureteronephrosis ([Fig. 11]).
-
-
IIIC: involvement of pelvic and/or paraaortic lymph nodes, irrespective of tumor size and extent:
-
○ IIIC1: pelvic lymph node metastasis only ([Fig. 12]).
-
○ IIIC2: para-aortic lymph node metastasis.
-


Stage IV: tumor extends outside the true pelvis or invades bladder/rectal mucosa.
IVA: tumor invades the rectal or vesical mucosa:
On MRI, bladder wall thickening is observed with disruption of the normal T2 hypointense signal, and tumor nodules protrude into the bladder or rectal lumen ([Fig. 13]). Owing to the bare surface of the bladder posteriorly, bladder invasion is more common than rectal invasion. Contiguous involvement of the bladder/rectum with loss of fat planes indicates serosal involvement.

MRI has a high negative predictive value of 100% in assessing bladder and rectal invasion[8] and offers more information than endoscopic examination.[7] Woo et al state, “The pooled specificity and sensitivity of MRI in detecting bladder wall infiltration as 95% and 84%, respectively.”[15]
Bullous edema of the bladder ([Fig. 14]) suggests a nonspecific reaction without definite invasion. The thickened posterior bladder wall with high SI on T2W shows poor enhancement of the central wall, against the homogenous mucosal and serosal enhancement.
Stage IVB: distant metastases
Tumor involving organs outside the true pelvis. Zhou and Peng stated that single-site metastasis accounts for 68.7%, while multiorgan metastases are relatively rare. Lung (37.9%) was the most common, followed by bone (16.7%) and liver (12.5%). Brain metastases are uncommon, accounting for 1.6%.[16] Pulmonary metastases are more likely to cavitate in squamous cell cervical cancer.
Lymph Node Evaluation
Cervical cancer follows the lymphatic drainage of the cervix. The risk of nodal metastases is proportional to tumor size, depth of stromal invasion, lymphovascular invasion, and parametrial disease.[17] [18] [19]

MRI helps in the assessment of the size and morphology of nodes. Involved nodes have a round shape, central necrosis, short-axis diameter of >10 mm, and perinodal infiltration ([Fig. 12]).
Node-RADS has different size criteria for lymph nodes depending on the regions. Generally, LNs with a short axis larger than 10 mm were considered enlarged; this is true for para-aortic, common iliac, and internal iliac nodes. However, for obturator nodes, a short axis of more than 5 mm is considered enlarged, while for the inguinal region, a short axis greater than 15 mm is considered enlarged.[20]
Necrosis is seen as small areas of T2-hyperintense SI. Similar to primary disease, DWI and DCE also have a role, but they are unable to identify micrometastases in nodes of normal size, and reactive enlargement can happen without malignant involvement.
The size criterion may be overruled by suspicious morphological patterns for accurate staging. Doubtful cases can be considered for fine needle aspiration cytology.
Role of CT and PET-CT
CT scans have a poorer inherent gray-scale evaluation for evaluating the cervix, where its zones and early lesions are not well demarcated; hence, CT is not recommended for this purpose. Larger masses with contoural changes, obvious parametrial infiltration, and with unequivocal uterine and cervical involvement are well visualized. In advanced cases, CT detects bladder invasion, with 100% sensitivity and 92% specificity. In a systematic review, Bipat et al stated that “MRI was not significantly better than CT in the detection of bladder and rectal invasion.[21]
ESGO/ESTRO/ESP Guidelines (update 2023) recommend “CT or PET-CT for detecting lymph node metastases and distant spread in locally advanced disease or in early-stage disease with suspicious lymph nodes on imaging.”[7]
Choi et al stated[22] that CT has overall inferior diagnostic performance compared to PET, PET-CT, or MRI in identifying metastatic lymph nodes. Also stated by Olthof et al, “FDG-PET-CT outperforms MRI and CT in detecting nodal metastases. As MRI is routinely used to assess local and regional spread of cervical cancer, FDG-PET-CT can be used to confirm suspicious lymph nodes.”[17] Although there are no international protocols available, lymph nodes are considered suspicious when they have morphological tumor features, a short-axis diameter > 10 mm, and increased FDG uptake with SUV >2.5 or more than the adjacent vessel.[17]
Initially, CT was the only modality used for the RT planning. However, with the advent of MRI and PET-CT, these are now frequently employed as well—MRI providing the improved resolution and tumor delineation, and PET integrating the metabolic information with the anatomical details. Nevertheless, CT remains the sole 3D imaging modality used for dose calculations.[23]
Diagnosis and Importance of Accurate Staging and Treatment
Cervical cancer detection is not challenging due to the organ anatomy providing direct visual access on per speculum examination with the feasibility of histopathological correlation in the outpatient department, primary health center, or screening by tests such as visual acetic acid and Papanicolaou smear examination/LBC.
At our institute, after a pre-vaginal examination and local diagnosis, MRI is performed for locoregional assessment to determine whether surgical treatment is feasible or if RT planning is required. The primary imaging modality is the MRI, usually a biparametric MRI. Multiparametric MRI is done depending on the clinical history, examination findings, and evaluation of the noncontrast sequences, if there is a need for assessment of the parametrium/early organ invasion.
For advanced cases, staging is preferably performed using CT and PET-CT. For cervical cancer management, imaging holds greater strength in staging than diagnosis. [Table 2] compares the different available imaging modalities for cervical imaging and staging. Staging is driven by the anatomical extension of disease, which determines prognostication. Advances in therapeutic management have resulted in stage-based reductions in morbidity and mortality. Surgery, radiation therapy, chemotherapy, and immunotherapy form pillars of management of cervical cancer, and each of these has a dedicated indication and protocol that is based on staging.
Clinical examination alone can understage disease. Surgery in higher stages is associated with greater morbidity without survival benefits; thus, imaging paved its way into the FIGO classification, not only to stage disease, but also to decide the therapy planning and surveillance. Cervical cancer treatment includes surgery and/or radical RT with adjuvant chemotherapy, depending on its stage.[24] [25] Treatment depends on the stage of disease, the patient's performance status, and preference.
Cervical conization is recommended for IA1 disease without LVSI.[25] For FIGO stage IA1 with LVSI, 1A2, IB1 with < 2 cm tumor size, and no involvement of the internal os, trachelectomy is the procedure of choice. This approach allows preservation of the ovaries --avoiding early menopause --maintains sexual function, making it a preferred option for young women.[25] [26]
In early invasive tumors (IB1 and IIA1), the standard of care is either surgery or RT, with equivalent survival. The standard protocol is to proceed with bilateral pelvic lymphadenectomy at the start of the procedure and assess nodes by frozen section. If negative, surgical resection is performed, depending on the patient's fertility desire and stage of disease. If nodes are positive, surgery is abandoned, and concurrent chemoradiation is given. This approach prevents the dual added morbidity of radiation and surgery.[24] [25]
Tumors >4 cm are considered for radical hysterectomy. The decision regarding adjuvant therapy is a risk-adapted approach based on the final histopathology report and imaging features.[25]
Low-risk patients—defined as those with the absence of both intermediate and high-risk features—require no further adjuvant treatment.
In patients with any two intermediate-risk factors, including lymphovascular stromal invasion, deep cervical stromal invasion, tumor size >4 cm with the absence of high-risk features, adjuvant RT is recommended.
In patients with any high-risk characteristics, such as positive surgical margins, positive lymph nodes, or parametrial involvement, adjuvant chemoradiotherapy with concurrent cisplatin is recommended.[25] Tumors >4 cm and with internal os involvement are associated with increased risk of lymph node metastases.[27]
Patients with advanced stages are treated with radical chemoradiation, where surgery is not feasible due to the patients' health condition or the tumor has unfavorable characteristics. The disease is managed nonsurgically by giving chemoradiation therapy.
For preoperative imaging, a systematic checklist is necessary for staging and to predict characteristics pertinent to personalized treatment planning.
Imaging Checklist
-
➢ Site and morphology: anterior ([Fig. 5])/posterior lip.
Polypoidal ([Fig. 6])/plaque-like thickening, endoexophytic, partly circumferential/circumferential, or infiltrative. This allows mapping volume and location of the tumor, helping in surgical management and RT planning.
-
➢ Size
Tumor size plays a crucial role in treatment decisions and prognostication. The lesion should be measured in all three orthogonal planes, as FIGO is based on the maximum tumor size in any of the planes.
The earliest detectable stage on imaging is Stage IB.[3] [24] Detection of small lesions requires multiparametric MRI, as they may be occult on the T2W sequence, but may show restricted diffusion on DWI and early enhancement on DCE.
Trachelectomy is an option in stage ≤ IB1 and distance of >5 mm from the internal os, to preserve fertility.[3] [25] As there is an increased incidence of lymph node involvement and extrauterine spread with large tumors, patients with tumor size ≥ 4 cm, and FIGO IB2-IIA or more undergo chemoradiation rather than radical surgery.[3] [25]
-
➢ Stromal involvement: Less than 50% or more than 50%.
-
➢ Vaginal involvement: Involvement of the upper two-thirds or extension to the lower one-third of the vagina changes staging and prognostication. A horizontal line at the level of the bladder neck divides the vagina into the upper two-thirds and the lower one-third.[2] [28]
It is usually seen as a contiguous spread, while sometimes macroscopic skip lesions may be seen in the lower vagina.
-
➢ Parametrial involvement and extent
Parametrial invasion precludes surgical treatment, and hence its accurate assessment is essential. MRI's accuracy for parametrial extension is 88 to 97%, which is better than that of clinical assessment.[3] [28] An intact cervical stromal ring excludes parametrial extension.[3] [29] It is categorized as IIB after it penetrates the cervical stoma and spreads into the parametrium.
It is best evaluated in axial oblique T2W, and equivocal cases will benefit from multiparametric MR including DWI and sDCE.
-
➢ Lateral pelvic wall assessment: The pelvic sidewall includes the obturator internus and the iliac bone. Cervical cancer rarely extends up to the bone. For management and RT planning, involvement within 3 mm of pelvic sidewall muscles or iliac vessels, as well as encasement of the ureter with upstream hydroureteronephrosis, is considered as lateral-wall extension.
-
➢ Bladder and bowel: MRI is highly accurate in excluding bladder/bowel invasion by depicting an intact fat plane between tumor and bladder/rectum.[3]
Disruption of the T2-hypointense wall, demonstration of intraluminal mass, or vesicovaginal/rectovaginal fistula is classified as invasion/stage IVA.
-
➢ Lymph nodes: size, site, and the level of suspicion
Assessment of lymph nodes is an important part of staging and management, as their improper treatment paves the way for recurrence. Pelvic and extrapelvic nodes need to be assessed for adjuvant chemoradiation therapy if planned for surgery. For RT planning, it is crucial to detect lymph node metastases outside the routinely applied radiation field in locally advanced disease.[7]
-
i. Location:
-
○ Pelvic: internal/external iliac, perivesical, and common iliac nodes.
-
○ Extrapelvic nodal sites: para-aortic (above/below the renal hilum) and inguinal nodes and other distant sites.
-
-
ii. Size: Suspicious nodes are indicated by a short axis diameter (SAD) of 10 mm or greater.[3] [11] This has drawbacks since small lymph nodes may have microscopic disease foci, whereas larger lymph nodes may be reactive.
-
iii. Morphology: A node displaying SI (on T2W), restricted diffusion, and heterogeneous enhancement fairly similar to the primary cervical mass may be considered suspicious. Additional criteria such as round shape, lost hilum, irregular or microlobulated margins, perinodal architectural distortion, and internal heterogeneity or central necrosis should raise suspicion.[28] [30]
Cytology correlation may be performed for a lone suspicious node, significantly changing planning,[3] [31] such as extended surgery or RT field increasing bowel toxicity. Cytology may also be performed for a single suspicious node, in an early cancer, where young fertility-preserving surgery is preferred.[32]
-
➢ Incidental findings: Gynecological, such as uterine fibroids, adenomyomatosis, and adnexal masses, or nongynecological detected findings should be added.
Role of MRI in RT Planning
Radiation therapy encompasses external beam radiotherapy followed by brachytherapy. Earlier, RT planning was based on 2D planning. It led to inadequate radiation dosage to the tumor and nearby organs, leading to increased toxicity. 3D planning with CT/MRI has widened the scope of precision RT. CT-guided planning is superior to 2D, but is less precise than MRI in terms of tumor delineation.[33]
MRI-guided brachytherapy has led to a transition from prescribing uniform dosage to point A, to targeting disease in the cervix and paracervical tissues individually, called MR image-guided adaptive brachytherapy[34] [35] [36] ([Fig. 15]). Contour delineation is performed and volumes with dosage are assigned depending on the tumor volume (GTV, HR CTV, and IR CTV).

GTV (gross tumor volume)—intermediate SI on T2W in the cervix and paracervical region, in addition to clinical examination.
High-risk clinical target volume (HR-CTV)—region around the GTV, including the whole cervix, with the highest risk of local recurrence due to residual macroscopic disease at the time of brachytherapy.
Intermediate-risk CTV (IR-CTV)—Further extension of HR-CTV with a margin of 5 to 15 mm to encompass the region at risk for microscopic residual disease. In addition to these, the organs at risk—bladder, rectum, sigmoid, and vagina—are also contoured on T2W sequences to minimize their inclusion in the radiation field.[34] [35] [36]
Posttherapy Assessment
Post-therapy assessment is done to determine complete, partial response, stable disease, progression, or recurrence. MR criteria for complete response include homogenous hypointense cervical stroma, resolution of the cervical mass, and uniform delayed post-contrast enhancement of the cervix. Post-treatment, the cervix appears contracted and fibrotic with a darker signal on T2W imaging without restricted diffusion. These should be compared with pretreatment images[3] [37] ([Fig. 16]).
In early stages where surgery is the primary treatment, imaging follow-up is dependent on the level of clinical suspicion. Post-trachelectomy, patients should be followed up with an MRI at 6 months and 1 year.[38] For FIGO stage ≥ II B and positive surgical margins, follow-up MRI is recommended every 6 months for 2 years.[39] Patients with complete regression of tumor on MRI do not need further imaging, if clinically negative.[39] [40] Advanced cervical cancer patients on chemoradiation require sequential follow-up with MRI to determine response. Residual cancer ([Fig. 16]) may be offered immediate curative salvage therapy, such as pelvic exenteration or concomitant CCRT.[41] Small-volume residual or recurrent disease can be addressed with RT.
Recurrence
Tumor recurrence can occur locally in the cervix or vaginal vault ([Fig. 17]), regionally in the parametrium or pelvic side walls ([Fig. 17]), or distantly in the lung, liver, para-aortic, or inguinal lymph nodes.[11]

Distinguishing post-treatment changes from recurrence is important. A recurrent lesion appears as a T2-intermediate, lobulated mass with diffusion restriction and heterogeneous enhancement, whereas a fibrotic scar shows low signal on T2W and lacks diffusion restriction. Post-radiation changes of edema may be encountered as T2W-intermediate SI, but will lack diffusion restriction and show poor enhancement.[42]
Complications
Post-radiation changes of bone marrow edema are seen on T2W and fat-suppressed sequences, exhibiting high SI conforming to the radiation field. Accompanying hypointense lines on T1 and T2 suggest insufficiency fractures. The sacrum is the most common site ([Fig. 18]).

Fistula formation may involve the bladder or bowel. Its occurrence is directly related to pretreatment involvement of the bladder or bowel wall. A breach in the continuity of the vaginal wall, well delineated by vaginal jelly, makes it visible. Fistulas are often occult and are better appreciated on a fat-saturated postcontrast sequence.
Future Directions
Hypoxia Imaging
Intratumor hypoxia can predict poor disease control and survival.[43] Biological information can be integrated in RT planning and target radiation-resistant regions by creating a heterogeneous dose pattern, designated as “dose painting.” PET and MRI can be used for hypoxia imaging.[44]
MRI: Functional imaging (DWI and DCE) can be used to evaluate tumor topography and intratumoral heterogeneity.
ADC values are lower in tumor than in normal tissue due to higher cellularity, with increasing values being a surrogate of response due to apoptosis and cell death.[45] These changes, early during RT, can predict tumor response.[17] [18] [19] Some studies show worse outcomes with high initial ADC values than with lower ADC values, possibly due to hypoxic necrotic areas that were radioresistant.[45]
DCE MRI shows the vascular density and perfusion characteristics of the tumor, which may predict hypoxia and radioresistance. Local tumor control and survival are predicted by changes in SI that show increasing tumor perfusion and volume change during 2 to 3 weeks of therapy.[45]
Further new imaging methods include BOLD (blood-oxygen level dependent) MRI[42] and diffusion-weighted magnetic resonance spectroscopy (MRS).[45]
PET scan: 18F-fluoromisonidazole (FMISO) accumulates in hypoxic cells, demarcating the hypoxic regions better than FDG PET and may have a promising role in better prediction and target planning.
USPIO-Based MR
Some new MR contrast agents contain ultrasmall particles of iron oxide (USPIO), taken up by normal lymph nodes (macrophages). Macrophages are displaced in metastatic nodes, thereby preventing USPIO uptake. The sensitivity of MR increased to 93% with USPIO to predict nodal metastases, which can also improve tumor conspicuity.[46] [47] [48]
PET-MRI
PET-MRI integrates metabolic data from PET and high-resolution multiplanar morphologic, functional information from MRI. Recent data suggest that FDG PET-MRI is equivalent to MRI and superior to FDG PET-CT for local staging of the primary tumor, while comparable to FDG PET-CT for nodal staging.[7] [49] [50] Fused images can improve locoregional and distant staging, with improvement in nodal assessment in a single scan.[7] [45]
Artificial Intelligence
Like in other cancers, artificial intelligence (AI) has the scope of enhancing early detection, diagnosis, accurate staging, treatment planning, and follow-up. Radiomics is a tool of AI, extracts the quantitative features from images (shape, texture, intensity), and can assist MRI and PET in segmenting tumors. Auto-contouring organs-at-risk and tumors by AI may improve precision and reduce planning time. Novel MRI-guided adaptive therapy is explored, in which the radiation dose can be adjusted based on tumor response using serial imaging.
Mimics of Cervical Cancer
Both benign and malignant diseases can mimic cervical cancer, such as cervical degenerative fibroids, complicated cysts, polyps, endometrial cancers, and bladder/rectal masses invading the cervix. Fibroids have a mottled diffusion restriction versus sheet-like restriction in cancers, and with a higher ADC value. Other benign lesions are unlikely to have restricted diffusion.
Distinguishing lower endometrial carcinoma from upper endophytic cervical lesions can be challenging, and conventional biopsy may not be sufficient. This distinction is important for differing management. Some features, as stated by Bourgioti et al in the MR scoring system, epicenter in cervix, tumor hypervascularity, and cervical stromal invasion, suggest cervical origin, whereas epicenter in endometrial cavity and myometrial invasion favor endometrial origin[11] ([Fig. 19]).

Conclusion
Imaging plays a crucial role in cervical cancer disease management. Ultrasonography may be the first and only modality available, but where cross-sectional imaging is available, routine use of MRI is highly encouraged for characterization of disease and locoregional staging. For predicted advanced disease, CECT or FDG PET-CECT may be performed for overall staging. New imaging tools will further enhance precision and guidance, revolutionizing existing standards for personalized therapy.
Conflict of Interest
None declared.
-
References
- 1 Ramamoorthy T, Kulothungan V, Sathishkumar K. et al. Burden of cervical cancer in India: estimates of years of life lost, years lived with disability and disability adjusted life years at national and subnational levels using the National Cancer Registry Programme data. Reprod Health 2024; 21 (01) 111
- 2 Chen J, Kitzing YX, Lo G. Systematic review-role of MRI in cervical cancer staging. Cancers (Basel) 2024; 16 (11) 1983
- 3 Devine CE, Viswanathan C, Faria SD, Marcal LP, Sagebiel TL. Imaging and staging of cervical cancer. Semin Ultrasound CT MRI 2019; 40 (04) 280-286
- 4 Steiner A, Narva S, Rinta-Kiikka I, Hietanen S, Hynninen J, Virtanen J. Diagnostic efficiency of whole-body 18F-FDG PET/MRI, MRI alone, and SUV and ADC values in staging of primary uterine cervical cancer. Cancer Imaging 2021; 21 (01) 16
- 5 Knoth J, Pötter R, Jürgenliemk-Schulz IM. et al. Clinical and imaging findings in cervical cancer and their impact on FIGO and TNM staging - an analysis from the EMBRACE study. Gynecol Oncol 2020; 159 (01) 136-141
- 6 Cuccu I, D'Augè TG, Tonti N. et al. Precision imaging in cervical cancer: a comprehensive approach to diagnosis and pre-treatment evaluation. Clin Exp Obstet Gynecol 2024; 51 (06) 145
- 7 Fischerova D, Frühauf F, Burgetova A, Haldorsen IS, Gatti E, Cibula D. The role of imaging in cervical cancer staging: ESGO/ESTRO/ESP guidelines (update 2023). Cancers (Basel) 2024; 16 (04) 775
- 8 Gala FB, Gala KB, Gala BM. Magnetic resonance imaging of uterine cervix: a pictorial essay. Indian J Radiol Imaging 2021; 31 (02) 454-467
- 9 Ghardon SSL, Hemida R, Borg MA, Sallam HF, Ahmed HM. Correlative study between apparent diffusion coefficient value and grading of cervical cancer. Egypt J Radiol Nucl Med 2022; 53: 170
- 10 Lakhman Y, Aherne EA, Jayaprakasam VS, Nougaret S, Reinhold C. Staging of cervical cancer: a practical approach using MRI and FDG PET. AJR Am J Roentgenol 2023; 221 (05) 633-648
- 11 Bourgioti C, Chatoupis K, Moulopoulos LA. Current imaging strategies for the evaluation of uterine cervical cancer. World J Radiol 2016; 8 (04) 342-354
- 12 Haldorsen IS, Lura N, Blaakær J, Fischerova D, Werner HMJ. What is the role of imaging at primary diagnostic work-up in uterine cervical cancer?. Curr Oncol Rep 2019; 21 (09) 77
- 13 Lucas R, Lopes Dias J, Cunha TM. Added value of diffusion-weighted MRI in detection of cervical cancer recurrence: comparison with morphologic and dynamic contrast-enhanced MRI sequences. Diagn Interv Radiol 2015; 21 (05) 368-375
- 14 Bhatla N, Berek JS, Cuello Fredes M. et al. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynaecol Obstet 2019; 145 (01) 129-135
- 15 Woo S, Atun R, Ward ZJ, Scott AM, Hricak H, Vargas HA. Diagnostic performance of conventional and advanced imaging modalities for assessing newly diagnosed cervical cancer: systematic review and meta-analysis. Eur Radiol 2020; 30 (10) 5560-5577
- 16 Zhou S, Peng F. Patterns of metastases in cervical cancer: a population-based study. Int J Clin Exp Pathol 2020; 13 (07) 1615-1623
- 17 Olthof EP, Bergink-Voorthuis BJ, Wenzel HHB. et al. Diagnostic accuracy of MRI, CT, and [18F]FDG-PET-CT in detecting lymph node metastases in clinically early-stage cervical cancer - a nationwide Dutch cohort study. Insights Imaging 2024; 15 (01) 36
- 18 Brunette LL, Bonyadlou S, Ji L. et al. Predictive value of FDG PET/CT to detect lymph node metastases in cervical cancer. Clin Nucl Med 2018; 43 (11) 793-801
- 19 Meng X, Song S, Li K. et al. Application of CT in predicting lymph node metastasis in cervical cancer and construction of a preoperative nomogram. Sci Rep 2025; 15 (01) 11674
- 20 Wu Q, Lou J, Liu J. et al. Performance of node reporting and data system (node-RADS): a preliminary study in cervical cancer. BMC Med Imaging 2024; 24 (01) 28
- 21 Bipat S, Glas AS, van der Velden J, Zwinderman AH, Bossuyt PM, Stoker J. Computed tomography and magnetic resonance imaging in staging of uterine cervical carcinoma: a systematic review. Gynecol Oncol 2003; 91 (01) 59-66
- 22 Choi HJ, Ju W, Myung SK, Kim Y. Diagnostic performance of computer tomography, magnetic resonance imaging, and positron emission tomography or positron emission tomography/computer tomography for detection of metastatic lymph nodes in patients with cervical cancer: meta-analysis. Cancer Sci 2010; 101 (06) 1471-1479
- 23 Pereira GC, Traughber M, Muzic Jr RF. The role of imaging in radiation therapy planning: past, present, and future. BioMed Res Int 2014; 2014: 231090
- 24 Popat P, Maheshwari A, Manchanda S. et al. Imaging recommendations for diagnosis, staging, and management of cervical cancer. Indian J Med Paediatr Oncol 2023; 44: 119-129
- 25 Mahantshetty U, Deodhar K, Modi R, Kerkar R. Cervical cancer. Tata Memorial Centre Textbook of Oncology. Springer; 2024: 777-794
- 26 Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri. Int J Gynaecol Obstet 2018; 143 (Suppl. 02) 22-36
- 27 Bourgioti C, Chatoupis K, Rodolakis A. et al. Incremental prognostic value of MRI in the staging of early cervical cancer: a prospective study and review of the literature. Clin Imaging 2016; 40 (01) 72-78
- 28 Sala E, Rockall AG, Freeman SJ, Mitchell DG, Reinhold C. The added role of MR imaging in treatment stratification of patients with gynecologic malignancies: what the radiologist needs to know. Radiology 2013; 266 (03) 717-740
- 29 Kaur H, Silverman PM, Iyer RB, Verschraegen CF, Eifel PJ, Charnsangavej C. Diagnosis, staging, and surveillance of cervical carcinoma. AJR Am J Roentgenol 2003; 180 (06) 1621-1631
- 30 Patel-Lippmann K, Robbins JB, Barroilhet L, Anderson B, Sadowski EA, Boyum J. MR imaging of cervical cancer. Magn Reson Imaging Clin N Am 2017; 25 (03) 635-649
- 31 Mitchell DG, Snyder B, Coakley F. et al. Early invasive cervical cancer: tumor delineation by magnetic resonance imaging, computed tomography, and clinical examination, verified by pathologic results, in the ACRIN 6651/GOG 183 Intergroup Study. J Clin Oncol 2006; 24 (36) 5687-5694
- 32 Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri: 2021 update. Int J Gynaecol Obstet 2021; 155 (Suppl 1, Suppl 1): 28-44
- 33 Mahantshetty U, Swamidas J, Khanna N, Engineer R, Merchant NH, Shrivastava S. Magnetic resonance image-based dose volume parameters and clinical outcome with high dose rate brachytherapy in cervical cancers – a validation of GYN GEC-ESTRO brachytherapy recommendations. Clin Oncol (R Coll Radiol) 2011; 23 (05) 376-377
- 34 Haie-Meder C, Pötter R, Van Limbergen E. et al; Gynaecological (GYN) GEC-ESTRO Working Group. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiother Oncol 2005; 74 (03) 235-245
- 35 Pötter R, Haie-Meder C, Van Limbergen E. et al; GEC ESTRO Working Group. Recommendations from gynaecological (GYN) GEC ESTRO working group (II): concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy-3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiother Oncol 2006; 78 (01) 67-77
- 36 Nag S, Gupta N. A simple method of obtaining equivalent doses for use in HDR brachytherapy. Int J Radiat Oncol Biol Phys 2000; 46 (02) 507-513
- 37 Dimopoulos JC, Petrow P, Tanderup K. et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (IV): basic principles and parameters for MR imaging within the frame of image based adaptive cervix cancer brachytherapy. Radiother Oncol 2012; 103 (01) 113-122
- 38 Balleyguier C, Sala E, Da Cunha T. et al. Staging of uterine cervical cancer with MRI: guidelines of the European Society of Urogenital Radiology. Eur Radiol 2011; 21 (05) 1102-1110
- 39 Testa AC, Di Legge A, De Blasis I. et al. Imaging techniques for the evaluation of cervical cancer. Best Pract Res Clin Obstet Gynaecol 2014; 28 (05) 741-768
- 40 Gaffney DK, Erickson-Wittmann BA, Jhingran A. et al. ACR Appropriateness Criteria® on advanced cervical cancer expert panel on radiation oncology-gynecology. Int J Radiat Oncol Biol Phys 2011; 81 (03) 609-614
- 41 Ciulla S, Celli V, Aiello AA. et al. Post treatment imaging in patients with local advanced cervical carcinoma. Front Oncol 2022; 12: 1003930
- 42 Papadopoulou I, Stewart V, Barwick TD. et al. Post-radiation therapy imaging appearances in cervical carcinoma. Radiographics 2016; 36 (02) 538-553
- 43 Skipar K, Hompland T, Lund KV. et al. MRI-guided dynamic risk assessment in cervical cancer based on tumor hypoxia at diagnosis and volume response at brachytherapy. Radiother Oncol 2024; 195: 110263
- 44 Yadav D, O'Dwyer E, Agee M, Dutruel SP, Mahajan S, Huicochea Castellanos S. Unraveling the role of PET in cervical cancer: review of current applications and future horizons. J Imaging 2025; 11 (02) 63
- 45 Fields EC, Weiss E. A practical review of magnetic resonance imaging for the evaluation and management of cervical cancer. Radiat Oncol 2016; 11: 15
- 46 Rockall AG, Sohaib SA, Harisinghani MG. et al. Diagnostic performance of nanoparticle-enhanced magnetic resonance imaging in the diagnosis of lymph node metastases in patients with endometrial and cervical cancer. J Clin Oncol 2005; 23 (12) 2813-2821
- 47 Shi Q, Pisani LJ, Lee YK. et al. Evaluation of the novel USPIO GEH121333 for MR imaging of cancer immune responses. Contrast Media Mol Imaging 2013; 8 (03) 281-288
- 48 Dappa E, Elger T, Hasenburg A, Düber C, Battista MJ, Hötker AM. The value of advanced MRI techniques in the assessment of cervical cancer: a review. Insights Imaging 2017; 8 (05) 471-481
- 49 Nie J, Zhang J, Gao J. et al. Diagnostic role of 18F-FDG PET/MRI in patients with gynecological malignancies of the pelvis: a systematic review and meta-analysis. PLoS One 2017; 12 (05) e0175401
- 50 Kim SK, Choi HJ, Park SY. et al. Additional value of MR/PET fusion compared with PET/CT in the detection of lymph node metastases in cervical cancer patients. Eur J Cancer 2009; 45 (12) 2103-2109
Address for correspondence
Publication History
Article published online:
12 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Ramamoorthy T, Kulothungan V, Sathishkumar K. et al. Burden of cervical cancer in India: estimates of years of life lost, years lived with disability and disability adjusted life years at national and subnational levels using the National Cancer Registry Programme data. Reprod Health 2024; 21 (01) 111
- 2 Chen J, Kitzing YX, Lo G. Systematic review-role of MRI in cervical cancer staging. Cancers (Basel) 2024; 16 (11) 1983
- 3 Devine CE, Viswanathan C, Faria SD, Marcal LP, Sagebiel TL. Imaging and staging of cervical cancer. Semin Ultrasound CT MRI 2019; 40 (04) 280-286
- 4 Steiner A, Narva S, Rinta-Kiikka I, Hietanen S, Hynninen J, Virtanen J. Diagnostic efficiency of whole-body 18F-FDG PET/MRI, MRI alone, and SUV and ADC values in staging of primary uterine cervical cancer. Cancer Imaging 2021; 21 (01) 16
- 5 Knoth J, Pötter R, Jürgenliemk-Schulz IM. et al. Clinical and imaging findings in cervical cancer and their impact on FIGO and TNM staging - an analysis from the EMBRACE study. Gynecol Oncol 2020; 159 (01) 136-141
- 6 Cuccu I, D'Augè TG, Tonti N. et al. Precision imaging in cervical cancer: a comprehensive approach to diagnosis and pre-treatment evaluation. Clin Exp Obstet Gynecol 2024; 51 (06) 145
- 7 Fischerova D, Frühauf F, Burgetova A, Haldorsen IS, Gatti E, Cibula D. The role of imaging in cervical cancer staging: ESGO/ESTRO/ESP guidelines (update 2023). Cancers (Basel) 2024; 16 (04) 775
- 8 Gala FB, Gala KB, Gala BM. Magnetic resonance imaging of uterine cervix: a pictorial essay. Indian J Radiol Imaging 2021; 31 (02) 454-467
- 9 Ghardon SSL, Hemida R, Borg MA, Sallam HF, Ahmed HM. Correlative study between apparent diffusion coefficient value and grading of cervical cancer. Egypt J Radiol Nucl Med 2022; 53: 170
- 10 Lakhman Y, Aherne EA, Jayaprakasam VS, Nougaret S, Reinhold C. Staging of cervical cancer: a practical approach using MRI and FDG PET. AJR Am J Roentgenol 2023; 221 (05) 633-648
- 11 Bourgioti C, Chatoupis K, Moulopoulos LA. Current imaging strategies for the evaluation of uterine cervical cancer. World J Radiol 2016; 8 (04) 342-354
- 12 Haldorsen IS, Lura N, Blaakær J, Fischerova D, Werner HMJ. What is the role of imaging at primary diagnostic work-up in uterine cervical cancer?. Curr Oncol Rep 2019; 21 (09) 77
- 13 Lucas R, Lopes Dias J, Cunha TM. Added value of diffusion-weighted MRI in detection of cervical cancer recurrence: comparison with morphologic and dynamic contrast-enhanced MRI sequences. Diagn Interv Radiol 2015; 21 (05) 368-375
- 14 Bhatla N, Berek JS, Cuello Fredes M. et al. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynaecol Obstet 2019; 145 (01) 129-135
- 15 Woo S, Atun R, Ward ZJ, Scott AM, Hricak H, Vargas HA. Diagnostic performance of conventional and advanced imaging modalities for assessing newly diagnosed cervical cancer: systematic review and meta-analysis. Eur Radiol 2020; 30 (10) 5560-5577
- 16 Zhou S, Peng F. Patterns of metastases in cervical cancer: a population-based study. Int J Clin Exp Pathol 2020; 13 (07) 1615-1623
- 17 Olthof EP, Bergink-Voorthuis BJ, Wenzel HHB. et al. Diagnostic accuracy of MRI, CT, and [18F]FDG-PET-CT in detecting lymph node metastases in clinically early-stage cervical cancer - a nationwide Dutch cohort study. Insights Imaging 2024; 15 (01) 36
- 18 Brunette LL, Bonyadlou S, Ji L. et al. Predictive value of FDG PET/CT to detect lymph node metastases in cervical cancer. Clin Nucl Med 2018; 43 (11) 793-801
- 19 Meng X, Song S, Li K. et al. Application of CT in predicting lymph node metastasis in cervical cancer and construction of a preoperative nomogram. Sci Rep 2025; 15 (01) 11674
- 20 Wu Q, Lou J, Liu J. et al. Performance of node reporting and data system (node-RADS): a preliminary study in cervical cancer. BMC Med Imaging 2024; 24 (01) 28
- 21 Bipat S, Glas AS, van der Velden J, Zwinderman AH, Bossuyt PM, Stoker J. Computed tomography and magnetic resonance imaging in staging of uterine cervical carcinoma: a systematic review. Gynecol Oncol 2003; 91 (01) 59-66
- 22 Choi HJ, Ju W, Myung SK, Kim Y. Diagnostic performance of computer tomography, magnetic resonance imaging, and positron emission tomography or positron emission tomography/computer tomography for detection of metastatic lymph nodes in patients with cervical cancer: meta-analysis. Cancer Sci 2010; 101 (06) 1471-1479
- 23 Pereira GC, Traughber M, Muzic Jr RF. The role of imaging in radiation therapy planning: past, present, and future. BioMed Res Int 2014; 2014: 231090
- 24 Popat P, Maheshwari A, Manchanda S. et al. Imaging recommendations for diagnosis, staging, and management of cervical cancer. Indian J Med Paediatr Oncol 2023; 44: 119-129
- 25 Mahantshetty U, Deodhar K, Modi R, Kerkar R. Cervical cancer. Tata Memorial Centre Textbook of Oncology. Springer; 2024: 777-794
- 26 Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri. Int J Gynaecol Obstet 2018; 143 (Suppl. 02) 22-36
- 27 Bourgioti C, Chatoupis K, Rodolakis A. et al. Incremental prognostic value of MRI in the staging of early cervical cancer: a prospective study and review of the literature. Clin Imaging 2016; 40 (01) 72-78
- 28 Sala E, Rockall AG, Freeman SJ, Mitchell DG, Reinhold C. The added role of MR imaging in treatment stratification of patients with gynecologic malignancies: what the radiologist needs to know. Radiology 2013; 266 (03) 717-740
- 29 Kaur H, Silverman PM, Iyer RB, Verschraegen CF, Eifel PJ, Charnsangavej C. Diagnosis, staging, and surveillance of cervical carcinoma. AJR Am J Roentgenol 2003; 180 (06) 1621-1631
- 30 Patel-Lippmann K, Robbins JB, Barroilhet L, Anderson B, Sadowski EA, Boyum J. MR imaging of cervical cancer. Magn Reson Imaging Clin N Am 2017; 25 (03) 635-649
- 31 Mitchell DG, Snyder B, Coakley F. et al. Early invasive cervical cancer: tumor delineation by magnetic resonance imaging, computed tomography, and clinical examination, verified by pathologic results, in the ACRIN 6651/GOG 183 Intergroup Study. J Clin Oncol 2006; 24 (36) 5687-5694
- 32 Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri: 2021 update. Int J Gynaecol Obstet 2021; 155 (Suppl 1, Suppl 1): 28-44
- 33 Mahantshetty U, Swamidas J, Khanna N, Engineer R, Merchant NH, Shrivastava S. Magnetic resonance image-based dose volume parameters and clinical outcome with high dose rate brachytherapy in cervical cancers – a validation of GYN GEC-ESTRO brachytherapy recommendations. Clin Oncol (R Coll Radiol) 2011; 23 (05) 376-377
- 34 Haie-Meder C, Pötter R, Van Limbergen E. et al; Gynaecological (GYN) GEC-ESTRO Working Group. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiother Oncol 2005; 74 (03) 235-245
- 35 Pötter R, Haie-Meder C, Van Limbergen E. et al; GEC ESTRO Working Group. Recommendations from gynaecological (GYN) GEC ESTRO working group (II): concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy-3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiother Oncol 2006; 78 (01) 67-77
- 36 Nag S, Gupta N. A simple method of obtaining equivalent doses for use in HDR brachytherapy. Int J Radiat Oncol Biol Phys 2000; 46 (02) 507-513
- 37 Dimopoulos JC, Petrow P, Tanderup K. et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (IV): basic principles and parameters for MR imaging within the frame of image based adaptive cervix cancer brachytherapy. Radiother Oncol 2012; 103 (01) 113-122
- 38 Balleyguier C, Sala E, Da Cunha T. et al. Staging of uterine cervical cancer with MRI: guidelines of the European Society of Urogenital Radiology. Eur Radiol 2011; 21 (05) 1102-1110
- 39 Testa AC, Di Legge A, De Blasis I. et al. Imaging techniques for the evaluation of cervical cancer. Best Pract Res Clin Obstet Gynaecol 2014; 28 (05) 741-768
- 40 Gaffney DK, Erickson-Wittmann BA, Jhingran A. et al. ACR Appropriateness Criteria® on advanced cervical cancer expert panel on radiation oncology-gynecology. Int J Radiat Oncol Biol Phys 2011; 81 (03) 609-614
- 41 Ciulla S, Celli V, Aiello AA. et al. Post treatment imaging in patients with local advanced cervical carcinoma. Front Oncol 2022; 12: 1003930
- 42 Papadopoulou I, Stewart V, Barwick TD. et al. Post-radiation therapy imaging appearances in cervical carcinoma. Radiographics 2016; 36 (02) 538-553
- 43 Skipar K, Hompland T, Lund KV. et al. MRI-guided dynamic risk assessment in cervical cancer based on tumor hypoxia at diagnosis and volume response at brachytherapy. Radiother Oncol 2024; 195: 110263
- 44 Yadav D, O'Dwyer E, Agee M, Dutruel SP, Mahajan S, Huicochea Castellanos S. Unraveling the role of PET in cervical cancer: review of current applications and future horizons. J Imaging 2025; 11 (02) 63
- 45 Fields EC, Weiss E. A practical review of magnetic resonance imaging for the evaluation and management of cervical cancer. Radiat Oncol 2016; 11: 15
- 46 Rockall AG, Sohaib SA, Harisinghani MG. et al. Diagnostic performance of nanoparticle-enhanced magnetic resonance imaging in the diagnosis of lymph node metastases in patients with endometrial and cervical cancer. J Clin Oncol 2005; 23 (12) 2813-2821
- 47 Shi Q, Pisani LJ, Lee YK. et al. Evaluation of the novel USPIO GEH121333 for MR imaging of cancer immune responses. Contrast Media Mol Imaging 2013; 8 (03) 281-288
- 48 Dappa E, Elger T, Hasenburg A, Düber C, Battista MJ, Hötker AM. The value of advanced MRI techniques in the assessment of cervical cancer: a review. Insights Imaging 2017; 8 (05) 471-481
- 49 Nie J, Zhang J, Gao J. et al. Diagnostic role of 18F-FDG PET/MRI in patients with gynecological malignancies of the pelvis: a systematic review and meta-analysis. PLoS One 2017; 12 (05) e0175401
- 50 Kim SK, Choi HJ, Park SY. et al. Additional value of MR/PET fusion compared with PET/CT in the detection of lymph node metastases in cervical cancer patients. Eur J Cancer 2009; 45 (12) 2103-2109