

RSS-Feed abonnieren
DOI: 10.1055/s-0045-1812479
Chronic Diarrhea Unveiling a Rare Cecal Ganglioneuroma
Autoren

A 55-year-old male presented to the outpatient department with a 1-year history of intermittent diarrhea. The patient described loose stools occurring three to four times per day, predominantly in the mornings, without nocturnal symptoms. There was no blood or mucus in stools, abdominal pain, fever, weight loss, or history of antibiotic/medication use. The stools were non-oily, not bulky, and not associated with urgency or tenesmus. His medical history was unremarkable. Physical examination was within normal limits. Routine blood investigations, including complete blood count, liver and renal function tests, thyroid profile, and stool analysis, were normal.
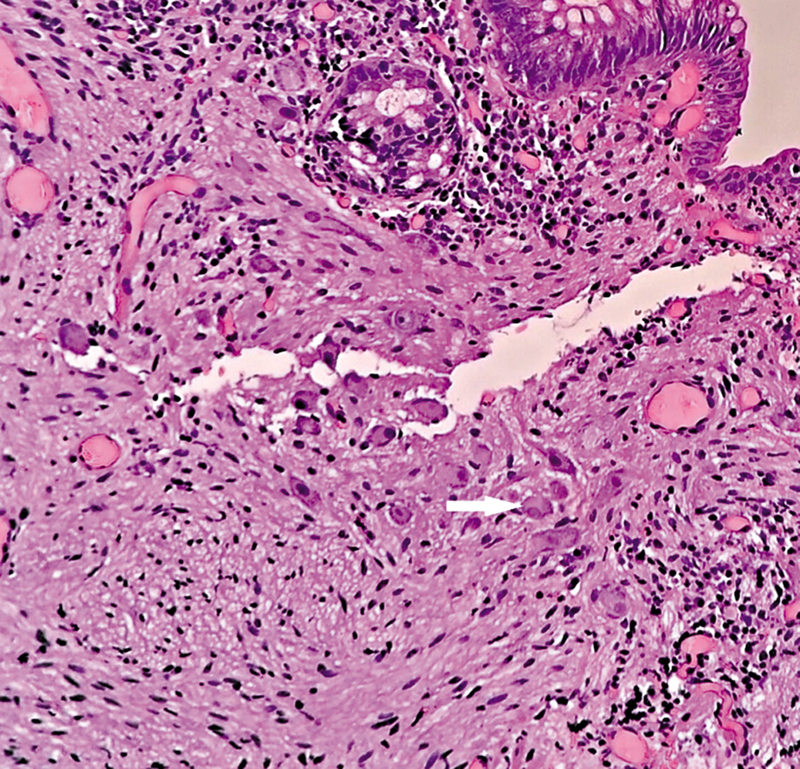
Given the chronicity of symptoms, a colonoscopy was performed. The colonoscopic examination revealed a single sessile polyp measuring approximately 1.2 cm in the cecum ([Fig. 1]). No other mucosal abnormalities were noted throughout the colon. Endoscopic polypectomy ([Fig. 2]) was performed, and the specimen was sent for histopathological examination. Microscopic evaluation revealed ganglion cells with neuronal spindle cells with wavy nuclei suggestive of ganglioneuroma ([Fig. 3]). Immunohistochemical staining showed positive expression of S100 and synaptophysin, supporting the diagnosis ([Figs. 4] and [5]). Following polypectomy, the patient reported complete resolution of diarrhea during follow-up visits.




In the present case, although the lesion was small and histologically nonsecretory, possible hypothesis for the resolution of diarrhea include: (1) polyp being an incidental finding with coincidental improvement of functional diarrhea, (2) local mucosal irritation or motility alteration caused by the lesion, (3) overlap with an irritable bowel syndrome-like presentation with symptomatic relief following intervention, (4) intermittent luminal flow alteration due to its location in the cecal fold, and (5) a potential neuromodulatory effect of polypectomy itself. While a direct causal relationship cannot be conclusively established, excision and histological confirmation remain clinically relevant for patient reassurance and accurate diagnosis.
Practical Implications for Endoscopists
-
Diagnostic tips: maintain a high index of suspicion for rare benign lesions such as ganglioneuromas in patients with nonspecific chronic diarrhea.[1] [2] Carefully inspect the mucosa, and document morphology and lesion location during colonoscopy.[3] [4]
-
Procedural cautions: ensure complete excision of even small or benign-appearing lesions, followed by histopathological evaluation, since endoscopic appearance alone is insufficient.[3] [4] Recognizing such rare benign tumors is essential to avoid misdiagnosis and to guide further follow-up when required.[5]
-
Therapeutic implications: provide reassurance to patients regarding the benign nature of ganglioneuromas to reduce anxiety. Avoid unnecessary aggressive surveillance unless multiple or syndromic lesions are suspected. Tailor follow-up to clinical symptoms rather than routine surveillance in isolated, sporadic lesions.
Conflict of Interest
None declared.
-
References
- 1 Mahdi M, Afaneh K, Mahdi A, Tayyem O. Colonic ganglioneuroma: a rare incidental finding. Kans J Med 2023; 16 (01) 112-113
- 2 Badrinath M, Mandru R, Lowe D, Manocha D, Achufusi T. Isolated intestinal ganglioneuroma mimicking small bowel Crohn's Disease. ACG Case Rep J 2019; 11 ;6 (07) e00114
- 3 Bahmad HF, Trinh S, Quian L, Terp K, Alloush F, Elajami MK. et al. Colonic Ganglioneuroma: A combined single-institution experience and review of the literature of forty-three patients. Diseases 2023; 11 (02) 69
- 4 Baiomi A, Abbas H, Niazi M, Remotti H, Daniel M, Balar B. Colonic Ganglioneuroma: A Rare Lesion With Extremely Different Presentations and Outcomes in Two Patients. Gastroenterology Res 2021; 14 (03) 194-198
- 5 Chambonnière ML, Porcheron J, Scoazec JY, Audigier JC, Mosnier JF. Intestinal ganglioneuromatosis diagnosed in adult patients [in French]. Gastroenterol Clin Biol 2003; 27 (02) 219-224
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
16. Oktober 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Mahdi M, Afaneh K, Mahdi A, Tayyem O. Colonic ganglioneuroma: a rare incidental finding. Kans J Med 2023; 16 (01) 112-113
- 2 Badrinath M, Mandru R, Lowe D, Manocha D, Achufusi T. Isolated intestinal ganglioneuroma mimicking small bowel Crohn's Disease. ACG Case Rep J 2019; 11 ;6 (07) e00114
- 3 Bahmad HF, Trinh S, Quian L, Terp K, Alloush F, Elajami MK. et al. Colonic Ganglioneuroma: A combined single-institution experience and review of the literature of forty-three patients. Diseases 2023; 11 (02) 69
- 4 Baiomi A, Abbas H, Niazi M, Remotti H, Daniel M, Balar B. Colonic Ganglioneuroma: A Rare Lesion With Extremely Different Presentations and Outcomes in Two Patients. Gastroenterology Res 2021; 14 (03) 194-198
- 5 Chambonnière ML, Porcheron J, Scoazec JY, Audigier JC, Mosnier JF. Intestinal ganglioneuromatosis diagnosed in adult patients [in French]. Gastroenterol Clin Biol 2003; 27 (02) 219-224