

RSS-Feed abonnieren
DOI: 10.1055/s-0045-1813042
Reuse of Single-Use Devices in Interventional Radiology: Indian Society of Vascular and Interventional Radiology (ISVIR) Guidelines 2025
Autor*innen
Funding None.


Abstract
In response to a proposal from the ISVIR members forum, an expert committee was established to comprehend the practice and formulate guidelines for the reuse of medical devices designated for single use. This initiative arose from the widespread use of single-use devices (SUDs) coupled with the absence of established guidelines. A comprehensive literature review on the subject was conducted. Additionally, a survey was administered to interventional radiology practitioners to evaluate their knowledge, attitudes, and practices. The expert committee members have considered a holistic approach to the topic, which encompasses definitions, the rationale for reuse, existing guidelines from other countries, similar societies, processing methods, and the responsibilities of stakeholders. A life cycle analysis of SUDs has been created to enhance understanding. Ethical and legal considerations have also been examined. Furthermore, the impact on research and global trends has been assessed. Given the scarcity of robust evidence, most recommendations are graded as 1C, reflecting expert opinion with low evidence strength. Accordingly, these guidelines should be interpreted with caution, serving primarily as a framework to support clinical decision-making and patient safety. [Supplementary Materials (1] [2] [3] [4], available in the online version only) have been provided for additional information. The authors are confident that the insights gained from this endeavor will aid in clinical decision-making and enhance patient safety. We anticipate the emergence of more randomized controlled trials in the near future, which may strengthen future guidance.
Introduction
The reuse of single-use devices (SUDs) is an evolving practice influenced by the growing need to reduce healthcare costs and minimize medical waste. Regulatory bodies such as the US FDA and UK MHRA define SUDs as devices intended for one-time use on a single patient. However, economic and environmental pressures have led many institutions to explore the safe and regulated reprocessing of selected SUDs. While concerns exist—such as cross-infection, endotoxin exposure, device failure, and chemical residue—evidence suggests[1] that, with proper protocols, many of these risks can be effectively mitigated. In several hospitals, multidisciplinary oversight involving clinicians, infection control teams, engineers, and legal experts ensures safe reprocessing practices. This document outlines practical guidelines for the selective and responsible reuse of SUDs, promoting safety, sustainability, and cost-effectiveness in clinical practice.
Methodology
Guideline Development Framework
These guidelines were developed using a transparent, structured consensus methodology under the aegis of the Indian Society of Vascular and Interventional Radiology (ISVIR). To identify priority areas for national guidance, ISVIR disseminated a structured digital survey among its members. Respondents ranked potential topics according to clinical relevance, economic impact, safety considerations, and environmental implications. “Reuse of materials in interventional radiology” emerged as a top-priority subject.
Constitution of the Guideline Development Group
A guideline development group (GDG) comprising 10 experts was appointed by ISVIR. Members were selected based on domain expertise, peer-reviewed publications, and representation from diverse geographical, institutional, and practice backgrounds (including government hospitals, private healthcare institutions, and charitable organizations).
Evidence Review
The GDG performed a comprehensive literature review using PubMed, EMBASE, and Google Scholar. The search strategy included terms such as reuse, single-use devices, interventional radiology, cost containment, sterilization, and safety. The search was not time-restricted and aimed to capture all relevant studies published to date.
National Practice Survey
A national online survey, developed in Google Forms, was circulated via email and social media platforms to IR professionals across India. The questionnaire included multiple-choice and open-ended questions addressing reuse practices, reprocessing techniques, device types, legal implications, and perceived need for national guidelines. A total of 103 responses were obtained from a broad spectrum of institutions, ensuring a representative overview of current practice ([Supplementary Material 3] [available in the online version only]). The survey was conducted in accordance with the principles of the Declaration of Helsinki. As this was an opinion-based survey without the collection of identifiable personal information, the requirement for individual informed consent was waived by the Institutional Review Board. The survey was made available for responses on May 24, 2025, and was closed on June 1, 2025.
Consensus Process
The consensus process followed a structured Likert scale approach.[2] [3] Preliminary recommendations were drafted and iteratively refined through multiple online discussion rounds. Each GDG member rated their agreement on a 10-point Likert scale (1 = strongly disagree; 10 = strongly agree). Statements achieving ≥80% agreement at a score of ≥8 were accepted as consensus. Statements not meeting the threshold were revised based on anonymized feedback and re-circulated for further voting. For each final recommendation, the grade of recommendation and level of evidence were assigned in accordance with the UPTODATE's current best practice guidelines.[4]
Final Approval and Endorsement
The completed guideline document was unanimously approved by the GDG and subsequently endorsed by the ISVIR Executive Council.
Ethics and Funding
Ethical approval was not required for the consensus process, as it was based on expert opinion and literature review without patient data. No external funding was received, and all participants disclosed potential conflicts of interest.
Background
Q1. What is single-use device (SUD)?
Answer: US FDA department (Federal Food, Drug, and Cosmetic Act) and UK MHRA (Medicines and Healthcare Products Regulatory Agencies)[1] [5] define SUD as:
Single-use device: A device that is intended for one use, or on a single patient during a single procedure ([Fig. 1]).[6]

Reprocessed/Reuse (R-SUD): The term “reprocessed,” with respect to a SUD, means an original device that has previously been used on a patient and has been subjected to additional processing and manufacturing for the purpose of an additional single use on a patient. The subsequent processing and manufacture of a reprocessed SUD shall result in a device that is reprocessed within the meaning of this definition.
Level of evidence/grade of recommendation: 1C
Remarks:
The term “single-patient use” means the medical device may be used for more than one episode of use on one patient only; the device may undergo some form of reprocessing between each use ([Fig. 2]).[1] [6] Cross-expiry unused SUD are not considered in our discussion.

Q2. What are the characteristics of potentially reusable SUD, non-reusable SUD, and reusable medical devices (RUD)?
Answer: Potentially reusable SUD (PR-SUD).
A device originally labelled as single-use, but may be considered for reuse if all the following criteria are met:
-
Retrieved in toto (entirely, without damage).
-
Cleanable thoroughly.
-
Reassemblable to its original form.
-
Sterilizable effectively.
-
Has a mechanism to check integrity and functionality, ensuring performance similar to first use.
Level of evidence/grade of recommendation: 1C
Remarks:
Non-reusable SUD:
A device must not be reused if any one of the above criteria is not met.
Examples: Vascular access closure devices, self-expanding stent delivery systems, very long angioplasty balloons.
Reusable medical devices (RUD):
Any medical device which are recommended by the manufacturers for reuse is considered a reusable medical device (RUD). Examples of reusable medical devices include surgical forceps, endoscopes, and stethoscopes, e.g., biopsy guns (Bard Magnum gun).[7]
If a device does not have reprocessing instructions, it is considered single-use and should be disposed of after one use.
Reusable medical devices can be classified into three categories according to the Spaulding classification system.[8] [9] [10] Critical devices, such as surgical forceps, come into contact with blood or normally sterile tissue and therefore require the highest level of sterilization. Semicritical devices, such as endoscopes, contact mucous membranes and require high-level disinfection at a minimum. Noncritical devices, such as stethoscopes, only contact intact skin and generally require low-level disinfection.
Q3. What are the concerns while reusing the SUD?
Answer: Reusing SUDs poses significant risks, including cross-infection, endotoxin reactions, device failure, and chemical injuries due to residual disinfectants. Material fatigue and legal liability further complicate reuse. Strict validation is essential before considering reprocessing.
Level of evidence/grade of recommendation: 1C
Remarks:
Reuse of SUDs can pose several safety risks:[1] [11] [12] [13] [14] These include the possibility of cross-infection due to the inability to adequately clean and decontaminate devices with complex designs; endotoxin reactions arising from excessive bacterial breakdown products that cannot be completely removed during cleaning; and patient injury resulting from device failure caused by fatigue, material alteration, or embrittlement during reprocessing. Additionally, chemical burns or sensitization may occur from residues of chemical decontamination agents, particularly in materials capable of absorbing or adsorbing such chemicals. Finally, there is the risk of legal liability associated with adverse outcomes linked to reuse.
Q4. Why reuse the devices?
Answer: Reusing SUDs significantly reduces healthcare costs and minimizes environmental waste. It helps lower emissions and conserve resources while maintaining patient safety.
Level of evidence/grade of recommendation: 1C
Remarks:
Cost is particularly important in developing countries where the cost of healthcare is high.[9] [11] [15] Reuse of SUD reduces the cost of the procedure, making it affordable for the patient. Also, in countries with limited resources, new devices may not be readily available when needed, thus necessitating to reuse SUDs to ensure the continuous availability of the necessary devices.
Annual estimates of savings with reprocessing in the United States have been reported to be approximately $ 1.8 billion per year.[11] A survey conducted across 3000 hospitals using reprocessed SUDs in the United States reported savings in excess of $ 150 million every year.[16] Cost estimate studies from Germany report savings of up to 20 million Euros per year from reprocessing balloon angioplasty catheters.[15]
Interventional radiology (IR) is an essential component of modern healthcare. However, as the volume and complexity of IR procedures increase, the waste burden that is generated also increases exponentially.[9] [17] [18] An audit of greenhouse gas generated by a hospital-based IR department in New York found that ∼23,500 kg CO2e (equivalent to burning 9,900 L of gasoline) was emitted over five consecutive weekdays, with an average of 243 kg CO2e generated per IR procedure.[19] Neurointerventional procedures produced an average of 8 kg of waste per case.[20]
It has also been noted that some manufacturers changed the labelling of their products from multiuse to single-use only without making significant changes to the devices in the initial years, thereby making the labelling of SUD arbitrary.[18] [21]
Available Publications—Literature/Countries Regulations/Societies Statements/White Papers from Authorities
Q5. What is the status of the regulatory framework for the reuse of the SUDs in different countries?
Answer: The regulatory framework for the reuse of SUDs varies across countries. Developed countries like the United States, Canada, and Australia have well well-established legal regulatory framework for reusing SUDs. In contrast, while reusing SUDs is a common practice in developing countries, there is a lack of specific regulations. Instead, the reuse of SUDs in these regions is primarily guided by hospital or institutional guidelines ([Supplementary Material 1] [available in the online version only]; [Fig. 3]).

 Green circles indicate countries/regions with established regulatory frameworks for
reuse of SUDs, while
Green circles indicate countries/regions with established regulatory frameworks for
reuse of SUDs, while  red circles indicate the absence of such regulations.
red circles indicate the absence of such regulations.Statement: Single-use devices (SUDs) can be reused if they are reprocessed by licensed facilities in accordance with the regulations specific to each country.[1] [5] [22] [23] [24] [25] [26] [27] [28] [29] [30] [31] [32] [33] [34] [35] [36] [37] [38] [39] [40] [41] [42] [43] [44] [45]
Level of evidence/Grade of recommendation: 1C
Remarks:
Having guidelines/policy and a regulatory framework will establish a clear direction for managing potential challenges and foster a shared understanding and responsibility among all parties involved. Once a policy or guideline for medical device management is created, its implementation and incorporation into national legislation will be influenced by the specific national context and available resources for monitoring and enforcement.
It is crucial for companies or hospitals engaged in the reprocessing of single-use devices (SUDs) to obtain the necessary licenses and comply with relevant international, national, and regional regulations. Reprocessors are regarded as the original manufacturers of the devices and bear legal responsibilities for their safe operation and quality. To ensure that reprocessed devices meet the safety and efficacy standards of the original products, reprocessors must implement a robust quality management system.
Q6. What is the stand of the other societies on the reuse of the SUDs?
Answer: Several medical societies/organizations have issued position statements, consensus documents, or guidelines regarding the reuse of single-use devices (SUDs). While the primary motivation for endorsing the reuse of SUDs is cost savings, there are definite safety concerns that lead some organizations to oppose this practice ([Supplementary Material 2] [available in the online version only]).
Statement: Various organizations have issued guidelines, position statements, and consensus documents regarding the reuse of single-use devices (SUDs).[10] [17] [46] [47] [48] [49] [50] [51] [52] [53] [54] [55] [56] [57]
Level of evidence/Grade of recommendation: 1C
Remarks:
Reuse of SUDs is a common practice in many countries, offering both financial and environmental benefits. While guidelines from medical societies and hospital institutions are valuable, it is essential to regulate the reuse of SUDs with an established reprocessing standard. Additionally, there should be a mechanism for reporting adverse events and outcomes related to reused devices to the relevant regulatory authority of the country. This data can facilitate research on the safety and efficacy of reused SUDs, ultimately aiding in the refinement of current practices.
How to Reprocess/How to Regulate/How to Determine the Effectiveness
Q7. How to reprocess a device?
Answer: Statement—Since there are different types of SUDs, the reprocessing should be as per institutional SOPs. It is recommended that this is according to the accreditation body and mandatory according to the regulatory body if applicable.
Level of evidence/grade of recommendation: 1C
Remarks:
Reprocessing of SUDs should be done at the hospital level with clearly defined, device-specific protocols or by third-party reprocessor. We are not aware of any certified third-party reprocessors in India. The process must include standardized steps such as thorough cleaning, drying, sterilization (commonly with ethylene oxide), integrity checks, and proper labeling. Reprocessing methods should be approved by the institution's infection control and biomedical engineering teams, with clear documentation and a defined limit on the number of reuses. In the absence of national guidelines, hospitals must ensure internal validation and adherence to best practices to maintain patient safety. This may be updated to the accreditation body when applicable.[48] [58] [59]
For example, the Cardiology Society of India, World Health Organization (WHO)'s 2016 document on decontamination and reprocessing of medical devices for health-care facilities describes various ways of reprocessing the SUDs. One example is quoted here[46] [47] [48]: To reprocess a catheter (hollow/non-hollow tubular devices), start by soaking it in an enzymatic detergent (neutral/alkaline), or an enzymatic cleaning agent. Make sure that the lumens are completely filled with the enzymatic detergent and disinfectant (step only in hollow devices). Carefully clean the entire surface of the catheter, using a flush and brush as necessary. Discard the used enzymatic detergent. Next, rinse the catheter with pressurized potable tap water or sterile distilled water for 10 minutes.
After rinsing, immerse the catheter in a high-level disinfectant that is compatible with the material—such as a 3% hydrogen peroxide solution—for 3 hours. Rinse the catheter thoroughly with clean water multiple times and then wipe it dry. Drying should be performed using compressed air jets that are free of oil, dust, and moisture. Inspect the catheter for any blood stains or dirt; if any are found, discard the catheter. Check for the overall integrity and functionality of the catheter.
Finally, repackage the catheter in double layers, sterilize it using ethylene oxide, and label it with the date of re-sterilization. Additionally, note the reuse number using different color codes for the 1st, 2nd, and 3rd reuses.
Q8. How many times can we reprocess/reuse?
Answer: Since there is heterogeneity in the type of material, a uniform number cannot be stated. The number of times of usage can be stated by the individual institution based on the type of device as SOP.
Level of evidence/grade of recommendation: 1C
Remarks:
A SUD that can withstand cleaning, disinfection, or sterilization and continue to comply with the necessary regulatory requirements (as for the original device) can be reused after reprocessing.[21] The maximum number of times a SUD can be used depends on the type of the SUD and on the data that the device is as safe and effective as the original device.
Hollow catheters (including diagnostic and microcatheters) are challenging to cleanse effectively to ensure that no organic materials remain in the lumen. Some recommendations (Cardiology Society of India) suggest a maximum of five reuses for non-hollow catheters and up to three reuses for hollow catheters.[48] In contrast, an old study suggests generation of data regarding the degradation of the coronary balloon catheters with use, as the toleration levels of these catheters are unknown.[60] While such cardiology-derived data provide a useful reference, they may not fully reflect the unique challenges of interventional radiology. Neurointerventional procedures, for example, often involve longer navigation through delicate vasculature, higher precision requirements, and different mechanical stresses compared to peripheral or body IR practices. These differences underscore the need for IR-specific evidence to guide reuse practices more reliably.
The WHO does not recommend the re-use of critical and semicritical SUDs unless the devices are reprocessed by a licensed reprocessor. It further recommends that SUDs with small lumens (catheters, drains, canulae) should not be reprocessed and reused.[61] A 2019 position statement published by Infection Prevention and Control, Canada, states that critical and semicritical medical equipment/devices labelled as single-use must not be reprocessed and reused unless a licensed reprocessor does the reprocessing.[62]
Heterogeneity in practice patterns and reliance on institutional standard operating procedures (SOPs) limit the ability to provide uniform guidance on the number of reuses. An attempt has been made to make a summary table linking device types with suggested reuse limits and device-related complications. However, More RCTs and Case studies are needed in this regard ([Table 1]).
Q9. How to identify/label the reused device/track the usage?
Answer: A robust quality management and tracking system is essential to ensure the safe reuse of single-use devices (SUDs).
Level of evidence/grade of recommendation: 1C
Remarks:
Identification and labelling can be done through clear methods such as color coding, barcoding, or tagging, which help differentiate reused devices from new ones. Documentation of each reuse cycle, including cleaning, sterilization, and inspection records, should be maintained.[12] This enables traceability and helps monitor the number of times a device has been reused, ensuring compliance with institutional or regulatory limits.
It is better to have a dual marking system—on the device itself (more than one similar material may be opened during the same procedure) as well as the package (all information cannot be written on the device). If ID mismatch is present, material can be discarded, or maximum usage may be counted as real. Certain planning should be done during the procedure itself if the reuse of materials is anticipated.
Q10. What should be the preparedness for the future potential reuse of material while doing a procedure?
Answer: Safe and sustainable reuse of medical materials requires stepwise planning—pre-, intra-, and post-procedure—focused on labelling, segregation, and functionality checks. Comprehensive staff training ensures standardization and minimizes risk in reuse practices ([Table 2]).
Level of evidence/grade of recommendation: 1C
Remarks:
Material must be handled carefully. Hollow catheters should be cleaned with saline each time, needless to say.[47] Implementation of AI-based image recognition and QR/barcode tracking can further enhance device verification.
Q11. Who is responsible for the performance of the reuse device?
Answer: The performance of reused SUDs must be overseen by a designated Reprocessing and Reuse Committee within each hospital, accountable for safety and compliance. As per institutional SOP, this responsibility may also be delegated to an approved third party.
Level of evidence/grade of recommendation: 1C
Remarks:
Certain countries have third-party reprocessing firms that assume legal responsibility and liability for the reprocessed equipment, thereby reducing hospitals' liability for reuse. In nations such as India, there are no officially recognized reprocessing firms. As a result, the liability for defects associated with the reuse of single-use items rests with the hospital.
Every hospital should establish a Reprocessing/Reuse Committee composed of physicians, infection control specialists, sterilization department, nurses, and administrators with regular internal and external audits. This committee can oversee central reprocessing, infection control, biomedical engineering, and cost management. The internal committee should be responsible for and accountable regarding protocol and safety matters. The hospital must ensure there is sufficient space allocated for reuse, trained staff, and other necessary supplies. Furthermore, the end-user (doctor) is also accountable for the performance of these devices, taking ethical considerations and integrity into account on a case-by-case basis.
Assessing the integrity of reused angiographic catheters requires a multimodal approach, including visual, mechanical, microscopic, and chemical testing. Given the potential for undetectable damage, rigorous validation is essential before reuse. Visual Inspection includes checking for cracks, stains, roughness, discoloration, and lumen narrowing. Mechanical Testing and Microscopic Analysis may be done if resources are there.[63] They include scanning electron microscopy to identify microcracks and structural defects. While chemical testing can assess molecular integrity, it may be impractical in resource-limited settings.[64] Regulatory bodies like the FDA mandate validation of functionality and integrity for reprocessed single-use devices.
ISVIR Survey Results
A total of 103 respondents participated in the survey, nearly 48% were affiliated with public hospitals, while the rest practiced in corporate or charitable institutions. Independent consultants comprised 74% of the cohort. Reuse of single-use devices (SUD) was reported by approximately 80% of respondents, most commonly involving guidewires, catheters, angioplasty balloons, and vascular sheaths. Formal departmental protocols for reuse were absent in 42% of practices. Tracking methods varied: physical marking (like ink on hubs or tally marks), manual records, or packaging labels to indicate usage count. Ethylene oxide sterilization was the predominant reprocessing method, reported by 80% of participants. The leading reason for reuse was financial constraints (97%), followed by a shortage of new devices and environmental considerations.
Regarding perceptions, 60% believed that endovascular SUDs can or should be reused, and an equal proportion were aware of some form of national or international guidance. Key concerns included risk of cross-infection, device damage during sterilization, and challenges in maintaining reuse records. Adverse events related to reused devices were reported by over 64%, and 56% felt that reuse could compromise procedural efficacy. Explicit disclosure and consent for reuse were supported by 35% of respondents. For cost allocation in multi-patient reuse, over 60% favored the first user bearing a larger share of the expense. In the event of a complication potentially linked to reuse, 56% believed courts would be unlikely to accept reuse as a valid justification. Standardized national guidelines for safe reuse were endorsed by more than 95% of participants ([Supplementary Material 3] [available in the online version only]).
Accreditations
Q12. What is the role of accreditation bodies in the reuse of SUDs?
Answer: Accreditation bodies play a critical role in implementing the safe practice of the reuse of SUDs. Accreditation bodies have recommendations, validate the SOPs stated by the institutions. They also conduct inspections to check whether the SOPs are followed.
Level of evidence/grade of recommendation: 1C
Remarks:
Joint Commission International (JCI) and NABH (National Accreditation Board for Hospitals and Healthcare Providers) are the two main accreditation bodies that recognize healthcare organizations for meeting high standards of quality and patient safety.[10] [65] Both organizations require hospitals to establish clear policies and procedures for the reuse and re-sterilization of single-use devices (SUDs). JCI specifically mandates that hospitals implement protocols to track SUDs and determine when a device is no longer safe or suitable for reuse. Additionally, JCI emphasizes that hospital policies must align with existing national laws and regulations, as well as professional standards. Despite strict guidelines by accreditation bodies, the lack of a comprehensive legal regulatory framework/legislation for the reuse of SUDs may lead to unsafe/unethical practices, which compromise patient safety. It also leaves hospitals vulnerable to legal and ethical challenges. To address this, we need a phased approach to formalize and regulate this practice ([Fig. 4]).
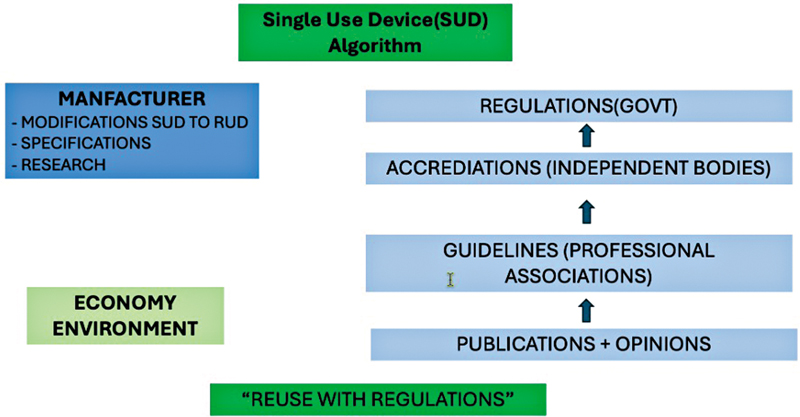
Professional and accreditation bodies (e.g., ISVIR–NABH) should collaborate to develop a phased framework for national accreditation audits tailored to resource-variable Indian centers. This may begin with defining minimum safety standards, progress to staff training and certification modules, and culminate in a tiered accreditation system with provisions for independent audits.
Reuse of Materials in Patients with Identified Biohazards
Q13. What should be the management practices to reuse devices after using them in patients with identified biohazards?
Answer: Devices used in patients with identified biohazards should ideally not be reused.
Level of evidence/grade of recommendation: 1C
Remarks:
In exceptional situations of financial constraint, reuse may be considered only for similar biohazard cases after proper decontamination and informed consent. Such decisions must be made on a strict case-by-case basis under expert supervision as per institutional SOP.
Impact on Research
Q14. What is the impact of research on the reuse of SUD in IR?
Answer: Further in-vivo and in-vitro research is required to generate evidence-based support for the reuse of single-use devices (SUDs), ensuring their safety and functionality following proper reprocessing.
Level of evidence/grade of recommendation: 1C
Remarks:
Studies have shown that certain IR tools can be safely reused after sterilization using methods like ethylene oxide, without compromising patient outcomes.[5] [44] [52] [58] [61] This research provides interventional radiologists with clinical confidence, reducing hesitation and uncertainty around device reuse. It also enables hospitals to implement standardized protocols based on data, ensuring safety, consistency, and regulatory compliance.
Further research can be pursued in two ways: (1) conducting randomized controlled trials (RCTs) comparing the safety and performance of new single-use devices (SUDs) versus reusable SUDs (R-SUDs); and (2) ensuring that studies involving the use of SUDs/R-SUDs include clear statements in their methodology regarding the reuse and reprocessing methods applied. In many existing studies—for example, those on GI bleed embolization, bronchial artery embolization, transjugular liver biopsies (TJLB), and embolization in splenic or liver trauma—reusable single-use devices (R-SUDs) might have been employed. However, most of these studies lack explicit statements in their methodology regarding R-SUD use and reprocessing methods. Including such statements in future publications could generate substantial evidence to support the safe and effective use of R-SUDs.
Beyond clinical practice, research empowers IRs to advocate for institutional policies and national guidelines that support ethical reuse. It also encourages transparency, such as informing patients when reused devices are involved, backed by published safety evidence. Additionally, ongoing research may lead to the development of cost-effective, locally manufactured devices designed for multiple uses, further reducing dependence on expensive imports.
Legal and Ethical Issues
Q15. Are there any legislation/regulatory frameworks of reusing of single-use devices (SUD) in India?
Answer: In accordance with the Drugs and Cosmetics Act, single-use medical devices must be used strictly as per the manufacturer's instructions, which typically specify one-time use only.[66]
Level of evidence/grade of recommendation: 1C
Remarks:
The recent update in 2025 also does not add significantly to SUD-related topics.[67]
Economics: Insurance Cover, Charges to Patient
Q16. What are the ethical considerations regarding informed consent when reused SUD is being used?
Answer: Patients must be clearly informed if any single-use devices (SUDs) are being reused during an IR procedure. Informed consent is essential to respect patient autonomy and ensure ethical transparency.
Level of evidence/grade of recommendation: 1C
Remarks:
Informed consent for the use of a reused device should clearly state that the device has been reprocessed.[13] [48] The consent process must briefly outline the sterilization method employed, the safety protocols in place, and any potential risks associated with reuse. Patients should be explicitly offered the option to refuse the use of a reused device. Any financial implications, such as potential cost reductions, should also be disclosed. Proper documentation of the consent is essential for medico-legal protection. An example consent form is provided in [Supplementary Material 4] (available in the online version only).
Q17. What are the ethical considerations regarding procedural charges when reused devices are used?
Answer: Charges billed to patients must reflect the actual cost of care. Using a reused or reprocessed device should not be charged as a new device unless explicitly justified and consented.
Level of evidence/grade of recommendation: 1C
Remarks:
Transparent pricing is essential when reused devices are employed. Any cost savings resulting from reuse should either be passed on to the patient or clearly explained. Charging the full price for a reused item without disclosure is both ethically and legally unacceptable. All billing practices must comply with institutional policies and be communicated to the patient in a clear and transparent manner.
Q18. Can R-SUD be covered by Indian medical insurance (government and private)?
Answer: Insurance coverage depends on whether the reuse complies with regulatory standards and manufacturer guidelines. However, insurance policies often lack uniformity in covering procedures involving reused devices, leading to out-of-pocket expenses for patients.
Level of evidence/grade of recommendation: 1C
Remarks:
If a SUD is reused without proper reprocessing, insurers may deny coverage for resulting complications or device-related expenses. Insurers often require documentation that the device was reused in a validated, regulatory-approved manner.
Global Impact
Q19. What is the global trend towards the reprocessed single-use devices?
Answer: There is reuse or intention to reuse of SUD globally for different reasons.
Level of evidence/grade of recommendation: 1C
Remarks:
In developing countries, cost can be a significant burden, indicating a trend of continuation, albeit with an overall reduction as the economy improves. No one has the resources to spend unnecessarily. Utilization should be approached in a “smart and scientific” manner rather than a “generous” one. Numerous publications have emphasized environmental concerns.[16] [19] [20] [68] [69] [70] It would represent a commitment if the IR departments were to advocate for a “go green” initiative.[69] [71]
Limitations/Scope for improvement/Things to Do
Q20. Who are the stakeholders involved in enhancing the reuse of materials?
Answer: Medical professionals utilizing the devices, researchers, hospital management, quality assurance teams, refurbishers, manufacturers, insurance companies, accreditation organizations, and government authorities are the stakeholders involved in enhancing the reuse of materials.
Level of evidence/grade of recommendation: 1C
Remarks:
Medical professionals utilizing the devices play a crucial role as they possess knowledge about the device's functionality. They assess the relative cost of the device in relation to its benefits and affordability. The identification of material types and acknowledgment of heterogeneity is a continuous process, especially as new materials are introduced into the market. The survey conducted as part of this study indicates that nearly half of the hospitals require the establishment and adherence to specific policies (survey). It is essential that audits be deemed mandatory by the users. Hospital administrators must ensure the provision of manpower, financial resources, and logistics necessary for facilitating reuse. It is advisable that audits conducted by a third party are more beneficial if refurbishing occurs internally. The primary users are also ideally positioned to lead these projects. The publications generated by them are crucial in determining the safety and efficacy of the regulations. Accreditation bodies must pay special attention to the reuse of SUD. Professional associations ought to contemplate the allocation of dedicated sessions during conferences. The guidelines established by these associations would be beneficial for practitioners. A dynamic ISVIR-managed digital repository can be established to update and reuse protocols and document adverse events. Professional organizations with comparable requirements and applications, such as cardiology and vascular surgery, can engage in the exchange of ideas to enhance mutual understanding. It is imperative that a dialogue between users and manufacturers facilitates modifications in device manufacturing, ensuring that the type of reuse is clearly defined and appropriately adapted. For instance, a bone drill should incorporate an electric recharging feature, complete with a display indicating the charge level. Additionally, devices should include a mechanism to track the number of reuses. Consequently, SUD should provide the option for reuse, although the decision to reuse ultimately rests with the user. Nonetheless, this guideline could evolve into a practical reference tool by classifying common devices and materials according to subspecialty systems (e.g., neuro-IR, body-IR, gastro-IR, pediatric IR), specifying which devices are more amenable to reuse and which fall into high-risk categories where reuse should be strictly avoided. We therefore emphasized the need for future randomized controlled trials and case studies to generate robust evidence that can inform subspecialty-specific guidance on device reuse. Regulatory authorities must develop specifications that include both simplified and detailed versions. While reuse is less prevalent in developed nations (such as the United States, Canada, and certain European countries), these regions do have regulatory frameworks established. These regulations are pertinent to the relevant government authorities. The considerations should encompass, but not be limited to, high standards for reprocessing, staff training, risk assessment, management, and validation of reprocessing, as well as ethical and legal considerations.[70] [72] [73]
This document will be reviewed and updated after 5 years, incorporating new evidence and literature available at that time.
Conclusion
Reuse of SUD may be considered based on the economy and environmental safety, but should be appropriately regulated: “Reuse but regulate.”
Level of evidence/grade of recommendation: 1C
Remarks:
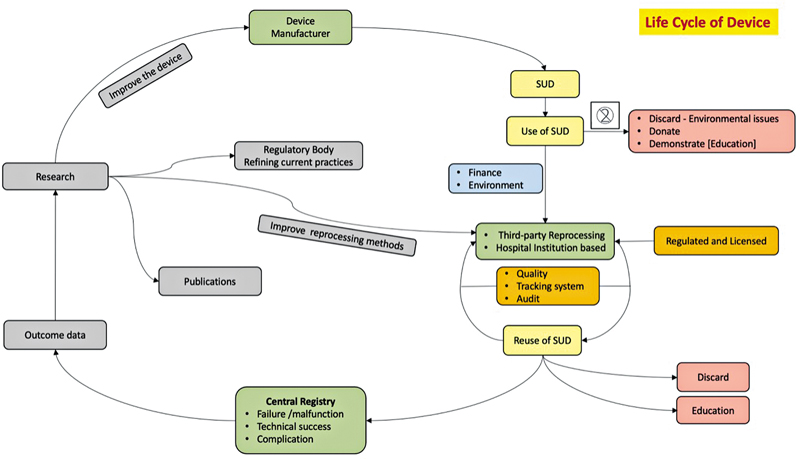
The reuse of SUD, when permitted, should be approached with caution. There exists a heterogeneity in the material. The current guidelines have outlined the necessity, methods, and timing for the safe, economical, and eco-friendly reuse of SUD. The management of materials and financial aspects has been considered. Although SUD is intended for single use, developing countries continue to utilize it predominantly due to financial constraints, while the concept is gaining importance in the Western world as a means to promote eco-friendliness. The hospitals reusing SUDs should have a detailed standard of practice (SOP) including all aspects mentioned in the life cycle of the device ([Fig. 5]). The recommendations by the accreditation bodies are advisable, and those by the regulatory authorities are mandatory.
It must be explicitly acknowledged that the majority of the recommendations in this guideline are graded as 1C, reflecting expert opinion supported by low-level evidence. Therefore, the guidance presented here should be interpreted as a framework to support safe practice rather than definitive standards. Given the widespread but under-studied practice of SUD reuse, the authors strongly emphasize the need for well-designed studies and randomized controlled trials to provide stronger evidence in the future ([Table 3]).
|
Sl. no. |
Statements |
|---|---|
|
1. |
US FDA department (Federal Food, Drug, and Cosmetic Act) and UK MHRA (Medicines and Healthcare Products Regulatory Agencies)[1] [5] define SUD as: Single-use device: A device that is intended for one use, or on a single patient during a single procedure ([Fig. 1]) Reprocessed/Reuse(R-SUD): The term “reprocessed,” with respect to a SUD, means an original device that has previously been used on a patient and has been subjected to additional processing and manufacturing for the purpose of an additional single use on a patient. The subsequent processing and manufacture of a reprocessed SUD shall result in a device that is reprocessed within the meaning of this definition |
|
2. |
Potentially reusable SUD (PR-SUD): A device originally labelled as single-use, but may be considered for reuse if all the following criteria are met: • Retrieved in toto (entirely, without damage) • Cleanable thoroughly • Reassemblable to its original form • Sterilizable effectively • Has a mechanism to check integrity and functionality, ensuring performance similar to first use |
|
3. |
Reusing SUDs poses significant risks, including cross-infection, endotoxin reactions, device failure, and chemical injuries due to residual disinfectants. Material fatigue and legal liability further complicate reuse. Strict validation is essential before considering reprocessing |
|
4. |
Reusing SUDs significantly reduces healthcare costs and minimizes environmental waste. It helps lower emissions and conserve resources while maintaining patient safety |
|
5. |
SUDs can be reused if they are reprocessed by licensed facilities in accordance with the regulations specific to each country |
|
6. |
Various organizations have issued guidelines, position statements, and consensus documents regarding the reuse of single-use devices (SUDs) |
|
7. |
Since there are different types of SUDs, the reprocessing should be as per institutional SOPs. It is recommended that this is according to the accreditation body and mandatory according to the regulatory body, if applicable |
|
8. |
Since there is heterogeneity in the type of material, a uniform number cannot be stated. The number of times of usage can be stated by the individual institution based on the type of device as SOP |
|
9. |
A robust quality management and tracking system is essential to ensure the safe reuse of SUDs |
|
10. |
Safe and sustainable reuse of medical materials requires stepwise planning—pre-, intra-, and post-procedure—focused on labelling, segregation, and functionality checks. Comprehensive staff training ensures standardization and minimizes risk in reuse practices |
|
11. |
The performance of reused SUDs must be overseen by a designated Reprocessing and Reuse Committee within each hospital, accountable for safety and compliance. As per institutional SOP, this responsibility may also be delegated to an approved third party |
|
12. |
Accreditation bodies play a critical role in implementing the safe practice of the reuse of SUDs. Accreditation bodies have recommendations, validate the SOPs stated by the institutions. They also conduct inspections to check whether the SOPs are followed |
|
13. |
Devices used on patients with identified biohazards should ideally not be reused |
|
14. |
Further in-vivo and in-vitro research is required to generate evidence-based support for the reuse of single-use devices (SUDs), ensuring their safety and functionality following proper reprocessing |
|
15. |
In accordance with the Drugs and Cosmetics Act, single-use medical devices must be used strictly as per the manufacturer's instructions, which typically specify one-time use only[66] |
|
16. |
Patients must be clearly informed if any SUDs are being reused during an IR procedure. Informed consent is essential to respect patient autonomy and ensure ethical transparency |
|
17. |
There is a reuse or intention to reuse of SUDs globally for different reasons |
|
18. |
Medical professionals utilizing the devices, researchers, hospital management, quality assurance teams, refurbishers, manufacturers, insurance companies, accreditation organizations, and government authorities are the stakeholders involved in enhancing the reuse of materials |
|
19. |
Reuse of SUD may be considered based on the economy and environmental safety, but should be appropriately regulated. “REUSE BUT REGULATE |
Abbreviations
-
ANVISA—Agência Nacional de Vigilância Sanitária
-
CADTH—Canadian Agency for Drugs and Technologies in Health
-
CDC—United States Centers for Disease Control and Prevention
-
CDSCO—Central Drugs Standard Control Organization
-
CFDA—China Food and Drug Administration
-
CO2—Carbon dioxide
-
CO2e—Carbon dioxide equivalent
-
CVIR—Cardiovascular and interventional radiology
-
EMA—European Medicines Agency
-
EU—European Union
-
FDA—United States Food and Drug Administration
-
IR—Interventional radiology
-
ISVIR—Indian Society of Vascular and Interventional Radiology
-
JCI—Joint Commission International
-
MDA—Medical Device Authority
-
MDR—Medical Device Regulation
-
MHRF—Medical Healthcare Regulatory Framework
-
MHRA—Medicines and Healthcare products Regulatory Agency
-
NABH—National Accreditation Board for Hospitals and Healthcare Providers
-
NABH MIS—NABH Minimal Invasive Surgery (Standards)
-
PMDA—Pharmaceuticals and Medical Devices Agency
-
PR-SUD—Potentially reusable single-use device.
-
Ref—Reference
-
RFID—Radio-frequency identification
-
R-SUD—Reusable single-use device
-
RUD—Reusable medical device
-
SAHPRA—South African Health Products Regulatory Authority
-
SFDA—Saudi Food and Drug Authority
-
SOP—Standard operating procedure
-
SUD—Single-use device
-
TGA—Therapeutic Goods Administration
-
TJLB—Transjugular liver biopsy
-
UK MHRA—United Kingdom Medicines and Healthcare Products Regulatory Agency
-
US—United States
-
USFDA—United States Food and Drug Administration
-
UPTODATE—UpToDate (Clinical Decision Support Resource)
-
WHO—World Health Organization
Conflict of Interest
None declared.
Acknowledgment
The authors gratefully acknowledge Dr. Shoban H. for his valuable assistance in proofreading the manuscript. No external financial support was received for this work.
-
References
- 1 Single-Use Medical Devices. Accessed May 25, 2025 at: https://assets.publishing.service.gov.uk/media/5bab562040f0b606568f6dc6/Single_use_medical_devices_leaflet_250918.pdf
- 2 Sullivan GM, Artino Jr AR. Analyzing and interpreting data from Likert-type scales. J Grad Med Educ 2013; 5 (04) 541-542
- 3 Likert. Accessed August 17, 2025 at: https://legacy.voteview.com/pdf/Likert_1932.pdf
- 4 GRADE 指南 | UpToDate临床顾问. Accessed August 17, 2025. https://www.uptodate.cn/home/Grading-Guide
- 5 Reprocessed Single-Use Devices: Frequently Asked Questions. FDA. Published online August 1, 2024. Accessed May 19, 2025 at: https://www.fda.gov/medical-devices/reprocessing-single-use-medical-devices-information-health-care-facilities/reprocessed-single-use-devices-frequently-asked-questions
- 6 Bowness P. Symbols to be used on labelling (ISO 15223) & Information to be provided by the manufacturer (ISO 20417). Published online 2020
- 7 Step-by-Step Guide. Accessed August 1, 2025 at: https://eu.bd.com/emea-peripheral-interventions/lib/asset/230.pdf
- 8 Position Statement. Accessed August 1, 2025 at: https://cjic.ca/pdfs/winter2020/POSITION_STATEMENT-Reprossing_of%20Critical_and_Semi-Critical_Devices_in_Community_Healthcare_Settings.pdf
- 9 Jacobs P, Polisena J, Hailey D, Lafferty S. Economic analysis of reprocessing single-use medical devices: a systematic literature review. Infect Control Hosp Epidemiol 2008; 29 (04) 297-301
- 10 White Paper: Reuse of Single-Use Devices. Joint Commission International. Accessed August 1, 2025 at: https://www.jointcommission.org/en/products-and-services/publications/white-papers/reuse-of-single-use-devices
- 11 Landro L. Hospitals Reuse Medical Devices To Lower Costs. Wall Street Journal. Accessed August 1, 2025 at: https://www.wsj.com/articles/SB120588469924246975 . March 19, 2008
- 12 Azizi J, Basile RJ. Doubt and proof: the need to verify the cleaning process. Biomed Instrum Technol 2012; 46 (Suppl): 49-54
- 13 Shuman EK, Chenoweth CE. Reuse of medical devices: implications for infection control. Infect Dis Clin North Am 2012; 26 (01) 165-172
- 14 CDC. Reuse of Single-Use Medical Devices. Infection Control. March 13, 2024. Accessed August 2, 2025 at: https://www.cdc.gov/infection-control/hcp/disinfection-sterilization/reuse-single-use-devices.html
- 15 Ischinger TA, Neubauer G, Ujlaky R, Schätzl H, Bock M. [Reuse of “single use” medical devices after quality assured reprocessing: hygienic, legal and economic aspects. Potential for cost savings in interventional cardiology]. Z Kardiol 2002; 91 (11) 889-898
- 16 Reduce, Reuse, Recycle: Reprocessing Medical Devices. Hospital Management. March 30, 2010. Accessed August 1, 2025 at: https://www.hospitalmanagement.net/features/feature80981/
- 17 AORN Position Statements. Accessed August 1, 2025 at: https://www.aorn.org/docs/default-source/guidelines-resources/position-statements/patient-workplace-safety/poststat-envirresp-022525.pdf
- 18 Keil M, Viere T, Helms K, Rogowski W. The impact of switching from single-use to reusable healthcare products: a transparency checklist and systematic review of life-cycle assessments. Eur J Public Health 2023; 33 (01) 56-63
- 19 Chua ALB, Amin R, Zhang J, Thiel CL, Gross JS. The environmental impact of interventional radiology: an evaluation of greenhouse gas emissions from an academic interventional radiology practice. J Vasc Interv Radiol 2021; 32 (06) 907-915.e3
- 20 Shum PL, Kok HK, Maingard J. et al. Sustainability in interventional radiology: are we doing enough to save the environment?. CVIR Endovasc 2022; 5 (01) 60
- 21 Reuse of Single-Use Medical Devices. Accessed August 1, 2025 at: https://www.govinfo.gov/content/pkg/CHRG-106hhrg62970/html/CHRG-106hhrg62970.htm
- 22 Miyake M. Remanufactured-Single Use Device in Japan. Available at:. https://www.pmda.go.jp/files/000266828.pdf
- 23 Australian Regulatory Guidelines for Medical Devices. Published online 2011. Available at: https://www.tga.gov.au/sites/default/files/devices-argmd-01.pdf
- 24 Therapeutic Goods Administration (TGA). Labelling medical devices to meet regulatory requirements | Therapeutic Goods Administration (TGA). September 24, 2024. Accessed August 3, 2025 at: https://www.tga.gov.au/resources/guidance/labelling-medical-devices-meet-regulatory-requirements
- 25 Therapeutic Goods Amendment (2020, Measures No. 2) Bill 2020. Accessed August 3, 2025 at: https://www.aph.gov.au/Parliamentary_Business/Bills_Legislation/bd/bd2021a/21bd045
- 26 Reprocessing of Reusable Medical Devices. Australian Commission on Safety and Quality in Health Care. . Accessed August 3, 2025 at: https://www.safetyandquality.gov.au/our-work/infection-prevention-and-control/reprocessing-reusable-medical-devices
- 27 Single-Use Medical Devices. Accessed August 1, 2025 at: https://assets.publishing.service.gov.uk/media/60117a378fa8f565559191cd/Single_use_medical_devices.pdf
- 28 Single-Use Medical Devices. Accessed August 3, 2025 at: https://assets.publishing.service.gov.uk/media/5a80245e40f0b62305b896df/Single-use_medical_devices_-_UK_guidance_on_re-manufacturing_-_draft.pdf
- 29 Reprocessing Single-Use Medical Devices. Information for Health Care Facilities. FDA. August 1, 2024. Accessed August 3, 2025 at: https://www.fda.gov/medical-devices/products-and-medical-procedures/reprocessing-single-use-medical-devices-information-health-care-facilities
- 30 Areté, European Health and Digital Executive Agency (European Commission), Gesundheit Österreich GmbH, et al. Study on the Implementation of Article 17 of Regulation (EU) 2017/745 on Medical Devices on the EU Market: Final Report. Publications Office of the European Union; 2024. . Accessed August 3, 2025. https://data.europa.eu/doi/10.2925/210943
- 31 Donnelly S. Medical Devices Regulations 202. Available at:. https://www.irishstatutebook.ie/eli/2021/si/261/made/en/print
- 32 National Rules on Reprocessing of Single-Use Devices—European Commission. August 1, 2025. Accessed August 3, 2025 at: https://health.ec.europa.eu/medical-devices-topics-interest/reprocessing-devices/national-rules-reprocessing-single-use-devices_en
- 33 Förordning. (2021:631) med kompletterande bestämmelser till EU:s förordningar om medicintekniska produkter | Sveriges riksdag. Accessed August 17, 2025 at: https://www.riksdagen.se/sv/dokument-och-lagar/dokument/svensk-forfattningssamling/forordning-2021631-med-kompletterande_sfs-2021-631/
- 34 Reprocessing of Critical and Semi-Critical Devices in the Community. Accessed August 17, 2025 at: https://ipac-canada.org/wp-content/uploads/2025/03/Reprocessing-of-Critical-and-Semi-Critical-Devices-in-the-Community_Pos._6Nov2019-1-FINAL.pdf
- 35 Canada's Drug Agency. CDA-AMC. Accessed August 17, 2025 at: https://www.cda-amc.ca/
- 36 Update: Notice to Stakeholders. Health Canada's Regulatory Approach to Commercial Reprocessing of Medical Devices Originally Labelled for Single Use. February 5, 2015. Accessed August 17, 2025 at: https://www.canada.ca/en/health-canada/services/drugs-health-products/medical-devices/activities/announcements/update-notice-stakeholders-regulatory-approach-commercial-reprocessing-medical-devices-originally-labelled-single-use.html
- 37 Product. CSA Group. Accessed August 3, 2025 at: https://www.csagroup.org/store/product/2704392/?srsltid=AfmBOopLvlRPVNL3qoE5mOutY_dtn_d14oFeQDyIcxKrTcw48ne6GArx
- 38 Lee SS, Salole E. Medical device reimbursement coverage and pricing rules in Korea: current practice and issues with access to innovation. Value Health 2014; 17 (04) 476-481
- 39 National Medical Products Administration. Accessed August 17, 2025 at: https://english.nmpa.gov.cn/
- 40 Reprocessing and Reuse of Single-Use Medical Devices in China: A Pilot Survey. BMC Public Health. Accessed August 3, 2025 at: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-019-6835-9
- 41 MDSysExcE.pdf. Accessed August 3, 2025 at: https://www.sfda.gov.sa/sites/default/files/2023-10/MDSysExcE.pdf
- 42 Reprocessing of Single-Use Medical Devices. Accessed August 3, 2025 at: https://www.sahpra.org.za/wp-content/uploads/2020/01/Reprocessing-of-Single-Use-Medical-Devices_Communication-to-Stakeholders_Nov2019.pdf
- 43 Jacobs P, Akpinar I. Single-use medical devices: economic issues. Heart Asia 2018; 10 (02) e011034
- 44 White Paper on Reuse of Single-Use Medical Devices. Accessed August 17, 2025 at: https://www.dakshamahealth.org/assets/report/White_Paper_on_reuse_of_single_use_medical_devices.pdf
- 45 Costa EAM. Panorama internacional do reprocessamento de produtos médicos de uso único. Rev SOBECC 2016; 21 (04) 203-209
- 46 World Health Organization, 2016. Decontamination and Reprocessing of Medical Device. Accessed August 17, 2025. https://iris.who.int/bitstream/handle/10665/250232/9789241549851-eng.pdf?sequence=1
- 47 WHO-UHL-IHS-IPC-2022. Accessed August 3, 2025. https://iris.who.int/bitstream/handle/10665/364587/WHO-UHL-IHS-IPC-2022.4-eng.pdf
- 48 Kapoor A, Vora A, Nataraj G, Mishra S, Kerkar P, Manjunath CN. Guidance on reuse of cardio-vascular catheters and devices in India: a consensus document. Indian Heart J 2017; 69 (03) 357-363
- 49 Guidelines for Perioperative Practice. AORN. Accessed August 17, 2025. https://www.aorn.org/guidelines-resources/guidelines-for-perioperative-practice
- 50 Reprocessing Single-Use Devices. Accessed August 17, 2025. https://text.apic.org/toc/basic-principles-of-infection-prevention-practice/reprocessing-single-use-devices
- 51 ACOG Committee Opinion No. ACOG Committee Opinion No. 769: Reprocessed Single-Use Devices. Obstet Gynecol 2019; 133 (03) e235-e237
- 52 Position Statement: Reuse of Single-Use Devices: Responsible Recycling of Medical Instrumentation. American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS). September 17, 2016. Accessed August 17, 2025. https://www.entnet.org/resource/position-statement-reuse-of-single-use-devices-responsible-recycling-of-medical-instrumentation/
- 53 Ghorai RP, Kumar R. Reuse of single-use devices in endourology: a review. Published online 2023.
- 54 Reuse of Single-Use Critical Medical Devices: Position Statement. Accessed August 17, 2025. https://www.sgna.org/portals/0/single%20use%20devices_final.pdf
- 55 Single use devices. Available at:. https://www.acipc.org.au/wp-content/uploads/2025/07/Position-Statement-Single-use-Devices-Jul-25.pdf
- 56 AST Guidelines for Best Practices in the Reuse of Single-Use Devices in Surgery. Accessed August 17, 2025 at: https://www.ast.org/uploadedFiles/Main_Site/Content/About_Us/Guideline_Single-Use_Devices.pdf
- 57 Tsay EL, Sabharwal S. Reuse of orthopaedic equipment: barriers and opportunities. JBJS Rev 2024; 12 (03)
- 58 Rashad SS, Ismail GA, Kassem NN, Baghagho E, El-Etriby A. Cardiac Catheters Reprocessing for Limited Resources Hospitals: An Experimental Study. Published online 2015. Available at: https://www.ijcmas.com/vol-4-11/Samar%20S.Rashad,%20et%20al.pdf
- 59 Amarante JMB, Toscano CM, Pearson ML, Roth V, Jarvis WR, Levin AS. Reprocessing and reuse of single-use medical devices used during hemodynamic procedures in Brazil: a widespread and largely overlooked problem. Infect Control Hosp Epidemiol 2008; 29 (09) 854-858
- 60 Browne KF, Maldonado R, Telatnik M, Vlietstra RE, Brenner AS. Initial experience with reuse of coronary angioplasty catheters in the United States. J Am Coll Cardiol 1997; 30 (07) 1735-1740
- 61 Decontamination and Reprocessing of Medical Devices for Health-Care Facilities. Accessed August 1, 2025 at: https://www.who.int/publications/i/item/9789241549851
- 62 Hailey D, Jacobs PD, Ries NM, Polisena J. Reuse of single use medical devices in Canada: clinical and economic outcomes, legal and ethical issues, and current hospital practice. Int J Technol Assess Health Care 2008; 24 (04) 430-436
- 63 Kuruoğlu T, Önger ME, Altun G, Atilla A, Esen Ş. Detrimental effects of sterilization types on single-use coronary angioplasty catheters for reuse: an electron microscopic study. Infect Dis Clin Microbiol 2024; 6 (01) 4-10
- 64 Myrna F, Oliveira DC, Vinhas G, Silva I, Teixeira M, Galembeck A. Reprocessing of catheters used for coronary angiography and changes in the polymeric structures. Cardiol Res 2018; 9 (05) 300-306
- 65 Draft Standards for MIS. 2nd edition.pdf. Available at: https://testing.nabh.co/wp-content/uploads/2025/07/5.-Standards-for-MIS-2nd-Edition_Edited.pdf
- 66 Medical Devices Rules. Accessed August 2, 2025 at: https://cdsco.gov.in/opencms/resources/UploadCDSCOWeb/2022/m_device/Medical%20Devices%20Rules,%202017.pdf
- 67 Addendum02faqmd.pdf. Accessed August 2, 2025 at: https://cdsco.gov.in/opencms/export/sites/CDSCO_WEB/Pdf-documents/Addendum02faqmd.pdf
- 68 Flowers D, Flowers D. The environmental impact of IR: a matter of concern?. Cardiovasc Intervent Radiol 2020; 43 (06) 916-917
- 69 Sumner C, Sumner C, Ikuta I. et al. Approaches to greening radiology. Acad Radiol 2022;
- 70 Brassil MP, Torreggiani WC. Recycling in IR, what IR specialists can do to help. Cardiovasc Intervent Radiol 2019; 42 (06) 789-790
- 71 Chawla A, Chinchure D, Marchinkow LO, Munk PL, Peh WCG. Greening the radiology department: not a big mountain to climb. Can Assoc Radiol J 2017; 68 (03) 234-236
- 72 Popp W, Rasslan O, Unahalekhaka A. et al. What is the use? An international look at reuse of single-use medical devices. Int J Hyg Environ Health 2010; 213 (04) 302-307
- 73 Bayrak T, Bayrak T, Bayrak T, Soylu SI, Soylu SI. Reprocessing of single use medical devices: a new proposal for a regulation. Health Policy Technol 2021;
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
06. Januar 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Single-Use Medical Devices. Accessed May 25, 2025 at: https://assets.publishing.service.gov.uk/media/5bab562040f0b606568f6dc6/Single_use_medical_devices_leaflet_250918.pdf
- 2 Sullivan GM, Artino Jr AR. Analyzing and interpreting data from Likert-type scales. J Grad Med Educ 2013; 5 (04) 541-542
- 3 Likert. Accessed August 17, 2025 at: https://legacy.voteview.com/pdf/Likert_1932.pdf
- 4 GRADE 指南 | UpToDate临床顾问. Accessed August 17, 2025. https://www.uptodate.cn/home/Grading-Guide
- 5 Reprocessed Single-Use Devices: Frequently Asked Questions. FDA. Published online August 1, 2024. Accessed May 19, 2025 at: https://www.fda.gov/medical-devices/reprocessing-single-use-medical-devices-information-health-care-facilities/reprocessed-single-use-devices-frequently-asked-questions
- 6 Bowness P. Symbols to be used on labelling (ISO 15223) & Information to be provided by the manufacturer (ISO 20417). Published online 2020
- 7 Step-by-Step Guide. Accessed August 1, 2025 at: https://eu.bd.com/emea-peripheral-interventions/lib/asset/230.pdf
- 8 Position Statement. Accessed August 1, 2025 at: https://cjic.ca/pdfs/winter2020/POSITION_STATEMENT-Reprossing_of%20Critical_and_Semi-Critical_Devices_in_Community_Healthcare_Settings.pdf
- 9 Jacobs P, Polisena J, Hailey D, Lafferty S. Economic analysis of reprocessing single-use medical devices: a systematic literature review. Infect Control Hosp Epidemiol 2008; 29 (04) 297-301
- 10 White Paper: Reuse of Single-Use Devices. Joint Commission International. Accessed August 1, 2025 at: https://www.jointcommission.org/en/products-and-services/publications/white-papers/reuse-of-single-use-devices
- 11 Landro L. Hospitals Reuse Medical Devices To Lower Costs. Wall Street Journal. Accessed August 1, 2025 at: https://www.wsj.com/articles/SB120588469924246975 . March 19, 2008
- 12 Azizi J, Basile RJ. Doubt and proof: the need to verify the cleaning process. Biomed Instrum Technol 2012; 46 (Suppl): 49-54
- 13 Shuman EK, Chenoweth CE. Reuse of medical devices: implications for infection control. Infect Dis Clin North Am 2012; 26 (01) 165-172
- 14 CDC. Reuse of Single-Use Medical Devices. Infection Control. March 13, 2024. Accessed August 2, 2025 at: https://www.cdc.gov/infection-control/hcp/disinfection-sterilization/reuse-single-use-devices.html
- 15 Ischinger TA, Neubauer G, Ujlaky R, Schätzl H, Bock M. [Reuse of “single use” medical devices after quality assured reprocessing: hygienic, legal and economic aspects. Potential for cost savings in interventional cardiology]. Z Kardiol 2002; 91 (11) 889-898
- 16 Reduce, Reuse, Recycle: Reprocessing Medical Devices. Hospital Management. March 30, 2010. Accessed August 1, 2025 at: https://www.hospitalmanagement.net/features/feature80981/
- 17 AORN Position Statements. Accessed August 1, 2025 at: https://www.aorn.org/docs/default-source/guidelines-resources/position-statements/patient-workplace-safety/poststat-envirresp-022525.pdf
- 18 Keil M, Viere T, Helms K, Rogowski W. The impact of switching from single-use to reusable healthcare products: a transparency checklist and systematic review of life-cycle assessments. Eur J Public Health 2023; 33 (01) 56-63
- 19 Chua ALB, Amin R, Zhang J, Thiel CL, Gross JS. The environmental impact of interventional radiology: an evaluation of greenhouse gas emissions from an academic interventional radiology practice. J Vasc Interv Radiol 2021; 32 (06) 907-915.e3
- 20 Shum PL, Kok HK, Maingard J. et al. Sustainability in interventional radiology: are we doing enough to save the environment?. CVIR Endovasc 2022; 5 (01) 60
- 21 Reuse of Single-Use Medical Devices. Accessed August 1, 2025 at: https://www.govinfo.gov/content/pkg/CHRG-106hhrg62970/html/CHRG-106hhrg62970.htm
- 22 Miyake M. Remanufactured-Single Use Device in Japan. Available at:. https://www.pmda.go.jp/files/000266828.pdf
- 23 Australian Regulatory Guidelines for Medical Devices. Published online 2011. Available at: https://www.tga.gov.au/sites/default/files/devices-argmd-01.pdf
- 24 Therapeutic Goods Administration (TGA). Labelling medical devices to meet regulatory requirements | Therapeutic Goods Administration (TGA). September 24, 2024. Accessed August 3, 2025 at: https://www.tga.gov.au/resources/guidance/labelling-medical-devices-meet-regulatory-requirements
- 25 Therapeutic Goods Amendment (2020, Measures No. 2) Bill 2020. Accessed August 3, 2025 at: https://www.aph.gov.au/Parliamentary_Business/Bills_Legislation/bd/bd2021a/21bd045
- 26 Reprocessing of Reusable Medical Devices. Australian Commission on Safety and Quality in Health Care. . Accessed August 3, 2025 at: https://www.safetyandquality.gov.au/our-work/infection-prevention-and-control/reprocessing-reusable-medical-devices
- 27 Single-Use Medical Devices. Accessed August 1, 2025 at: https://assets.publishing.service.gov.uk/media/60117a378fa8f565559191cd/Single_use_medical_devices.pdf
- 28 Single-Use Medical Devices. Accessed August 3, 2025 at: https://assets.publishing.service.gov.uk/media/5a80245e40f0b62305b896df/Single-use_medical_devices_-_UK_guidance_on_re-manufacturing_-_draft.pdf
- 29 Reprocessing Single-Use Medical Devices. Information for Health Care Facilities. FDA. August 1, 2024. Accessed August 3, 2025 at: https://www.fda.gov/medical-devices/products-and-medical-procedures/reprocessing-single-use-medical-devices-information-health-care-facilities
- 30 Areté, European Health and Digital Executive Agency (European Commission), Gesundheit Österreich GmbH, et al. Study on the Implementation of Article 17 of Regulation (EU) 2017/745 on Medical Devices on the EU Market: Final Report. Publications Office of the European Union; 2024. . Accessed August 3, 2025. https://data.europa.eu/doi/10.2925/210943
- 31 Donnelly S. Medical Devices Regulations 202. Available at:. https://www.irishstatutebook.ie/eli/2021/si/261/made/en/print
- 32 National Rules on Reprocessing of Single-Use Devices—European Commission. August 1, 2025. Accessed August 3, 2025 at: https://health.ec.europa.eu/medical-devices-topics-interest/reprocessing-devices/national-rules-reprocessing-single-use-devices_en
- 33 Förordning. (2021:631) med kompletterande bestämmelser till EU:s förordningar om medicintekniska produkter | Sveriges riksdag. Accessed August 17, 2025 at: https://www.riksdagen.se/sv/dokument-och-lagar/dokument/svensk-forfattningssamling/forordning-2021631-med-kompletterande_sfs-2021-631/
- 34 Reprocessing of Critical and Semi-Critical Devices in the Community. Accessed August 17, 2025 at: https://ipac-canada.org/wp-content/uploads/2025/03/Reprocessing-of-Critical-and-Semi-Critical-Devices-in-the-Community_Pos._6Nov2019-1-FINAL.pdf
- 35 Canada's Drug Agency. CDA-AMC. Accessed August 17, 2025 at: https://www.cda-amc.ca/
- 36 Update: Notice to Stakeholders. Health Canada's Regulatory Approach to Commercial Reprocessing of Medical Devices Originally Labelled for Single Use. February 5, 2015. Accessed August 17, 2025 at: https://www.canada.ca/en/health-canada/services/drugs-health-products/medical-devices/activities/announcements/update-notice-stakeholders-regulatory-approach-commercial-reprocessing-medical-devices-originally-labelled-single-use.html
- 37 Product. CSA Group. Accessed August 3, 2025 at: https://www.csagroup.org/store/product/2704392/?srsltid=AfmBOopLvlRPVNL3qoE5mOutY_dtn_d14oFeQDyIcxKrTcw48ne6GArx
- 38 Lee SS, Salole E. Medical device reimbursement coverage and pricing rules in Korea: current practice and issues with access to innovation. Value Health 2014; 17 (04) 476-481
- 39 National Medical Products Administration. Accessed August 17, 2025 at: https://english.nmpa.gov.cn/
- 40 Reprocessing and Reuse of Single-Use Medical Devices in China: A Pilot Survey. BMC Public Health. Accessed August 3, 2025 at: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-019-6835-9
- 41 MDSysExcE.pdf. Accessed August 3, 2025 at: https://www.sfda.gov.sa/sites/default/files/2023-10/MDSysExcE.pdf
- 42 Reprocessing of Single-Use Medical Devices. Accessed August 3, 2025 at: https://www.sahpra.org.za/wp-content/uploads/2020/01/Reprocessing-of-Single-Use-Medical-Devices_Communication-to-Stakeholders_Nov2019.pdf
- 43 Jacobs P, Akpinar I. Single-use medical devices: economic issues. Heart Asia 2018; 10 (02) e011034
- 44 White Paper on Reuse of Single-Use Medical Devices. Accessed August 17, 2025 at: https://www.dakshamahealth.org/assets/report/White_Paper_on_reuse_of_single_use_medical_devices.pdf
- 45 Costa EAM. Panorama internacional do reprocessamento de produtos médicos de uso único. Rev SOBECC 2016; 21 (04) 203-209
- 46 World Health Organization, 2016. Decontamination and Reprocessing of Medical Device. Accessed August 17, 2025. https://iris.who.int/bitstream/handle/10665/250232/9789241549851-eng.pdf?sequence=1
- 47 WHO-UHL-IHS-IPC-2022. Accessed August 3, 2025. https://iris.who.int/bitstream/handle/10665/364587/WHO-UHL-IHS-IPC-2022.4-eng.pdf
- 48 Kapoor A, Vora A, Nataraj G, Mishra S, Kerkar P, Manjunath CN. Guidance on reuse of cardio-vascular catheters and devices in India: a consensus document. Indian Heart J 2017; 69 (03) 357-363
- 49 Guidelines for Perioperative Practice. AORN. Accessed August 17, 2025. https://www.aorn.org/guidelines-resources/guidelines-for-perioperative-practice
- 50 Reprocessing Single-Use Devices. Accessed August 17, 2025. https://text.apic.org/toc/basic-principles-of-infection-prevention-practice/reprocessing-single-use-devices
- 51 ACOG Committee Opinion No. ACOG Committee Opinion No. 769: Reprocessed Single-Use Devices. Obstet Gynecol 2019; 133 (03) e235-e237
- 52 Position Statement: Reuse of Single-Use Devices: Responsible Recycling of Medical Instrumentation. American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS). September 17, 2016. Accessed August 17, 2025. https://www.entnet.org/resource/position-statement-reuse-of-single-use-devices-responsible-recycling-of-medical-instrumentation/
- 53 Ghorai RP, Kumar R. Reuse of single-use devices in endourology: a review. Published online 2023.
- 54 Reuse of Single-Use Critical Medical Devices: Position Statement. Accessed August 17, 2025. https://www.sgna.org/portals/0/single%20use%20devices_final.pdf
- 55 Single use devices. Available at:. https://www.acipc.org.au/wp-content/uploads/2025/07/Position-Statement-Single-use-Devices-Jul-25.pdf
- 56 AST Guidelines for Best Practices in the Reuse of Single-Use Devices in Surgery. Accessed August 17, 2025 at: https://www.ast.org/uploadedFiles/Main_Site/Content/About_Us/Guideline_Single-Use_Devices.pdf
- 57 Tsay EL, Sabharwal S. Reuse of orthopaedic equipment: barriers and opportunities. JBJS Rev 2024; 12 (03)
- 58 Rashad SS, Ismail GA, Kassem NN, Baghagho E, El-Etriby A. Cardiac Catheters Reprocessing for Limited Resources Hospitals: An Experimental Study. Published online 2015. Available at: https://www.ijcmas.com/vol-4-11/Samar%20S.Rashad,%20et%20al.pdf
- 59 Amarante JMB, Toscano CM, Pearson ML, Roth V, Jarvis WR, Levin AS. Reprocessing and reuse of single-use medical devices used during hemodynamic procedures in Brazil: a widespread and largely overlooked problem. Infect Control Hosp Epidemiol 2008; 29 (09) 854-858
- 60 Browne KF, Maldonado R, Telatnik M, Vlietstra RE, Brenner AS. Initial experience with reuse of coronary angioplasty catheters in the United States. J Am Coll Cardiol 1997; 30 (07) 1735-1740
- 61 Decontamination and Reprocessing of Medical Devices for Health-Care Facilities. Accessed August 1, 2025 at: https://www.who.int/publications/i/item/9789241549851
- 62 Hailey D, Jacobs PD, Ries NM, Polisena J. Reuse of single use medical devices in Canada: clinical and economic outcomes, legal and ethical issues, and current hospital practice. Int J Technol Assess Health Care 2008; 24 (04) 430-436
- 63 Kuruoğlu T, Önger ME, Altun G, Atilla A, Esen Ş. Detrimental effects of sterilization types on single-use coronary angioplasty catheters for reuse: an electron microscopic study. Infect Dis Clin Microbiol 2024; 6 (01) 4-10
- 64 Myrna F, Oliveira DC, Vinhas G, Silva I, Teixeira M, Galembeck A. Reprocessing of catheters used for coronary angiography and changes in the polymeric structures. Cardiol Res 2018; 9 (05) 300-306
- 65 Draft Standards for MIS. 2nd edition.pdf. Available at: https://testing.nabh.co/wp-content/uploads/2025/07/5.-Standards-for-MIS-2nd-Edition_Edited.pdf
- 66 Medical Devices Rules. Accessed August 2, 2025 at: https://cdsco.gov.in/opencms/resources/UploadCDSCOWeb/2022/m_device/Medical%20Devices%20Rules,%202017.pdf
- 67 Addendum02faqmd.pdf. Accessed August 2, 2025 at: https://cdsco.gov.in/opencms/export/sites/CDSCO_WEB/Pdf-documents/Addendum02faqmd.pdf
- 68 Flowers D, Flowers D. The environmental impact of IR: a matter of concern?. Cardiovasc Intervent Radiol 2020; 43 (06) 916-917
- 69 Sumner C, Sumner C, Ikuta I. et al. Approaches to greening radiology. Acad Radiol 2022;
- 70 Brassil MP, Torreggiani WC. Recycling in IR, what IR specialists can do to help. Cardiovasc Intervent Radiol 2019; 42 (06) 789-790
- 71 Chawla A, Chinchure D, Marchinkow LO, Munk PL, Peh WCG. Greening the radiology department: not a big mountain to climb. Can Assoc Radiol J 2017; 68 (03) 234-236
- 72 Popp W, Rasslan O, Unahalekhaka A. et al. What is the use? An international look at reuse of single-use medical devices. Int J Hyg Environ Health 2010; 213 (04) 302-307
- 73 Bayrak T, Bayrak T, Bayrak T, Soylu SI, Soylu SI. Reprocessing of single use medical devices: a new proposal for a regulation. Health Policy Technol 2021;
Green circles indicate countries/regions with established regulatory frameworks for
reuse of SUDs, while red circles indicate the absence of such regulations.