

Subscribe to RSS
DOI: 10.1055/s-0045-1811263
Enhancing Proctological Outcomes: The Role of Hyaluronic Acid in Hemorrhoid Care – An Innovative Adjunct to Surgery
Authors
Funding The author(s) received no financial support for the research.

Abstract
Introduction
Hemorrhoids are common anorectal conditions characterized by swollen and inflamed veins in the rectal and anal regions. They are classified as internal, external, or mixed, and may present with rectal bleeding, pain, itching, and prolapse. Chronic constipation, prolonged straining, and increased intra-abdominal pressure are frequent etiological factors. Management strategies range from conservative measures, such as dietary modifications and topical agents, to surgical procedures including hemorrhoidectomy and stapled hemorrhoidopexy.
Objective
To describe the therapeutic potential of hyaluronic acid (HA) in the management of hemorrhoids and to report clinical outcomes in patients treated with HA infiltration.
Results
Five patients with hemorrhoids underwent HA infiltration. Treatment was associated with significant symptom relief, reduced edema, and improved post-surgical recovery. The mechanism of action involved enhanced fibroblast activity, decreased inflammatory cytokines, and improved mucosal hydration.
Conclusion
Hyaluronic acid demonstrates promising results as a safe and effective option for hemorrhoid management. Its hydrating, anti-inflammatory, and wound-healing properties support its role as a versatile therapeutic agent in both conservative and surgical settings, contributing to improved patient outcomes.
Introduction
Hemorrhoids are swollen and inflamed veins in the rectal and anal region. They are classified into two main types: Internal hemorrhoids, which are located inside the rectum and are usually painless but may cause bleeding; and external hemorrhoids, which are found under the skin around the anus, often associated with pain, itching, and swelling. Common causes include chronic constipation, prolonged sitting, pregnancy, and straining during bowel movements. Treatment ranges from lifestyle modifications to surgical interventions, depending on severity.[1] [2]
Hyaluronic acid (HA), a naturally occurring glycosaminoglycan, is well-known for its hydrating and anti-inflammatory properties. Its role in promoting tissue repair and enhancing wound healing has led to its application in various medical fields. Recently, the use of HA in managing hemorrhoids has garnered attention due to its effectiveness in reducing symptoms and promoting healing.[3] [4]
We report here a series of 5 cases presenting in varying stages of hemorrhoids, treated with topical infiltration of HA with the intent of providing symptomatic relief and optimization for surgical treatment.
Case Series with Treatment Pathway and Outcomes
Case 1
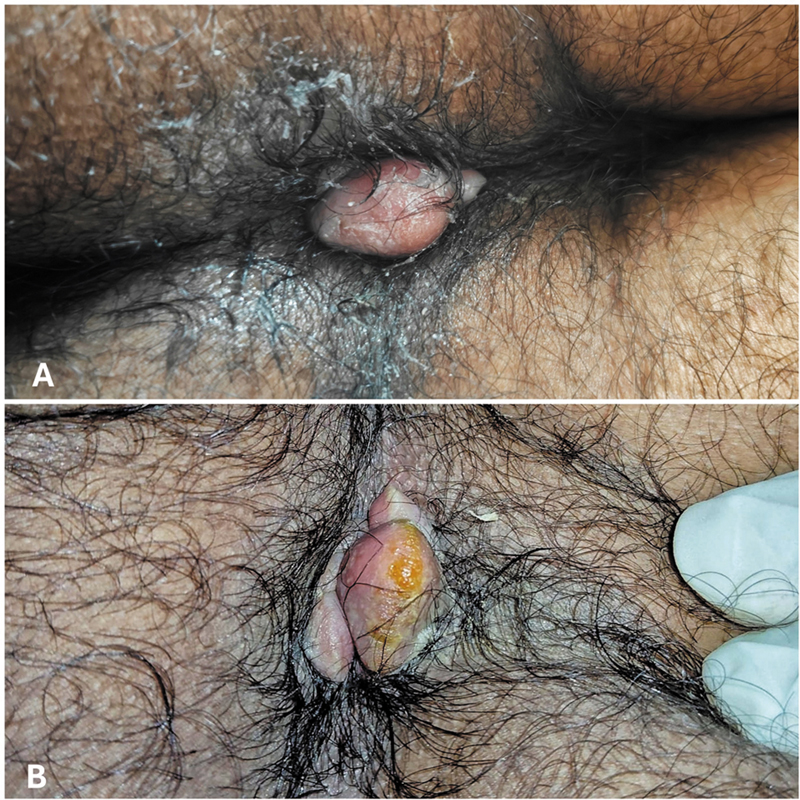
A 42-year-old male presented with complaints of foreign body sensation in the anal region, occasional bleeding, and pain during defecation. He was having a solitary, reducible Grade III thrombosed hemorrhoid, with no associated fissures or skin tags, and a normal anal tone ([Fig. 1A]).

Under aseptic precautions, the hemorrhoid was topically infiltrated with a 10ml solution of 5ml normal saline, 5ml of 2% lignocaine, and 1500mcg HA.
24 hours later, the hemorrhoid appeared shrunken in size, with significant reduction in edema and relief in pain ([Fig. 1B]). The patient underwent open hemorrhoidectomy with hemorrhoidal artery ligation (HAL). Upon excising the hemorrhoid at the base, there was no evidence of bleeding ([Fig. 1C]). The patient made an uneventful recovery. [Fig. 1]
Case 2
A 32-year-old male presented with a complaint of severe pain and bleeding during defecation. Upon examination, he was having a solitary, tender, irreducible Grade IV hemorrhoid, with an increased anal tone ([Fig. 2A]).
Under aseptic precautions, the hemorrhoid was topically infiltrated with a 10ml solution of 5ml normal saline, 5ml of 2% lignocaine, and 1500mcg HA.
The patient reported significant relief in pain over the next 48 hours, and the local examination revealed a relaxed anal tone with mild reduction in edema and size of hemorrhoid ([Fig. 2B]). The patient underwent open hemorrhoidectomy with HAL and made an uneventful recovery. [Fig. 2]
Case 3
A 28-year-old male presented with the complaint of painful defecation for 6 months, not relieved with conservative measures for hemorrhoid treatment. Examination revealed a solitary, inflamed, tender, irreducible Grade IV hemorrhoid, with an increased anal tone and a skin tag ([Fig. 3A]).

Under aseptic precautions, the hemorrhoid was topically infiltrated with a 10ml solution of 5ml normal saline, 5ml of 2% lignocaine, and 1 vial containing 1500mcg HA.
The patient was not willing to undergo surgery. Upon follow-up one week later, the patient reported significant pain relief. Local examination showed relaxation in the anal tone as well as reduced inflammation and edema of the hemorrhoid ([Fig. 3B]). [Fig. 3]
Case 4
A 54-year-old male having a solitary, non-tender Grade III hemorrhoid ([Fig. 4A]) was admitted for surgery – Minimally Invasive Procedure for Hemorrhoidectomy (MIPH) using a stapler under spinal anesthesia. Following induction, the hemorrhoid was topically infiltrated intraoperatively with a 10ml solution of 5ml normal saline, 5ml of 2% lignocaine, and 1 vial containing 1500mcg HA.

10 minutes after the infiltration, the hemorrhoid showed significant size reduction, with relief in surrounding edema as well, facilitating easier excision with minimal bleeding ([Fig. 4B]). Post-operatively, the patient showed rapid recovery with minimal post-operative pain and improved healing upon follow-up examination. [Fig. 4]
Case 5
A 63-year-old male with a recent history of stroke was brought with complaints of constipation and a foreign body sensation in the anal region, having prolapsed Grade IV hemorrhoids at 4, 7 and 11 o'clock positions ([Fig. 5A]).

Topical application of glycerin-soaked packs showed little improvement over 2 days. Subsequently, the hemorrhoids were topically infiltrated with a 20ml solution of 10ml normal saline, 10ml of 2% lignocaine, and 2 vials containing 3000mcg HA.
Over the next 24 hours, the patient exhibited pain relief and reduced straining while passing stool. The hemorrhoids showed moderate reduction in size, with reduced edema and inflammation ([Fig. 5B]). The patient continued conservative treatment with stool softeners and hot sitz baths and was discharged 1 week later following resolution of symptoms. [Fig. 5]
Discussion
Hemorrhoids are a prevalent anorectal condition affecting individuals across all age groups. Hemorrhoids are classified based on their location relative to the dentate line[2]:
-
Internal Hemorrhoids: Located above the dentate line,
-
External Hemorrhoids: Located below the dentate line,
-
Interno-External Hemorrhoids: A combination of both.
Understanding the pathophysiology of the development of hemorrhoids is critical to developing effective treatment strategies. Key mechanisms include:
-
Vascular Changes: Increased pressure in the hemorrhoidal plexus leads to vascular engorgement and venous dilation.
-
Connective Tissue Degeneration: Weakening of the supportive connective tissue results in prolapse.
-
Inflammatory Processes: Chronic irritation or straining causes local inflammation, leading to pain, itching, and swelling.
-
Elevated Intra-Abdominal Pressure: Conditions such as chronic constipation, pregnancy, and prolonged straining exacerbate pressure on hemorrhoidal tissue.
Patients present with complaints of painless rectal bleeding, prolapse of hemorrhoids during defecation, pruritus, pain while defecation, swelling in the perianal region, thrombosis of the hemorrhoid, and foreign body sensation in the perianal region. At times, patients may present with completely prolapsed hemorrhoids, bleeding, acute thrombosis, and ulceration of the hemorrhoids, along with fissures and anal canal stenosis, requiring emergent intervention.[1]
Conservative measures of management include a diet rich in fiber and improved hydration, topical application agents like steroidal creams and local anesthetic agents, and flavonoids. Interventional strategies include injection of sclerosant, which induces fibrosis and shrinks the hemorrhoids, band ligation of the hemorrhoids, or newer modalities like infrared coagulation. Surgical techniques include standard hemorrhoidectomy (Milligan-Morgan or Ferguson), MIPH or Stapler hemorrhoidopexy, and ultrasound-guided hemorrhoidal artery ligation.[1]
A recent advance in the treatment of hemorrhoids, especially acute hemorrhoidal crisis, is the use of hyaluronic acid as a topical agent in different forms. HA is a naturally occurring glycosaminoglycan with a wide array of clinical applications.[4] It stimulates fibroblast activity and enhances collagen production and tissue remodeling, allowing improved wound healing of mucosal tears and fissures associated with hemorrhoids. HA exerts anti-inflammatory effects by modulating cytokine release and reducing tissue inflammation and edema, causing a shrinkage in the size of hemorrhoids, reducing the tension and pain in the perianal region. It also acts as a mucosal protective agent due to its water retention properties, keeping the mucosa hydrated and forming a protective barrier.[3] Topical HA is available in multiple forms. Topical creams or gels containing hyaluronic acid in combination with local anesthetic agents like lidocaine are widely available. HA-based suppositories are also effective for internal hemorrhoids, providing localized relief and promoting mucosal repair.[5]
Joksimovic et al conducted a study on 36 patients, testing a gel medical device containing HA as a primary active ingredient, and reported benefits of HA-containing topical gel application.[6] In another study, the investigators tested a myophlebotrophic preparation having six components, HA being one amongst them, against a placebo and found significant benefit from using the topical preparation.[7] Another multicenter observational study from 2024 evaluated the use of a chlorhexidine-HA containing gel for post-operative pain relief, reporting improved analgesia and symptomatic relief with the use of the gel.[8]
In 1963, Zamborsky et al demonstrated the use of HA as a spreading agent for local anesthesia in the treatment of hemorrhoids and procidentia, allowing better surgical outcomes.[9] Another case report by Kolbe et al advocated topical infiltration of HA with a local anesthetic agent.[10] In our case series of 5 patients, we found that topical infiltration of HA with local anesthetic agents – either pre-operatively or intra-operatively, or even for conservative management, is a highly viable option and affords better clinical outcomes for the patients in terms of pain relief, bleeding, and improved recovery arcs following surgery.
In conclusion, hemorrhoids are a common condition that can significantly impact quality of life if untreated. Understanding anatomy and pathophysiology is essential for designing effective management strategies. HA has a wide range of clinical applications and must be explored as a topical agent for the management of hemorrhoids.
Conflict of Interest
The authors report no conflict of interest.
Authors' Contributions
RU: conceptualization, methodology, investigation, writing – original draft; AV: data curation, formal analysis, writing – review & editing; HVP: resources, validation, writing – review & editing; SU: supervision, project administration, writing – review & editing.
Data Availability Statement
The data that support the findings of this study are available from the authors upon reasonable request.
ORCID IDs
Riddhi Upadhyay – https://orcid.org/0009-0008-4837-9255
Akshat Vadaliya – https://orcid.org/0009-0004-9490-4656
Haryax V. Pathak – https://orcid.org/0000-0003-3683-3672
Soham Upadhyay – https://orcid.org/0009-0008-4218-3390
-
References
- 1 Sanchez C, Chinn BT. Hemorrhoids. Clin Colon Rectal Surg 2011; 24 (01) 5-13
- 2 Steele SR. Anorectal Disease, An Issue of Surgical Clinics. Elsevier Health Sciences; 2010: 229
- 3 Gupta RC, Lall R, Srivastava A, Sinha A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front Vet Sci 2019; 6: 192 https://www.frontiersin.org/journals/veterinary-science/articles/10.3389/fvets.2019.00192/full cited 2025Jan7 [Internet]
- 4 Kotla NG, Bonam SR, Rasala S. et al. Recent advances and prospects of hyaluronan as a multifunctional therapeutic system. J Control Release 2021; 336: 598-620
- 5 Scaldaferri F, Ingravalle F, Zinicola T, Holleran G, Gasbarrini A. Medical Therapy of Hemorrhoidal Disease. In: Ratto C, Parello A, Litta F. editors. Hemorrhoids [Internet]. Cham: Springer International Publishing; 2018. [cited 2025 Jan 7]. p. 49–72. Available from: https://doi.org/10.1007/978-3-319-53357-5_6
- 6 Joksimovic N, Spasovski G, Joksimovic V, Andreevski V, Zuccari C, Omini CF. Efficacy and tolerability of hyaluronic acid, tea tree oil and methyl-sulfonyl-methane in a new gel medical device for treatment of haemorrhoids in a double-blind, placebo-controlled clinical trial. Updates Surg 2012; 64 (03) 195-201
- 7 The influence of supportive therapy with a six-component myophlebotropic preparation on the reduction of symptoms in patients with symptoms of hemorrhoidal disease [Internet]. [cited 2025 Jan 7]. Available from: https://ppch.pl/article/546443/en
- 8 Brillantino A, Marano L, Grillo M. et al. Lower pain, less itching, and faster healing after ultrasound scalpel-assisted hemorrhoidectomy using an intimate cleaner containing chlorhexidine, acid hyaluronic acid, and natural anti-inflammatories: a multicenter observational case-control study. Ann Coloproctol 2024; 40 (06) 602-609
- 9 Zamborsky EJ, Trimpi HD. Hyaluronidase in local anesthesia for severe hermorrhoids and procidentia. Dis Colon Rectum 1963; 6 (06) 411-414
- 10 Kolbe N, Hain J. Treatment of acute hemorrhoidal crisis using hyaluronidase with local anesthetic prior to surgical excision. Tech Coloproctol 2015; 19 (08) 487-488
Address for correspondence
Publication History
Received: 09 April 2025
Accepted: 21 July 2025
Article published online:
16 October 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution 4.0 International License, permitting copying and reproduction so long as the original work is given appropriate credit (https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda.
Rua Rego Freitas, 175, loja 1, República, São Paulo, SP, CEP 01220-010, Brazil
Riddhi Upadhyay, Akshat Vadaliya, Haryax V. Pathak, Soham Upadhyay. Enhancing Proctological Outcomes: The Role of Hyaluronic Acid in Hemorrhoid Care – An Innovative Adjunct to Surgery. Journal of Coloproctology 2025; 45: s00451811263.
DOI: 10.1055/s-0045-1811263
-
References
- 1 Sanchez C, Chinn BT. Hemorrhoids. Clin Colon Rectal Surg 2011; 24 (01) 5-13
- 2 Steele SR. Anorectal Disease, An Issue of Surgical Clinics. Elsevier Health Sciences; 2010: 229
- 3 Gupta RC, Lall R, Srivastava A, Sinha A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front Vet Sci 2019; 6: 192 https://www.frontiersin.org/journals/veterinary-science/articles/10.3389/fvets.2019.00192/full cited 2025Jan7 [Internet]
- 4 Kotla NG, Bonam SR, Rasala S. et al. Recent advances and prospects of hyaluronan as a multifunctional therapeutic system. J Control Release 2021; 336: 598-620
- 5 Scaldaferri F, Ingravalle F, Zinicola T, Holleran G, Gasbarrini A. Medical Therapy of Hemorrhoidal Disease. In: Ratto C, Parello A, Litta F. editors. Hemorrhoids [Internet]. Cham: Springer International Publishing; 2018. [cited 2025 Jan 7]. p. 49–72. Available from: https://doi.org/10.1007/978-3-319-53357-5_6
- 6 Joksimovic N, Spasovski G, Joksimovic V, Andreevski V, Zuccari C, Omini CF. Efficacy and tolerability of hyaluronic acid, tea tree oil and methyl-sulfonyl-methane in a new gel medical device for treatment of haemorrhoids in a double-blind, placebo-controlled clinical trial. Updates Surg 2012; 64 (03) 195-201
- 7 The influence of supportive therapy with a six-component myophlebotropic preparation on the reduction of symptoms in patients with symptoms of hemorrhoidal disease [Internet]. [cited 2025 Jan 7]. Available from: https://ppch.pl/article/546443/en
- 8 Brillantino A, Marano L, Grillo M. et al. Lower pain, less itching, and faster healing after ultrasound scalpel-assisted hemorrhoidectomy using an intimate cleaner containing chlorhexidine, acid hyaluronic acid, and natural anti-inflammatories: a multicenter observational case-control study. Ann Coloproctol 2024; 40 (06) 602-609
- 9 Zamborsky EJ, Trimpi HD. Hyaluronidase in local anesthesia for severe hermorrhoids and procidentia. Dis Colon Rectum 1963; 6 (06) 411-414
- 10 Kolbe N, Hain J. Treatment of acute hemorrhoidal crisis using hyaluronidase with local anesthetic prior to surgical excision. Tech Coloproctol 2015; 19 (08) 487-488