

Subscribe to RSS
DOI: 10.1055/s-0045-1813649
Odontoid Fracture Nonunion with Atlantoaxial Instability, Myelopathy, High-Riding Vertebral Artery, and Narrow Pars Treated with C1-C2-C3 Posterior-Only Fixation: First Case Report
Authors

Abstract
Nonunion is a known complication of odontoid fractures. However, coexisting instability and neurological involvement render odontoid fixation alone insufficient for effective management. This scenario necessitates atlantoaxial fusion, which can be achieved through anterior, posterior, or combined approaches. We report a case of a 51-year-old female with posttraumatic nonunion of type II odontoid fracture, atlantoaxial instability, high-riding vertebral artery, and narrow pars, presenting with spastic quadriparesis. She underwent C1–C3 posterior cervical fixation and fusion. The patient demonstrated significant neurological improvement at 1-year follow-up. This case highlights the importance of ruling out cervical myelopathy in such patients. There are no prior reports in the literature describing odontoid nonunion leading to atlantoaxial instability and cervical myelopathy in the presence of a high-riding vertebral artery. The case also underscores the ongoing dilemma regarding the ideal surgical approach in such complex anatomical scenarios at the C1–C2 junction, known for its numerous variations.
Keywords
nonunion odontoid - myelopathy - C2 pars screws fixation - high-riding vertebral artery - atlantoaxial instabilityIntroduction
Odontoid fractures account up to half of all axis fractures.[1] The three forms of odontoid fractures were described by Anderson and D'Alonzo in 1974. The anatomical position of the fracture serves as the basis for this classification, in which the type II fracture occurs at the junction, where the C2 body and dens meet.[2]
The current gold standard management for type II odontoid fractures is still unclear. A revision to the widely accepted categorization of these fractures was reported by Grauer et al,[3] [4] where type II odontoid fractures were divided into three groups according to the displacement of the fractured dens segment. For type II subtype B, the authors recommended an anterior odontoid screw in this modification, which was more treatment-focused. But type II odontoid fractures with nonunion, instability, cervical myelopathy, and anatomical variations in the region present a challenging scenario for such treatment. Surgical intervention has shown benefits in terms of lowering rates of nonunion, mortality, and improved myelopathy scores.[5] [6] Anterior transodontoid screw fixation has been successful in achieving good clinical and radiological outcomes without complications, if there is no instability.[7] In cases of chronic, posteriorly displaced type II odontoid fractures, meticulous open reduction and fixation are necessary for successful management.[8] While surgical stabilization is associated with better outcomes, including lower nonunion rates and mortality, it is crucial to consider the patient's age, comorbidities, and potential complications when deciding on the appropriate treatment approach for type II odontoid fractures with coexisting nonunion, instability, cervical myelopathy, and high-riding vertebral artery (HRVA) with narrow pars. This happens to be a first reported incidence.
Case Report
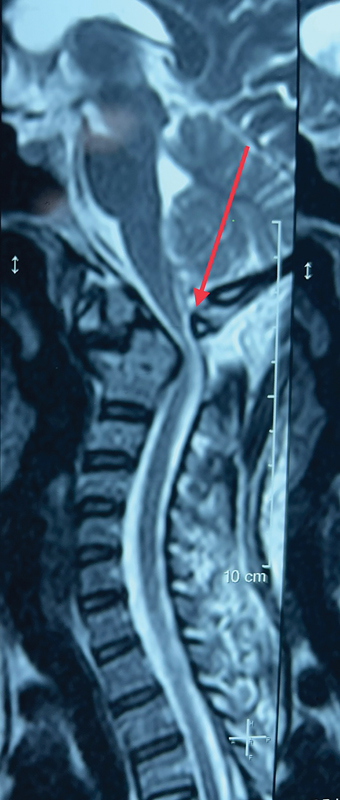
A 51-year-old female came with complaint of pain in her neck since history of fall 5 months ago. She had pain in her cervical region at presentation, which then progressed to tingling and numbness in her bilateral upper limb and lower limb in 2 months' duration. She had difficulty in walking since then and was bedridden since a month before arriving at the outpatient department for further management. On examination, she was found to have spasticity in all four limbs with exaggerated reflexes and signs of upper motor neuron lesion, Babinski–Hoffmann reflex; inverted radial reflex was bilaterally positive with a modified Japanese Orthopaedic Association (MJOA) score of 11 and Neurick score of 6. On radiographic evaluation of her cervical spine, she was found to have C1-C2 instability on flexion-extension dynamic radiographs with a type 2 fracture nonunion of odontoid, which was additionally confirmed on magnetic resonance imaging (MRI). Ossified posterior longitudinal ligament was ruled out by computed tomography (CT) scan but she was found to have narrow pars on the left side. Rheumatoid arthritis was ruled out by rheumatoid profile (rheumatoid factor, anti-cyclic citrullinated peptide, erythrocyte sedimentation rate, and C-reactive protein) and discussion with our rheumatologist. Because of coexisting deranged renal function tests, CT angiography craniovertebral junctional, which is considered mandatory for atlantoaxial surgeries, could not be performed. Hence, MRI-based assessment and look out for gross anatomical variations was done and she was found to have HRVA on her right side, because of which C2 pedicle screw fixation was not preferred. But she was in need of fusion surgery considering her instability and myelopathy stage. But because of narrow pars on the right side and HRVA on the right side, on surgical planning, with scarcity of advanced technology of O-arm and navigation, to ensure a stronger fixation construct the fixation was decided to be extended to C3. She hence underwent C1 lateral mass screw, C2 pars screw, and C3 lateral mass screw fixation. Case details are shown in the [Figs. 1] [2] [3] [4] to [5].




There were no unforeseen incidences intraop and postop. The patient was discharged with a hard cervical collar. At 6 months' follow-up, she neurologically improved to functional independence (MJOA 17 and Neurick 4), with no evidence of pseudoarthrosis or implant failure on CT scan. She was relieved from the collar at 1.5 months and remains neurologically and structurally stable at 1 year postoperative.
Discussion
Nonunion of posttraumatic fracture odontoid is a known complication, which can be treated surgically by both anterior and posterior approach. When the nonunion is associated with atlantoaxial instability, there needs to be a fusion of both the vertebrae. If there is coexisting cord compression secondary to degenerative changes, it requires an active and urgent intervention to prevent the neurological deterioration.
Shamji et al[8] have published a case report on a 68-year-old female with nonunion type 2 odontoid fracture causing cervical myelopathy where the patient underwent both anterior and posterior cervical fusion surgery (360 fusion) and they reported excellent follow-up at 1 year.
There have been other similar case reports and the largest being that of Ho and Ho[9] in 2010 where there was a female with nonunion odontoid who was managed conservatively and showed no significant improvement in neurology. These case reports, although scarce when compared with ours, suggest that nonunion odontoid almost always needs to be surgically fixed and fused to achieve a good surgical outcome and conservative management is not an option.
But this happens to be a novel case report because of the presence of multiple factors like, posttraumatic type 2 fracture odontoid nonunion with instability and myelopathy in a patient with HRVA and narrow pars, which was managed with posterior-only fixation and has showed an excellent outcome. There has been only one similar case report of nonunion of odontoid fixed with posterior-only fixation,[10] but their case did not have any anatomical variations at the atlantoaxial joint. And we believed on posterior-only approach considering increased risks and complications for the patient.
There is further scope for research to be done comparing anterior and posterior fixation with posterior fixation alone in patients with posttraumatic nonunion fracture odontoid with neurological involvement. Additionally, dynamic imaging can be done to assess the long-term follow-up, and should be included in further studies to assess the adequacy of fusion, but was not performed in our case due to the neurological recovery that the patient displayed.
Conclusion
This case highlights the neurological hazard of nonunion of type 2 fracture odontoid and the coexisting instability. Both of which needs to be addressed, hence requiring adequate planning and to never undermine the variations in course of vertebral artery around the atlas and axis vertebra, which has to be considered before planning intervention in such scenarios.
Conflict of Interest
None declared.
Authors' Contributions
C.S.S. prepared the manuscript, analyzed the findings, and assisted in the case. M.S.T. performed the surgery and contributed to manuscript preparation. M.B. also assisted in the preparation of the manuscript.
Ethical Approval
Ethics approval and consent were obtained from the Institutional Ethics Committee IEC/SNMC.
-
References
- 1 Greene KA, Dickman CA, Marciano FF, Drabier JB, Hadley MN, Sonntag VK. Acute axis fractures. Analysis of management and outcome in 340 consecutive cases. Spine 1997; 22 (16) 1843-1852
- 2 Anderson LD, D'Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am 1974; 56 (08) 1663-1674
- 3 Ricciardi L, Trungu S, Scerrati A. et al. Odontoid screw placement for Anderson type II odontoid fractures: how do duration from injury to surgery and clinical and radiological factors influence the union rate? A multicenter retrospective study. J Neurosurg Spine 2020; 34 (01) 27-31
- 4 Grauer JN, Shafi B, Hilibrand AS. et al. Proposal of a modified, treatment-oriented classification of odontoid fractures. Spine J 2005; 5 (02) 123-129
- 5 Mohamed A, Ehab Y, Hassanin A, Ibrahim A. Anterior odontoid lag screw fixation in type II odontoid fractures. Egypt Orthopaed J 2024;
- 6 Rathod T, Prabhu RM, Mohanty SS, Chandanwale A. A novel technique of managing an irreducible posteriorly displaced type 2 odontoid fracture: a case report. Surg Neurol Int 2023; 14: 371
- 7 Avila MJ, Farber SH, Rabah NM. et al. Nonoperative versus operative management of type II odontoid fracture in older adults: a systematic review and meta-analysis. J Neurosurg Spine 2023; 40 (01) 45-53
- 8 Shamji MF, Alotaibi N, Ghare A, Fehlings MG. Chronic hypertrophic nonunion of the Type II odontoid fracture causing cervical myelopathy: case report and review of literature. Surg Neurol Int 2016; 7 (Suppl. 03) S53-S56
- 9 Ho AW, Ho YF. Atlanto-axial deformity secondary to a neglected odontoid fracture: a report of six cases. J Orthop Surg (Hong Kong) 2010; 18 (02) 235-240
- 10 Shaaban ATE, Doomi A, Belkheir S. A case of cervical myelopathy following chronic hypertrophic non-union type 2 odontoid fracture managed with posterior C1 decompression and C1-3 instrumentation: case report and brief review of literature. Surg Neurol Int 2020; 11: 132
Address for correspondence
Publication History
Article published online:
22 December 2025
© 2025. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Greene KA, Dickman CA, Marciano FF, Drabier JB, Hadley MN, Sonntag VK. Acute axis fractures. Analysis of management and outcome in 340 consecutive cases. Spine 1997; 22 (16) 1843-1852
- 2 Anderson LD, D'Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am 1974; 56 (08) 1663-1674
- 3 Ricciardi L, Trungu S, Scerrati A. et al. Odontoid screw placement for Anderson type II odontoid fractures: how do duration from injury to surgery and clinical and radiological factors influence the union rate? A multicenter retrospective study. J Neurosurg Spine 2020; 34 (01) 27-31
- 4 Grauer JN, Shafi B, Hilibrand AS. et al. Proposal of a modified, treatment-oriented classification of odontoid fractures. Spine J 2005; 5 (02) 123-129
- 5 Mohamed A, Ehab Y, Hassanin A, Ibrahim A. Anterior odontoid lag screw fixation in type II odontoid fractures. Egypt Orthopaed J 2024;
- 6 Rathod T, Prabhu RM, Mohanty SS, Chandanwale A. A novel technique of managing an irreducible posteriorly displaced type 2 odontoid fracture: a case report. Surg Neurol Int 2023; 14: 371
- 7 Avila MJ, Farber SH, Rabah NM. et al. Nonoperative versus operative management of type II odontoid fracture in older adults: a systematic review and meta-analysis. J Neurosurg Spine 2023; 40 (01) 45-53
- 8 Shamji MF, Alotaibi N, Ghare A, Fehlings MG. Chronic hypertrophic nonunion of the Type II odontoid fracture causing cervical myelopathy: case report and review of literature. Surg Neurol Int 2016; 7 (Suppl. 03) S53-S56
- 9 Ho AW, Ho YF. Atlanto-axial deformity secondary to a neglected odontoid fracture: a report of six cases. J Orthop Surg (Hong Kong) 2010; 18 (02) 235-240
- 10 Shaaban ATE, Doomi A, Belkheir S. A case of cervical myelopathy following chronic hypertrophic non-union type 2 odontoid fracture managed with posterior C1 decompression and C1-3 instrumentation: case report and brief review of literature. Surg Neurol Int 2020; 11: 132