

Subscribe to RSS
DOI: 10.1055/s-0045-1812894
LCNEC of Nasal Cavity: Diagnostic and Treatment Modalities—Case Report and a Narrative Review
Authors

Abstract
Large cell neuroendocrine carcinoma (LCNEC) of the nasal cavity is a rare epithelial malignancy with only a few cases reported to date. In this article, we present a case report of a 48-year-old male, who presented with a history of epistaxis and nasal blockage for over 1 year and was initially diagnosed as undifferentiated carcinoma further confirmed as LCNEC by histological findings and immunohistochemistry. The patient was managed by neoadjuvant chemotherapy followed by concurrent chemoradiotherapy. After follow-up for 18 months, the patient continues to be in complete clinical, histopathological, and radiological remission. The following report also discusses the rarity, presentation, and various treatment modalities and their outcomes as per current knowledge. Essentially, through this article, we want to highlight the crucial role of the degree of differentiation in such malignancies, the outcome of different treatment modalities used till now, and how these aspects play a crucial role in the treatment and prognosis of such carcinomas.
Introduction
Large cell neuroendocrine carcinoma (LCNEC) is a rare epithelial neuroendocrine malignancy. The most common site is the lung; however, LCNEC might occur at different sites like the gastrointestinal tract, pancreas, cervix, kidney, prostate, larynx, and multiple other primary sites. LCNEC is associated with only 20% 5-year overall survival (OS) according to a Dutch registry (47,800 patients) and the reported incidence was increased by 1.79 per 100,000 people.[1] To the best of our knowledge, there have only been four cases of LCNEC of the nasal cavity described to date, making it an extremely rare condition. For a patient to survive, a cancer with such a rare occurrence and inadequate 5-year OS exploring efficient treatment is crucial. As of now, both radiotherapy and surgery followed by chemoradiotherapy have been adopted as the initial and mainstay treatment modality, but a complete agreement on adequate management is lacking.[2]
Patient Report
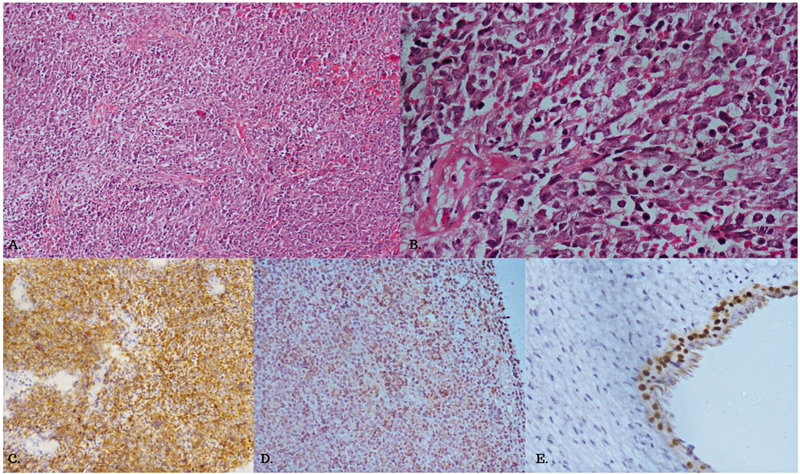
A 48-year-old male patient presented to us with a history of epistaxis and left-sided nasal blockage for almost 1-year duration. The patient was a smoker (15 pack years) and consumed alcohol in moderation. Examination of the left nasal cavity revealed a mass abutting the nasal choana. Nasal endoscopic examination revealed a left sinonasal bleeding polypoidal mass. Endoscopy-guided nasal biopsy was done for histopathological examination. On contrast-enhanced computed tomography (CT) of the neck and face, an ill-defined moderately enhancing solid mass was noticed in the left nasal cavity, ethmoidal air cells, and extending into the nasopharynx posteroinferiorly and laterally into the left orbit through the left lamina papyracea. Fluorodeoxyglucose (FDG)/positron emission tomography (PET) revealed an FDG-avid solid lesion in the left nasal cavity. Microscopic examination of the lesion revealed a tumor composed of sheets of malignant cells having high N:C (nuclear to chromatin ratio), scanty cytoplasm, monomorphic nuclei with stippled chromatin, and few cells showing prominent nucleoli. There was no evidence of prominent nuclear molding, Azzopardi phenomenon, necrosis, keratinization, or brisk mitosis. On immunohistochemistry (IHC), the cells showed positivity for synaptophysin but were negative for Pan CK, p40, and CD45. The proliferation index (Ki-67) was 55 to 60% and p53 was wild-type. A final diagnosis of poorly differentiated LCNEC was confirmed ([Fig. 1]).
The patient was managed with neoadjuvant chemotherapy (NACT) with cisplatin + etoposide, for three cycles (with growth factor support). This was followed by concurrent chemoradiotherapy (CCRT) of 70 Gy divided into 35 fractions, delivered over 6 to 8 weeks along with cisplatin weekly during the radiotherapy. End of therapy PET CT after 12 weeks revealed FDG-avid bilateral neck nodes (standardized uptake value 4.4), while the primary lesion in the left nasal cavity and left ethmoidal air cells were not appreciated. A biopsy was done which showed chronic inflammation without any malignant features. The patient is under regular follow-up with no evidence of recurrence.
Discussion
Accounting for less than 5% of the sinonasal malignancies, LNCEC of the nasal cavity is overall a rare entity. Epistaxis is one of the most common symptoms in the presentation of LCNEC of the nasal cavity. Nasal obstruction, epiphora, and facial pain are the other common symptoms. Local extension to skull base, brain, or nasopharynx can cause symptoms of mass lesion or exophthalmos. In addition to metastases to lungs, bone, or liver, the entity may be associated with paraneoplastic syndrome of inappropriate antidiuretic hormone secretion.[3] [4] Human papilloma virus may be positive in some sinonasal LCNEC and these have aggressive course with poor prognosis.[5] Histopathology and IHC remain the mainstay for the differential diagnosis of NEC with the major histologic feature being the presence of high mitotic activity with > 10 mitoses in 10 high-power fields distinguishing it from moderately differentiated NEC. Other features under microscopy are scant cytoplasm and a high N:C ratio without molding or crush artifacts.[6]
Recently, the suggestion to include LCNEC as an independent category within the classification of head and neck cancers has been put forth by multiple authors rather than categorizing such tumors as NEC-not otherwise specified. Compared to atypical carcinoid tumors, LCNEC has a worse prognosis and behaves aggressively, much like small cell carcinoma.[7] Malignant melanoma, lymphoma, and sinonasal undifferentiated carcinoma are a few examples of differential diagnosis. It is conceptually difficult to diagnose and distinguish LCNEC from sinonasal undifferentiated carcinoma (SNUC) and high-grade olfactory neuroblastoma due to the paucity of occurrences and convergent morphologic and immunohistochemical characteristics.[8]
Owing to the extremely rare nature of LCNEC in the head and neck region, no clinical trials have yet been undertaken to decide on the best course of action for managing both localized and advanced disease.[9] A meta-analysis on neuroendocrine carcinomas of the sinonasal cavity revealed that the choice of treatment method and differentiation grade constitute important indicators of OS. Furthermore, the investigation demonstrated that sinonasal moderately differentiated carcinomas had the highest 5-year disease-specific survival (70.2%), while undifferentiated sinonasal carcinomas had the lowest (35.9%). The majority of sinonasal neuroendocrine carcinoma (SNEC)s responded well to surgery employed as a monotherapy.[10]
Various other studies also suggest surgery as the mainstay for the treatment of such high-grade tumours.[11] But, when sinonasal carcinoma (SNC) spreads to nearby sites like the orbit, ethmoidal sinuses, and nasopharynx, they pose a challenge for surgical removal and often involve the removal of a large portion of the abovementioned structures. NACT helps in the reduction of tumor size and metastases, which makes surgical removal less complicated. CCRT has been used in NEC carcinomas of the lungs and has proved beneficial compared to the use of either chemotherapy or radiotherapy alone. The use of chemotherapy along with radiotherapy provides solutions for radio-resistance, via mechanisms involving either additivity or supra-additivity.[2]
Though CCRT has its benefits, its usage is limited, a prospective study conducted in the Netherlands suggested that, due to a number of comorbidities, 59% of the 686 patients with non-small cell lung carcinoma (NSLC) cancer were deemed unfit for CCRT.[12] In another prospective cohort study of 341 randomized patients with low-risk nasopharyngeal carcinoma, intensity-modulated radiation therapy (IMRT) alone was not inferior to CCRT. When compared to CCRT, IMRT alone resulted in noticeably fewer grade 3 to 4 adverse events (17% vs. 46%). A case report on LCNEC reported no significant improvement in patients with NACT, but CCRT followed by adjuvant chemotherapy led to complete remission of solid tumors based on nasal endoscopy.[13] In a different case, a 35-year-old patient with nasopharyngeal LCNEC (T4N0M0) was treated with six rounds of chemotherapy and then radiation treatment. Six months following the end of treatment, the patient presented with a local and meningeal relapse despite having previously shown clinical and radiological improvement. In the end, the patient received palliative care till passing away.[14] Although more research is needed to confirm these findings, but two cases of Epstein-Barr virus (EBV)-positive LCNEC were successfully treated with chemotherapy and radiation. EBV-positive LCNEC may be more responsive to chemoradiotherapy and therefore have a better prognosis than EBV-negative LCNEC.[15] [16]
Conclusion
The entity of LCNEC of nasal cavity is rare and the use of a specific treatment modality remains debatable, majorly due to few numbers reported and different treatment protocols showing varied results. Surgery poses challenges for such high-grade tumors. Chemotherapy or CCRT showed promising result in our case. Two cases with EBV-positive LCNEC and one case failed to show improvement with NACT. Chemotherapy followed by radiotherapy was not successful. The data available is insignificant to reach a consensus for treatment protocol of LCNEC of sinonasal cavity.
Conflict of Interest
None declared.
Patient Consent
Patient consent has been taken.
Affiliation where the work was carried out: AFMC & CH (SC), Pune.
-
References
- 1 Corbett V, Arnold S, Anthony L, Chauhan A. Management of large cell neuroendocrine carcinoma. 2021; 11: 1-20
- 2 Seiwert TY, Salama JK, Vokes EE. The concurrent chemoradiation paradigm--general principles. Nat Clin Pract Oncol 2007; 4 (02) 86-100
- 3 Lahma J, Hejjouji R, Gicquel P, Essakalli L. Large cell neuroendocrine carcinoma of the nasal cavity: an extremely rare and new distinct entity. Pan Afr Med J 2018; 30: 188
- 4 Wu W, Gan P, Xu Q, Wang Y, Liao H. Neuroendocrine carcinoma of the nasal cavity with epiphora as the first symptom: a case report. Medicine (Baltimore) 2020; 99 (49) e23502
- 5 Thompson ED, Stelow EB, Mills SE, Westra WH, Bishop JA. Large cell neuroendocrine carcinoma of the head and neck: a clinicopathologic series of 10 cases with an emphasis on HPV status. Am J Surg Pathol 2016; 40 (04) 471-478
- 6 Mills SE. Neuroectodermal neoplasms of the head and neck with emphasis on neuroendocrine carcinomas. Mod Pathol 2002; 15 (03) 264-278
- 7 Survival O. Head and neck large cell neuroendocrine carcinoma should be separated from atypical carcinoid on the basis of different clinical features. 2012; 36 (02) 185-192
- 8 Shah K, Perez-Ordóñez B. Neuroendocrine neoplasms of the sinonasal tract: neuroendocrine carcinomas and olfactory neuroblastoma. Head Neck Pathol 2016; 10 (01) 85-94
- 9 Ferlito A, Strojan P, Lewis Jr JS, Perez-Ordoñez B, Rinaldo A. Large cell neuroendocrine carcinoma of the head and neck: a distinct clinicopathologic entity. Eur Arch Otorhinolaryngol 2014; 271 (08) 2093-2095
- 10 van der Laan TP, Iepsma R, Witjes MJH, van der Laan BFAM, Plaat BEC, Halmos GB. Meta-analysis of 701 published cases of sinonasal neuroendocrine carcinoma: the importance of differentiation grade in determining treatment strategy. Oral Oncol 2016; 63: 1-9
- 11 Bell D, Hanna EY, Weber RS. et al. Neuroendocrine neoplasms of the sinonasal region. Head Neck 2016; 38 (Suppl. 01) E2259-E2266
- 12 De Ruysscher D, Botterweck A, Dirx M. et al. Eligibility for concurrent chemotherapy and radiotherapy of locally advanced lung cancer patients: a prospective, population-based study. Ann Oncol 2009; 20 (01) 98-102
- 13 Tang LL, Guo R, Zhang N. et al. Effect of radiotherapy alone vs radiotherapy with concurrent chemoradiotherapy on survival without disease relapse in patients with low-risk nasopharyngeal carcinoma: a randomized clinical trial. JAMA 2022; 328 (08) 728-736
- 14 Zhao Q, Wei J, Zhang C. et al. Large-cell neuroendocrine carcinoma of nasal cavity and paranasal sinuses after successful curative therapy: a case report and literature review. OncoTargets Ther 2019; 12: 2975-2980
- 15 Wasserman JK, Papp S, Hope AJ, Perez-Ordóñez B. Epstein-Barr virus-positive large cell neuroendocrine carcinoma of the nasopharynx: report of a case with complete clinical and radiological response after combined chemoradiotherapy. Head Neck Pathol 2018; 12 (04) 587-591
- 16 Cai Z, Lin M, Blanco AI, Liu J, Zhu H. Epstein – Barr virus-positive large cell neuroendocrine carcinoma of the nasopharynx: report of one case and review of the literature. Head Neck Pathol 2019; 13 (03) 313-317
Address for correspondence
Publication History
Article published online:
07 November 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Corbett V, Arnold S, Anthony L, Chauhan A. Management of large cell neuroendocrine carcinoma. 2021; 11: 1-20
- 2 Seiwert TY, Salama JK, Vokes EE. The concurrent chemoradiation paradigm--general principles. Nat Clin Pract Oncol 2007; 4 (02) 86-100
- 3 Lahma J, Hejjouji R, Gicquel P, Essakalli L. Large cell neuroendocrine carcinoma of the nasal cavity: an extremely rare and new distinct entity. Pan Afr Med J 2018; 30: 188
- 4 Wu W, Gan P, Xu Q, Wang Y, Liao H. Neuroendocrine carcinoma of the nasal cavity with epiphora as the first symptom: a case report. Medicine (Baltimore) 2020; 99 (49) e23502
- 5 Thompson ED, Stelow EB, Mills SE, Westra WH, Bishop JA. Large cell neuroendocrine carcinoma of the head and neck: a clinicopathologic series of 10 cases with an emphasis on HPV status. Am J Surg Pathol 2016; 40 (04) 471-478
- 6 Mills SE. Neuroectodermal neoplasms of the head and neck with emphasis on neuroendocrine carcinomas. Mod Pathol 2002; 15 (03) 264-278
- 7 Survival O. Head and neck large cell neuroendocrine carcinoma should be separated from atypical carcinoid on the basis of different clinical features. 2012; 36 (02) 185-192
- 8 Shah K, Perez-Ordóñez B. Neuroendocrine neoplasms of the sinonasal tract: neuroendocrine carcinomas and olfactory neuroblastoma. Head Neck Pathol 2016; 10 (01) 85-94
- 9 Ferlito A, Strojan P, Lewis Jr JS, Perez-Ordoñez B, Rinaldo A. Large cell neuroendocrine carcinoma of the head and neck: a distinct clinicopathologic entity. Eur Arch Otorhinolaryngol 2014; 271 (08) 2093-2095
- 10 van der Laan TP, Iepsma R, Witjes MJH, van der Laan BFAM, Plaat BEC, Halmos GB. Meta-analysis of 701 published cases of sinonasal neuroendocrine carcinoma: the importance of differentiation grade in determining treatment strategy. Oral Oncol 2016; 63: 1-9
- 11 Bell D, Hanna EY, Weber RS. et al. Neuroendocrine neoplasms of the sinonasal region. Head Neck 2016; 38 (Suppl. 01) E2259-E2266
- 12 De Ruysscher D, Botterweck A, Dirx M. et al. Eligibility for concurrent chemotherapy and radiotherapy of locally advanced lung cancer patients: a prospective, population-based study. Ann Oncol 2009; 20 (01) 98-102
- 13 Tang LL, Guo R, Zhang N. et al. Effect of radiotherapy alone vs radiotherapy with concurrent chemoradiotherapy on survival without disease relapse in patients with low-risk nasopharyngeal carcinoma: a randomized clinical trial. JAMA 2022; 328 (08) 728-736
- 14 Zhao Q, Wei J, Zhang C. et al. Large-cell neuroendocrine carcinoma of nasal cavity and paranasal sinuses after successful curative therapy: a case report and literature review. OncoTargets Ther 2019; 12: 2975-2980
- 15 Wasserman JK, Papp S, Hope AJ, Perez-Ordóñez B. Epstein-Barr virus-positive large cell neuroendocrine carcinoma of the nasopharynx: report of a case with complete clinical and radiological response after combined chemoradiotherapy. Head Neck Pathol 2018; 12 (04) 587-591
- 16 Cai Z, Lin M, Blanco AI, Liu J, Zhu H. Epstein – Barr virus-positive large cell neuroendocrine carcinoma of the nasopharynx: report of one case and review of the literature. Head Neck Pathol 2019; 13 (03) 313-317