

Subscribe to RSS
DOI: 10.1055/s-0045-1813041
Endoscopic Ultrasound-Guided Tissue Acquisition in Solid Pancreatic Lesions: Fine Needle Aspiration or Fine Needle Biopsy—A Randomized Pilot Study from a Low-Resource Tertiary Care Center
Authors
Funding None.

Abstract
Background
Solid pancreatic mass lesions pose a substantial diagnostic challenge, especially in resource-limited settings. Endoscopic ultrasound (EUS)-guided fine-needle aspiration (EUS-FNA) and fine-needle biopsy (EUS-FNB) are both widely utilized, yet comparative data on their performance under constrained conditions remain limited.
Materials and Methods
In this prospective, randomized, single-center pilot study, patients with suspected solid pancreatic lesions were randomized to undergo either EUS-FNA (n = 20) or EUS-FNB (n = 21). Diagnostic accuracy, sensitivity, specificity, sample cellularity, technical success, adverse events, and total cost (needle + pathological processing) were assessed.
Results
Forty-one patients were randomized. Diagnostic accuracy was slightly higher in the FNB group (95.2%) compared to the FNA group (90%). Sensitivity was similar for FNB (92.9%) and FNA (92.3%), but specificity was greater with FNB (100% vs. 85.7%). Technical success was 100% in both arms, with only minor adverse events reported. Most samples demonstrated moderate to high cellularity in both arms. The estimated cost per procedure was INR 22,200 for FNA and INR 27,400 for FNB.
Conclusion
EUS-FNB demonstrated slightly improved diagnostic yield but was expensive compared to FNA. In resource-limited settings, EUS-FNA offers a cost-effective and reliable first-line diagnostic option. Larger multicenter studies are needed to guide context-appropriate needle selection strategies.
Keywords
endoscopic ultrasound - fine-needle aspiration (FNA) - fine-needle biopsy (FNB) - adenocarcinoma - pancreatic cancerIntroduction
Pancreatic cancer remains one of the most aggressive malignancies globally, characterized by poor prognosis and limited treatment options. In India, the reported incidence ranges from 0.5 to 2.4 per 100,000 women and 0.2 to 1.8 per 100,000 men, although these figures appear to be rising with the increasing westernization of lifestyles.[1] Epidemiological data from tertiary care centers in northern India indicate that pancreatic cancer is a significant contributor to malignant extrahepatic biliary obstruction, comprising up to 18% of cases in one study and representing the predominant malignant etiology of obstructive jaundice (33.6%) in another.[2] [3] Given the high mortality associated with pancreatic cancer, timely and precise diagnostic modalities are essential for improving clinical outcomes.
Endoscopic ultrasound (EUS) has emerged as a pivotal tool for both imaging pancreatic lesions and procuring tissue samples. It demonstrates superior sensitivity for detecting small pancreatic tumors and assessing local vascular involvement compared to computed tomography (CT) and magnetic resonance imaging (MRI), thereby facilitating earlier disease detection.[4] Additionally, EUS offers considerable accuracy in identifying local lymph node involvement.[5] Despite the notable specificity of EUS-guided fine needle aspiration (EUS-FNA), which can approach 100%, its sensitivity varies widely (60–93%) due to factors such as needle caliber, the availability of rapid on-site cytopathological evaluation (ROSE), and procedural techniques. Moreover, in patients with chronic pancreatitis, the diagnostic utility of EUS-FNA may be compromised by an increased risk of false-negative findings.[6]
In response to these challenges, advanced EUS techniques have been explored to enhance diagnostic accuracy, including contrast-enhanced harmonic EUS and real-time elastography EUS. Both modalities, used alone or together, achieve a high negative predictive value (NPV), effectively enhancing diagnostic rates in inconclusive EUS-FNA cases. Recently, EUS-guided fine needle biopsy (EUS-FNB) has been able to obtain more robust histological cores, potentially reducing reliance on on-site cytopathology and decreasing false-negative results.[7] The overall diagnostic accuracy of EUS-FNA/EUE-FNB for solid pancreatic lesions is reported to range from 78 to 95%.[7] However, even EUS-guided tissue sampling may be less sensitive and specific in patients with chronic pancreatitis, with sensitivities reported between 50 and 73.9% and specificities from 73.7 to 100%, depending on the study.[8] [9]
While EUS-FNB may offer marginally higher diagnostic yields, it is typically more expensive than FNA, and the needles are not reusable—constraints that can be prohibitive in resource-limited health care settings. Consequently, EUS-FNA remains the primary investigation modality in many developing countries, especially for patients with a high clinical suspicion of pancreatic malignancy, owing to its relative affordability and widespread availability.
Against this backdrop, the present study aimed to compare the diagnostic accuracy of EUS-FNA and EUS-FNB in patients with solid pancreatic masses. Findings from this investigation may help refine diagnostic strategies and optimize resource allocation in low- and middle-income settings.
Materials and Methods
This was a single-center, prospective, randomized, double-blinded study (patient and statistician were blinded) conducted in a tertiary care teaching institute in eastern India.
Patients
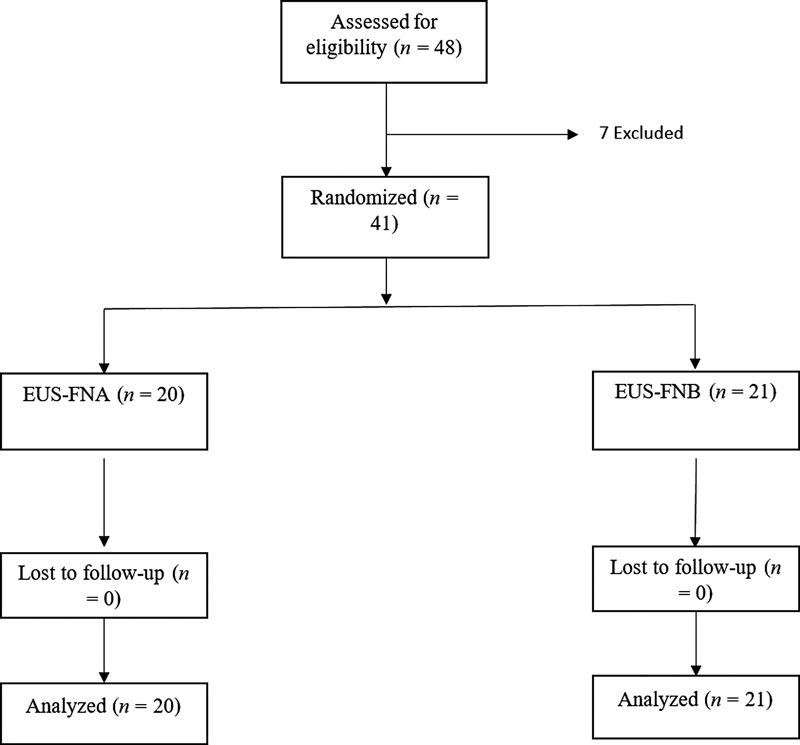
Patients with suspected solid pancreatic lesions, aged between 18 and 80 years, presenting to our department from July 2022 to March 2024, fulfilling the inclusion criteria, were recruited for the study (CONSORT diagram; [Fig. 1]). Diagnosis of solid pancreatic mass was made based on either abdominal ultrasound, abdominal CT scan, or MRI findings. Ethical clearance was obtained from the Institutional Ethics Committee, AIIMS Bhubaneswar (Reference number: IEC/AIIMS BBSR/PG Thesis/2022-23/42, dated June 13, 2022). The trial was registered with CTRI (CTRI/2022/11/047481). Written informed consent was obtained from all participants in their local language.
Patients either aged under 18 years or more than 80 years, had lesions <1 cm in size, had a history of previous gastrectomy or any other gastric surgery, were unable or unwilling to provide informed consent, had uncorrected coagulopathy, had cystic pancreatic lesions, and were critically ill were excluded from the study. All procedures were performed by a single experienced endosonographer (H.K.N.) who had performed more than 500 EUS-FNA before the initiation of this study.
Sample Size Calculation
This trial was prospectively designed as a pilot randomized controlled trial (RCT) to assess feasibility, event rates, and variability for a larger definitive study. Following Browne's guidance for pilot studies, we aimed for about 20 participants per arm (total around 40). No formal hypothesis test was powered in advance; instead, the focus was on the precision (95% confidence intervals) around accuracy estimates to guide planning for the next trial. Effect sizes and variability observed here will help inform a comprehensive, adequately powered multicenter RCT.
Randomization and Blinding
Participants were randomly assigned 1:1 using computer-generated permuted blocks of varying sizes [4 and 6], prepared by an independent coordinator. Allocation was concealed in sequentially numbered, opaque, sealed envelopes, which were opened in the endoscopy suite immediately before needle selection. Patients and the study statistician remained blinded to allocation. The cytopathologist/histopathologist was not blinded due to operational constraints and the potential recognition of core architecture on H&E; this is acknowledged as a study limitation.
Technical Procedure
EUS was performed using a linear array echo-endoscope (GF UCT 180; Olympus Ltd., Tokyo, Japan) connected to an ultrasound unit processor (EUS ME2 Premium plus) by a single endoscopist (H.K.N.). Patients were placed in the left lateral decubitus position under conscious sedation using midazolam and pentazocine injections. After reaching the stomach station, the EUS probe was placed in contact with the gastric wall and the abdominal aorta was identified in an elongated cross-section. This finding was confirmed by color Doppler imaging. The scope was then slowly advanced up to the duodenum when required. EUS evaluation was done from the gastroesophageal junction, duodenal bulb, and second part of the duodenum to screen the entire pancreas and characterize pancreatic lesions. The size, shape, location, echotexture, and vascular encasement of the pancreatic lesion were documented.
A transduodenal approach was used for lesions in the pancreatic head and uncinate process, while a transgastric approach was used for lesions in the body and tail. FNA used a 22-gauge conventional bevel needle; FNB used a 22-gauge multi-blade (Franseen-type) tip. For both arms, we used the same trajectory and fanning technique to limit procedural bias. After puncturing into the deepest part of the lesion, the stylet was withdrawn, an inflation system employing a 60-mL syringe with 50-mL high negative pressure was attached to the proximal end of the needle, and then tissue acquisition was done by the fanning technique with the standard method of 5–10 to-and-fro movements, by application of negative suction.
Crossover/rescue: if the initial allocation yielded paucicellular or nondiagnostic material after the planned passes, a single rescue pass with the alternate needle was allowed at the endoscopist's discretion (documented as crossover). Reuse/sterilization: needles were single-use only; no re-use was performed.
Smears (air-dried/alcohol-fixed) and formalin-fixed material were prepared from each pass; cell blocks were routinely made. All slides/blocks were processed per institutional protocol and reported by the pathologist. Cellularity was graded as follows: paucicellular (<10 diagnostic clusters or <100 lesional cells), low (100–500), moderate (500–2,000), and high (>2,000). Contamination (blood/gastrointestinal epithelium) was semi-quantitatively graded as minimal (<10% slide area), moderate (10–50%), or heavy (>50%). ROSE was not available; Macroscopic on-site evaluation (MOSE) was limited to a macroscopic core assessment, which was not done routinely in our study. In case of scant material aspirated after the first pass, a second pass for tissue acquisition was performed.
Patients were continuously monitored during the procedure with an electrocardiogram tracing and pulse oximetry. All patients were followed for 6 months or till surgery was done, and the surgical specimen biopsy was then correlated with FNA/FNB results. Lesions diagnosed as positive for malignancy with either FNA or FNB and confirmed as positive either by surgical resection or the clinical course of the patient were considered true positives. Lesions diagnosed as benign on EUS-FNA/B and finally confirmed as benign based on the clinical course of the patient were considered true negatives. Aspirates initially diagnosed as benign by EUS-FNA/B but finally diagnosed as malignant either by surgical resection or clinical course of the patient were classified as false negatives. For analysis, inconclusive samples were considered false negatives when comparing diagnostic accuracy.
Primary outcome: diagnostic accuracy for malignancy of index EUS-guided tissue acquisition (FNA vs. FNB) was assessed, adjusted against surgical histology or ≥6-month clinical course.
Secondary outcomes: sensitivity, specificity, positive predictive value (PPV)/NPV; technical success; sample cellularity, adverse events; and procedure total cost (needle + pathology processing) were assessed.
Statistical Analysis
Categorical variables were expressed as frequencies and percentages, while continuous variables were reported as means. The chi-square and Fisher's exact tests were used for categorical variables, and the Student's t-test was employed to compare means between study groups. Continuous variables used the t-test or Mann–Whitney U-test as appropriate for comparison.
Sensitivity, specificity, diagnostic accuracy, and PPVs and NPVs were calculated. Sensitivity was defined as the proportion of true positives correctly identified by the test among cases of malignancy in the study population. Specificity was defined as the proportion of true negatives correctly identified among patients without tumors. The positive likelihood ratio was calculated as sensitivity divided by the false-positive rate, while the negative likelihood ratio was calculated as the false-negative rate divided by specificity. Statistical analysis was performed using SPSS version 23 (IBM, Armonk, New York, United States). Group comparisons of proportions (accuracy, sensitivity, specificity, PPV/NPV) used Fisher's exact test with two-sided α = 0.05; effect sizes are shown as risk difference with 95% CI.
Given the pilot study with a small sample size, we have not done any exploratory logistic regression for correct diagnosis (yes/no), including age, lesion site (head vs. body/tail), size on EUS, bilirubin, CA 1 9-9, and arm (FNA vs. FNB).
The prevalence of solid pancreatic lesions in the Indian subcontinent is not well established. As this was a prospective, randomized pilot study, the sample size was set at 40 subjects, with 20 participants in each group, based on the rules of thumb for pilot studies.[10]
Results
We assessed 48 patients with pancreatic head, body, or tail masses for eligibility. Seven patients were excluded, and 41 patients were randomized into the EUS-FNA and EUS-FNB groups using computer-generated random number sequences. Twenty patients were allocated to the FNA group, while 21 patients were assigned to the FNB group. The patient enrolment and study design are shown in the CONSORT diagram ([Fig. 1]).
The baseline characteristics are summarized in [Table 1]–[2]. The mean age was similar in both groups, with no significant difference. The most common presenting complaint was abdominal pain in both groups. The head of the pancreas was the most common site of the pancreatic mass, occurring in 85% of the FNA group and 61.9% of the FNB group.
Abbreviations: EUS-FNA, Endoscopic ultrasound-guided fine-needle aspiration; EUS-FNB, Endoscopic ultrasound-guided fine-needle biopsy; SD, standard deviation.
Abbreviations: CCP, convoluted cerebriform pattern; CT, computed tomography; EUS-FNA, Endoscopic ultrasound-guided fine-needle aspiration; EUS-FNB, Endoscopic ultrasound-guided fine-needle biopsy; INR, international normalized ratio.
In the EUS-FNA group, 11 patients (55%) were diagnosed with adenocarcinoma based on cytology, while 7 patients (35%) were diagnosed with an inflammatory mass. In the EUS-FNB group, adenocarcinoma was diagnosed in 10 patients (47.6%) on biopsy, while 8 patients (38.1%) had an inflammatory mass (summarized in [Table 3]).
Abbreviations: EUS-FNA, Endoscopic ultrasound-guided fine-needle aspiration; EUS-FNB, Endoscopic ultrasound-guided fine-needle biopsy; SPEN, solid pseudopapillary neoplasm.
Two FNA-allocated cases underwent single-rescue FNB due to initial nondiagnostic/discordant results; one converted to adenocarcinoma, and one remained inflammatory. Analyses were performed by intention-to-treat, counting inconclusive results as false negatives for accuracy.
A total of five patients underwent surgery (Whipple procedure) in the EUS-FNA group, in which adenocarcinoma was the final diagnosis in four patients, while in one patient, an inflammatory mass was seen with no evidence of malignancy.
Similarly, five patients in the FNB group underwent surgery. Four cases had adenocarcinoma as the histological diagnosis, and one case was initially diagnosed with an inflammatory mass. In all five cases, the final histological diagnosis after surgery was adenocarcinoma.
The diagnostic accuracy was 90% in the EUS-FNA group and 95.2% in the EUS-FNB group ([Table 4]). In both groups, most of the patients had moderately cellular samples ([Table 5]).
Abbreviations: EUS-FNA, Endoscopic ultrasound-guided fine-needle aspiration; EUS-FNB, Endoscopic ultrasound-guided fine-needle biopsy.
Note: Values are n/N (%). Group comparisons used Fisher's exact test. CI = 95% confidence interval. No between-group differences were statistically significant.
Abbreviations: EUS-FNA, Endoscopic ultrasound-guided fine-needle aspiration; EUS-FNB, Endoscopic ultrasound-guided fine-needle biopsy.
Between-group differences in diagnostic accuracy (FNA 90.0% vs. FNB 95.2%) and sensitivity (92.3% vs. 92.9%) were not statistically significant (Fisher's exact, p-values >0.05).
Costs were calculated from the provider perspective and included needle + pathology processing (smear, cell-block, histology). The estimated cost per procedure was INR 22,200 for FNA and INR 27,400 for FNB. FNB remained costlier by approximately INR 5,200.
No needle malfunction or mechanical failure was seen, and technical success was 100%.
No severe adverse events were registered. Abdominal pain was seen in two patients (10%) in the EUS-FNA group and three (15%) in the EUS-FNB group. No procedural bleeding was seen in either group. All of the complications were managed conservatively.
Discussion
The diagnostic accuracy of EUS-guided tissue acquisition, whether using FNA or FNB needles, is affected by several factors. These include the sampling technique, the type and size of the needle, the availability of rapid on-site evaluation (ROSE), and the expertise of both the endosonographer and the cytopathologist or histopathologist.[11] There remains a lack of consensus regarding the optimal needle type, emphasizing the need for further studies to clarify how FNA and FNB needles influence diagnostic accuracy and tissue quality.
In this study, diagnostic accuracy was slightly higher in the FNB group (95.2%) compared to the FNA group (90%). Sensitivity was similar in both groups, but specificity was greater with FNB (100% vs. 85.7%). In the absence of ROSE, a common scenario in low-resource settings, achieving high diagnostic accuracy becomes more challenging. EUS-FNA achieved 90% diagnostic accuracy and sensitivity, reinforcing its utility as a frontline tool when performed by experienced endosonographers. Despite EUS-FNB providing marginally better diagnostic accuracy and specificity, EUS-FNA remains a robust and cost-efficient alternative, particularly in settings lacking ROSE.
Various previously published studies have evaluated the diagnostic accuracy of EUS-FNA compared to EUS-FNB.[12] [13] Notably, Wong et al conducted a retrospective study involving 151 patients, which showed a higher diagnostic accuracy for EUS-FNB (94.6%) compared to EUS-FNA (89.6%), although the difference was not statistically significant.[14]
Similarly, a study by Yousri et al and Kuraoka et al observed a slight diagnostic advantage of FNB over FNA, but the difference was not statistically significant.[15] [16] Similarly, another multicenter prospective study with a relatively adequate sample size observed no differences in diagnostic accuracy when smears alone were used.[17]
Cellularity is another critical factor influencing diagnostic success. Both FNA and FNB needles provided sufficient histological cores for diagnosing solid pancreatic lesions. In our study, both arms yielded predominantly moderate to high cellularity samples: 60% in the FNA group and 71% in the FNB group. Although FNB showed a slight advantage, the difference was not statistically significant. This suggests that when the optimal technique is applied, FNA can yield diagnostically sufficient material in the majority of cases, even without typical histological core or ROSE support.
From a cost-effectiveness standpoint, the contrast was more pronounced. The needle cost per procedure for FNB was more than that of FNA (INR 27,400 vs. INR 22,200), resulting in an additional expense for the FNB arm. This cost differential must be carefully weighed, especially in public or resource-limited settings.
Although FNB remains valuable, especially for histologic subtyping or challenging-to-diagnose lesions, our results show that EUS-FNA offers nearly comparable diagnostic performance at a lower cost. These findings are especially important for countries with limited access to advanced cytopathology support or funding for repeat procedures.
The strengths of our study include its prospective, randomized design and focus on real-world limitations, such as cost and lack of ROSE. Limitations include the pilot sample size, single-center design, absence of ROSE, lack of pathologist blinding, procedures performed by a single operator, and the exploratory nature of regression analyses. Cost analysis was limited to direct provider costs and did not account for downstream costs (e.g., repeat procedures). Findings should be validated in adequately powered multicenter studies.
In conclusion, EUS-FNB offers a marginally better diagnostic yield but comes at a higher cost, making EUS-FNA a cost-effective and reliable first-line option in resource-constrained settings. Larger multicenter trials are warranted to establish clearer guidelines for optimal needle selection and sampling strategies, with careful consideration of cost–benefit balance in resource-limited settings.
Conflict of Interest
None declared.
Acknowledgement
The authors acknowledge Dr. Abhijeet, Dr. Harsha Jain, Mr. Santosh, Mr. Debashish, Mrs. Staffey, and Karishma.
Authors' Contributions
H.K.N.: substantial contribution to the conception and design of the study; read, edited, and approved the final manuscript; performed EUS-guided intervention.
S.G., M.C., K.A., S.K., and A.K.G.: substantial contribution to data collection and writing the first draft of the manuscript.
B.P. and R.K.P.: substantial contribution for statistical analysis, extensively edited the manuscript, and revised it critically for important intellectual content.
S.P. and P.M.: pathological reporting.
M.K.P. and S.C.S.: intellectual input and approval of the final manuscript.
All authors read the final manuscript and approved the manuscript.
Patients' Consent
Written informed consent was obtained from all the participating patients.
IEC clearance taken: IEC/AIIMS BBSR/PG Thesis/2022-23/42.
CTRI registration number: CTRI/2022/11/047481.
-
References
- 1 Dhir V, Mohandas KM. Epidemiology of digestive tract cancers in India IV. Gall bladder and pancreas. Indian J Gastroenterol 1999; 18 (01) 24-28
- 2 Sharma V. Profile of malignant extrahepatic biliary obstruction at an Indian tertiary care centre: a dismal picture. ARGH [Internet]. 2017 Jan 19. ;2(4). Accessed January 5, 2025 at: https://juniperpublishers.com/argh/ARGH.MS.ID.555591.php
- 3 Verma S, Sahai S, Gupta P, Munshi A, Verma S, Goyal P. Obstructive jaundice: aetiological spectrum, clinical, biochemical, and radiological evaluation at a tertiary care teaching hospital. Internet J Trop Med 2010 7. 02
- 4 Pancreatic tumors: evaluation with endoscopic US, CT, and MR imaging. Radiology [Internet]. Accessed January 5, 2025 at: https://pubs.rsna.org/radiographics/doi/10.1148/radiology.190.3.8115622
- 5 Warshaw AL, Fernández-del Castillo C. Pancreatic carcinoma. N Engl J Med 1992; 326 (07) 455-465
- 6 Brand B, Pfaff T, Binmoeller KF. et al. Endoscopic ultrasound for differential diagnosis of focal pancreatic lesions, confirmed by surgery. Scand J Gastroenterol 2000; 35 (11) 1221-1228
- 7 Bang JY, Hebert-Magee S, Trevino J, Ramesh J, Varadarajulu S. Randomized trial comparing the 22-gauge aspiration and 22-gauge biopsy needles for EUS-guided sampling of solid pancreatic mass lesions. Gastrointest Endosc 2012; 76 (02) 321-327
- 8 Ngamruengphong S, Li F, Zhou Y, Chak A, Cooper GS, Das A. EUS and survival in patients with pancreatic cancer: a population-based study. Gastrointest Endosc 2010; 72 (01) 78-83 , 83.e1–83.e2
- 9 Othman MO, Wallace MB. The role of endoscopic ultrasonography in the diagnosis and management of pancreatic cancer. Gastroenterol Clin North Am 2012; 41 (01) 179-188
- 10 Browne RH. On the use of a pilot sample for sample size determination. Stat Med 1995; 14 (17) 1933-1940
- 11 Bang JY, Kirtane S, Krall K. et al. In memoriam: fine-needle aspiration, birth: fine-needle biopsy: the changing trend in endoscopic ultrasound-guided tissue acquisition. Dig Endosc 2019; 31 (02) 197-202
- 12 Tian L, Tang AL, Zhang L. et al. Evaluation of 22G fine-needle aspiration (FNA) versus fine-needle biopsy (FNB) for endoscopic ultrasound-guided sampling of pancreatic lesions: a prospective comparison study. Surg Endosc 2018; 32 (08) 3533-3539
- 13 Moura DTH, McCarty TR, Jirapinyo P. et al. Endoscopic ultrasound fine needle aspiration vs fine needle biopsy in solid lesions: a multi-center analysis. World J Clin Cases 2021; 9 (34) 10507-10517
- 14 Wong T, Pattarapuntakul T, Netinatsunton N. et al. Diagnostic performance of endoscopic ultrasound-guided tissue acquisition by EUS-FNA versus EUS-FNB for solid pancreatic mass without ROSE: a retrospective study. World J Surg Oncol 2022; 20 (01) 215
- 15 Yousri M, Abusinna E, Tahoun N, Okasha HH, El-Habashi AH. A comparative study of the diagnostic utility of endoscopic ultrasound-guided fine needle aspiration cytology (EUS-FNA) versus endoscopic ultrasound-guided fine needle biopsy (EUS-FNB) in pancreatic and non-pancreatic lesions. Asian Pac J Cancer Prev 2022; 23 (06) 2151-2158
- 16 Kuraoka N, Hashimoto S, Matsui S, Terai S. Effectiveness of EUS-guided fine-needle biopsy versus EUS-guided fine-needle aspiration: a retrospective analysis. Diagnostics (Basel) 2021; 11 (06) 965
- 17 Okasha HH, Ahmed MY, Ahmed MA. et al. Comparative diagnostic performance of endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) versus endoscopic ultrasound-guided fine-needle biopsy (EUS-FNB) for tissue sampling of solid pancreatic and non-pancreatic lesions without ROSE: a prospective multicenter study. Egypt J Intern Med 2024; 36: 66
Address for correspondence
Publication History
Article published online:
18 November 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Dhir V, Mohandas KM. Epidemiology of digestive tract cancers in India IV. Gall bladder and pancreas. Indian J Gastroenterol 1999; 18 (01) 24-28
- 2 Sharma V. Profile of malignant extrahepatic biliary obstruction at an Indian tertiary care centre: a dismal picture. ARGH [Internet]. 2017 Jan 19. ;2(4). Accessed January 5, 2025 at: https://juniperpublishers.com/argh/ARGH.MS.ID.555591.php
- 3 Verma S, Sahai S, Gupta P, Munshi A, Verma S, Goyal P. Obstructive jaundice: aetiological spectrum, clinical, biochemical, and radiological evaluation at a tertiary care teaching hospital. Internet J Trop Med 2010 7. 02
- 4 Pancreatic tumors: evaluation with endoscopic US, CT, and MR imaging. Radiology [Internet]. Accessed January 5, 2025 at: https://pubs.rsna.org/radiographics/doi/10.1148/radiology.190.3.8115622
- 5 Warshaw AL, Fernández-del Castillo C. Pancreatic carcinoma. N Engl J Med 1992; 326 (07) 455-465
- 6 Brand B, Pfaff T, Binmoeller KF. et al. Endoscopic ultrasound for differential diagnosis of focal pancreatic lesions, confirmed by surgery. Scand J Gastroenterol 2000; 35 (11) 1221-1228
- 7 Bang JY, Hebert-Magee S, Trevino J, Ramesh J, Varadarajulu S. Randomized trial comparing the 22-gauge aspiration and 22-gauge biopsy needles for EUS-guided sampling of solid pancreatic mass lesions. Gastrointest Endosc 2012; 76 (02) 321-327
- 8 Ngamruengphong S, Li F, Zhou Y, Chak A, Cooper GS, Das A. EUS and survival in patients with pancreatic cancer: a population-based study. Gastrointest Endosc 2010; 72 (01) 78-83 , 83.e1–83.e2
- 9 Othman MO, Wallace MB. The role of endoscopic ultrasonography in the diagnosis and management of pancreatic cancer. Gastroenterol Clin North Am 2012; 41 (01) 179-188
- 10 Browne RH. On the use of a pilot sample for sample size determination. Stat Med 1995; 14 (17) 1933-1940
- 11 Bang JY, Kirtane S, Krall K. et al. In memoriam: fine-needle aspiration, birth: fine-needle biopsy: the changing trend in endoscopic ultrasound-guided tissue acquisition. Dig Endosc 2019; 31 (02) 197-202
- 12 Tian L, Tang AL, Zhang L. et al. Evaluation of 22G fine-needle aspiration (FNA) versus fine-needle biopsy (FNB) for endoscopic ultrasound-guided sampling of pancreatic lesions: a prospective comparison study. Surg Endosc 2018; 32 (08) 3533-3539
- 13 Moura DTH, McCarty TR, Jirapinyo P. et al. Endoscopic ultrasound fine needle aspiration vs fine needle biopsy in solid lesions: a multi-center analysis. World J Clin Cases 2021; 9 (34) 10507-10517
- 14 Wong T, Pattarapuntakul T, Netinatsunton N. et al. Diagnostic performance of endoscopic ultrasound-guided tissue acquisition by EUS-FNA versus EUS-FNB for solid pancreatic mass without ROSE: a retrospective study. World J Surg Oncol 2022; 20 (01) 215
- 15 Yousri M, Abusinna E, Tahoun N, Okasha HH, El-Habashi AH. A comparative study of the diagnostic utility of endoscopic ultrasound-guided fine needle aspiration cytology (EUS-FNA) versus endoscopic ultrasound-guided fine needle biopsy (EUS-FNB) in pancreatic and non-pancreatic lesions. Asian Pac J Cancer Prev 2022; 23 (06) 2151-2158
- 16 Kuraoka N, Hashimoto S, Matsui S, Terai S. Effectiveness of EUS-guided fine-needle biopsy versus EUS-guided fine-needle aspiration: a retrospective analysis. Diagnostics (Basel) 2021; 11 (06) 965
- 17 Okasha HH, Ahmed MY, Ahmed MA. et al. Comparative diagnostic performance of endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) versus endoscopic ultrasound-guided fine-needle biopsy (EUS-FNB) for tissue sampling of solid pancreatic and non-pancreatic lesions without ROSE: a prospective multicenter study. Egypt J Intern Med 2024; 36: 66