

Subscribe to RSS
DOI: 10.1055/s-0045-1810085
Citral and Geraniol: Two Novel and Potent Noncarcinogenic Terpene Alternatives to Alcohol-Based Mouthwashes against Cariogenic Oral Bacteria
Authors

Abstract
Objective
Several recent studies have linked the high incidence of oral cancer among users with a history of prolonged use of alcohol-based mouthwashes, due to increased topical acetaldehyde, a carcinogen made from alcohol breakdown. Our research has previously shown that two volatile oils, Cymbopogon winterianus (Lemon grass) and Cymbopogon flexuosus (Citronella Java), exhibit significant antibacterial activity on four commonly occurring cariogenic oral bacteria. We have also demonstrated that these oils are mainly composed of four terpenes: citronellal, citronellol, geraniol, and citral. In this follow-up study, we wanted to determine which of these specific terpene constituents was responsible for the antibacterial activity of these two volatile oils.
Materials and Methods
In this study, we tested these terpenes on our selected panel of oral bacteria, namely Micrococcus luteus, Streptococcus salivarius, Streptococcus mutans, and Enterococcus faecalis in several qualitative assays such as Kirby–Bauer disc diffusion, minimum inhibitory concentration determination, minimum bactericidal concentration determination, and time-kill kinetics to evaluate their effectiveness as antibacterial agents.
Results
Citral and geraniol emerged as the most potent broad-spectrum antibacterial agents among all four terpene candidates. More specifically, citral was most effective on both oral streptococcal strains followed by geraniol, while geraniol exhibited the highest antibacterial activity against E. faecalis. Both terpenes showed a similar pattern of killing as seen with oral streptococci when tested against M. luteus.
Conclusion
We hypothesize that these two terpenes may serve as safer, better alternatives to alcohol-based mouthwashes.
Introduction
About half a million cases of oropharyngeal cancer arise per year, leading to approximately a quarter million deaths each year in the United States alone. With an estimated 5-year survival rate in less than 50% of such affected individuals, preventive measures for these types of cancers are essential through the mitigation of risk factors.[1] [2] The main risk factors for oropharyngeal cancers are poor oral hygiene, heavy alcohol consumption, and increased tobacco usage, with over 70% of cases being attributed to tobacco and alcohol exposure.[1] [2] [3] [4] While ethanol itself is not a carcinogenic substance, its first metabolite, acetaldehyde (ACH), is found to be a mutagenic and carcinogenic compound. ACH at mutagenic concentrations can induce deleterious effects such as point mutations, sister chromatid exchanges, cross-chromosomal aberrations, DNA cross-links, DNA adducts, epithelial hyper-proliferation, and can interfere with DNA repair enzymes.[1] [2] [3] [5] [6] [7]
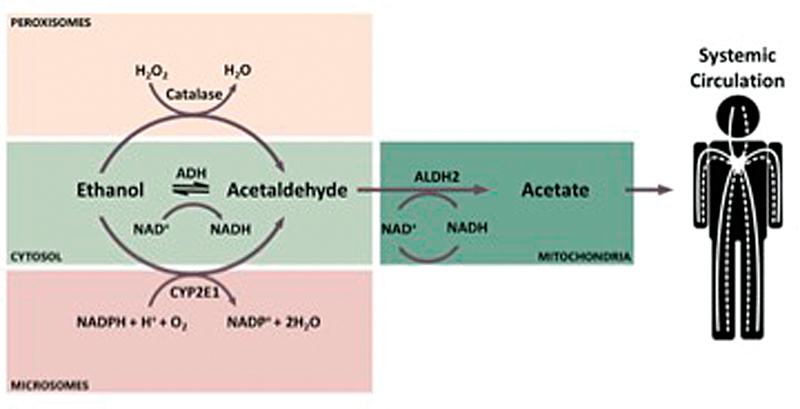
Mutagenic concentrations of ACH are readily achievable with very low concentrations of ethanol.[6] While the risk of ACH exposure from ethanol metabolism comes primarily from the consumption of alcoholic beverages, alcohol-based mouthwashes also pose a significant risk, due to this low concentration of risk threshold. Furthermore, exposure to ACH is cumulative, thus daily exposure to alcohol-containing mouthwashes may lead to significant long-term risk.[1] [4] The estimated concentration of ACH that accumulates twice with daily use as directed is observed to be above the minimum mutagenic concentration and safety threshold for humans.[6] Upon exposure to ethanol, both the oral mucosa and oral microflora play a role in its metabolism. Ethanol is first converted into ACH, catalyzed by alcohol dehydrogenase enzymes.[3] ACH is then converted into acetate by acetaldehyde dehydrogenase enzymes ADHL1 and ALDH2. However, the concentration of acetaldehyde dehydrogenase enzymes in the oral cavity is very low, and oral bacteria have shown to perform alcohol dehydrogenation very effectively, besides exhibiting very low levels of acetaldehyde dehydrogenation enzymatic activity.[4] [5] [8] This results in a buildup of ACH concentration in the oral cavity upon consumption of ethanol.[4] The mechanism of ethanol metabolism is shown in [Fig. 1].[7]
The most at-risk demographic regarding ACH exposure is the same demographic of individuals most likely to consistently use and/or overuse alcohol-based mouthwashes. This demographic is those who are heavy alcohol and tobacco consumers, as well as those with poor oral hygiene.[4] Usage of alcohol-based mouthwashes in this population may perpetuate a vicious cycle of ACH exposure and subsequent poor oral hygiene. Thus, alternative antibacterial agents which do not produce carcinogenic metabolites are necessary.[3] [4] Plant volatile oils have shown promising antibacterial activity against common oral bacteria, suggesting that their main components have the potential to be used as alternate antibacterial agents.[9] [10] [11]
Our previous study using Cymbopogon winterianus and Cymbopogon flexuosus demonstrated significant antibacterial properties of these two volatile oils.[11] In this study, we aim to determine the specific constituents of these volatile oils responsible for their antibacterial activity. Gas chromatography (GC) revealed the main components of C. winterianus to be citronellal, citronellol, and geraniol, while the main component of C. flexuosus is citral; a mixture of E and Z isomers, geranial and neral, respectively.[11] These monoterpenes make up the vast majority of our two oils, thus we hypothesize that one or more of them are responsible for the antibacterial properties we observed in C. winterianus and C. flexuosus in our previous study.[11]
We evaluated the antibacterial activity of these terpenes against a varied panel of oral bacteria. Our panel included the following strains: Micrococcus luteus, Enterococcus faecalis, Streptococcus mutans, and Streptococcus salivarius. These strains were chosen such that the broad-spectrum efficacy of our terpenes could be assessed, and for their wide prevalence in the human oral microbiota. The mitigation of harmful oral bacteria is essential for maintaining good oral health, as well as preventing ACH production, since the majority of ACH metabolism is completed by the oral microflora.[3]
Materials and Methods
Materials: terpenes were purchased from Fisher Scientific (Pittsburgh, Pennsylvania). Bacterial strains were obtained from Carolina Biological Supply Company (Burlington, North Carolina) and Ward's Science (Rochester, New York). Chemicals and reagents were from Fisher Scientific (Pittsburgh, Pennsylvania) and Carolina Biological Supply Company (Burlington, North Carolina).
Terpenes: four terpenes were evaluated in this study, namely, citronellal, citronellol, geraniol, and citral. Terpenes with a percentage purity of greater than 95% were used in all our assays. Their purity was ascertained by GC by the manufacturer (Fisher Scientific, Pittsburgh, Pennsylvania). They were stored in a cool, dry place at 25°C in dark glass bottles to minimize their oxidation.
Growth and maintenance of bacterial cultures: four bacterial strains were chosen for this study, namely, M. luteus, E. faecalis, S. mutans, and S. salivarius. Micrococcus luteus was grown on Tryptic Soy Agar (TSA, Difco, Detroit, Michigan). Enterococcus faecalis was grown on Brain Heart Infusion (BHI, Difco, Detroit, Michigan) Agar. Both S. salivarius and S. mutans were grown on TSA with 5% sheep blood (Carolina Biological Supply Company, Burlington, North Carolina). All strains were propagated at 37°C overnight (approximately 18–20 hours). Bacterial cultures were maintained in their respective growth media in sterile broth at 4°C and fresh cultures were reinoculated every 2 to 3 weeks.
Gram-staining: all bacterial strains were streaked for single colonies under aseptic conditions. Plates were then incubated for 24 hours at 37°C. Standard gram staining procedure was followed with well-isolated single colonies to corroborate colony morphology.[12]
Agar well-diffusion assay: agar well-diffusion assay was adapted from Kirby–Bauer's disc diffusion method.[12] 100 µL of each bacterial strain (OD600 = 0.25–roughly 2 × 108 cells per mL) was spread evenly onto sterile agar plates. Plates were then allowed to dry for about 10 minutes. One such agar plate with each bacterial strain without any terpene served as a negative control for that set. For experimental trials, a sterile serological pipet was used to cut 10 mm wells at the center of each agar plate. 20 µL of the terpene was added into the well. Discs containing 30 μg of tetracycline were tested in parallel as a positive control on all four bacterial strains. Trials with tetracycline were done at least twice to ensure that results were consistent. Plates were left undisturbed and incubated for approximately 18 to 22 hours at 37°C. The diameter of the zone of inhibition was measured for each experiment and recorded. Experimental trials were performed on all the bacterial strains with all four terpenes at least three times, and values were averaged.
Minimum inhibitory concentration (MIC) and minimum bactericidal concentration (MBC) assays: reactions were set up in six sterile tubes. 4 mL of sterile growth media was added to the first tube. 2 mL of sterile media was added to each of the remaining five tubes. 20 µL of the terpene was added to the first tube and mixed well by vortexing. 2 mL was then removed from the first tube and added to the second tube and mixed thoroughly. The terpene was serially diluted by repeating this process between successive tubes. The final tube (tube six) had a total reaction volume of 4 mL. 20 µL of bacterial culture (OD600 = 0.25–approximately 2 × 108 cells per mL) was added to the first five tubes. 40 µL of bacterial culture was added to the last tube to keep the same working concentration of bacterial cells. Bacterial cells were diluted 100-fold (2000 µL/ 20 µL) to achieve a working concentration of 2 × 106 cells in each tube. Sterile media with the same bacterial cell density without any terpene served as a control. Reactions were incubated at 37°C for 18 to 22 hours and observed the next day for bacterial growth. Concentration of candidate terpenes that prevented any bacterial growth was determined as MIC for that terpene against the bacterial strain that was tested.[12] Experimental trials were performed on M. luteus, S. mutans, and S. salivarius with citral and on E. faecalis with geraniol at least three times, and the values were averaged. 100 μL of MIC reactions were then plated on sterile agar plates. The MBC value for a candidate terpene was designated as that concentration that showed no bacterial growth.[12]
Bacterial time kill assay: 5 µL of an older inoculum was used to grow up 20 mL of fresh bacterial culture overnight in sterile media in an incubator shaker with 230 rpm (rotations per minute) at 37°C. Bacterial cell density was adjusted to roughly 4–6 × 108 cells per mL with sterile media. Geraniol was added at a 1:200-fold dilution of the total reaction volume. Bacterial culture without any added terpene served as a control. Bacterial growth was monitored in both control samples and geraniol trials by recording absorbance values at 600 nm using a UV-Vis spectrophotometer at regular time intervals over 4 hours. Absorbance readings were recorded at specific time intervals based on the growth pattern of each strain. Sterile media was used as a blank for control readings. Sterile media with geraniol at a 1:200-fold dilution served as a blank for geraniol trials to eliminate background turbidity seen with the addition of geraniol. The same procedure was followed for all the strains used in this study. Assays were repeated at least three times with each strain and values were averaged. Bacterial cell density (CFU/mL) was then plotted on a log scale versus time in hours to analyze the killing dynamics of geraniol on each strain.
Results
Terpenes: four terpenes were analyzed in our study, namely: citral, citronellal, citronellol, and geraniol. Citral is composed of an equimolar mixture of its trans and cis forms, namely, neral and geranial ([Fig. 2A, B]). It is an open chain monoterpenoid aldehyde. Citronellal is a monoterpenoid aldehyde ([Fig. 2C]). Citronellol is a monoterpene aromatic alcohol ([Fig. 2D]). Geraniol is an acyclic isoprenoid monoterpene aromatic alcohol ([Fig. 2E]).[13]

Gram staining: all the strains were identified as gram-positive cocci since they were spherical and stained purple. Streptococcus mutans colonies appear as short chains. Colonies of S. salivarius appear as small coccal clusters. Micrococcus luteus colonies appear as tetrads. Enterococcus faecalis appears as short chains as well as small clusters of two coccal colonies. This is corroborated with relevant literature regarding these oral bacteria ([Fig. 3]).[12]

Agar well diffusion assay: among all four terpenes that were tested, citronellal was most effective against M. luteus, followed by citral ([Fig. 4]). Citronellal produced a much higher zone of inhibition (diameter: 54 mm) on M. luteus, more than twice what was observed with the positive control tetracycline (diameter: 23.8 mm). However, it had no effect on E. faecalis. Citral was also highly efficient at killing M. luteus with an average zone of inhibition diameter of 18 mm, followed by geraniol with an average zone of inhibition diameter of 13.5 mm ([Table 1]). Citral exhibited the highest lethal effect on both oral Streptococcal strains, followed by geraniol. Zone of inhibition diameters seen with citral and geraniol on S. mutans were 23.8 and 20.7 mm, respectively ([Fig. 5] and [Table 2]). Likewise, zone of inhibition diameters seen with citral and geraniol on S. salivarius were 23.5 and 16.5 mm, respectively ([Fig. 6] and [Table 3]). Geraniol showed the highest antibacterial activity against E. faecalis with an inhibition zone 15.5 mm in diameter ([Table 4]). Overall, the antibacterial activity shown by citral and geraniol was similar or much higher than what was observed with tetracycline on the bacterial strains used in our study ([Tables 1] [2] [3] [4]).

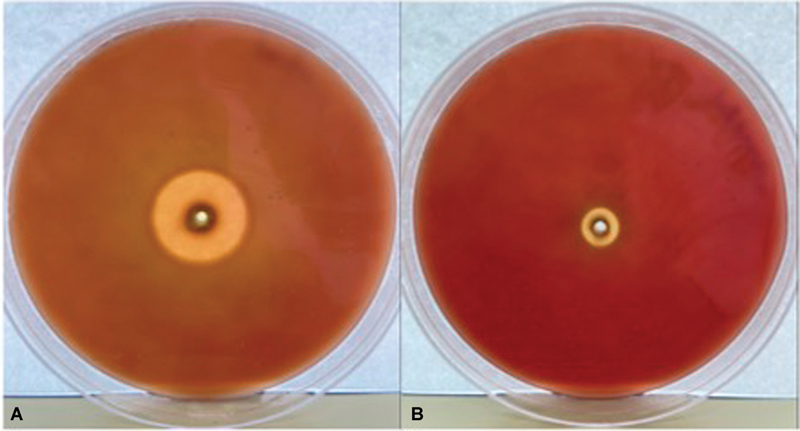
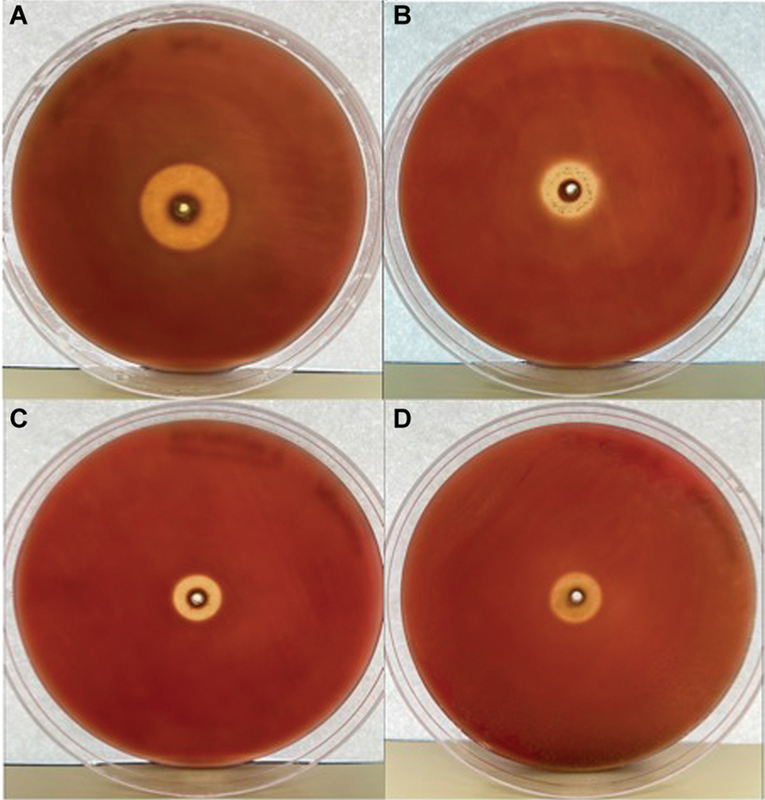
MIC assay: among all four terpenes, citral and geraniol were the most effective overall on all the bacterial strains. Hence, we decided to test them even further in MIC and MBC assays as described earlier in Materials and Methods. MIC refers to the minimum concentration of a drug or antibacterial substance that prevents the growth of 99.9% of cells.[12] We determined MIC values of citral for M. luteus and both oral Streptococcal strains since it was the leading terpene candidate against these bacteria. Likewise, we found geraniol's MIC on E. faecalis since it showed the highest antibacterial effect on this strain. Micrococcus luteus, E. faecalis, and S. mutans showed no growth with citral at a concentration of 5 μL/mL. However, citral was able to kill S. salivarius even at a lower concentration of 2.5 μL/mL ([Figs. 7] [8] [9]).



MBC assay: MBC refers to the minimum concentration of a drug or antibacterial substance that kills 99.9% of cells.[12] No growth of M. luteus was observed with citral at a concentration of 5 μL/mL. However, slight growth was observed at 2.5 μL/mL ([Fig. 7]). Hence, MBC of citral for M. luteus was determined to be 5 μL/mL. Citral was able to kill M. luteus at half molar density to bacterial CFU/mL (approximately 2 × 108 cells per mL). MBC of citral with S. mutans was also determined to be 5 μL/mL with incremental growth from citral concentrations of 2.5 μL/mL onwards ([Fig. 8]). Thus, citral was also able to kill S. mutans at half the molar density to bacterial CFU/mL (approximately 2 × 108 cells per mL). However, citral was even more effective on S. salivarius, preventing growth at a lower concentration of 2.5 μL/mL. Sparse growth was seen from citral concentrations of 1.25 μL/mL onwards ([Fig. 9]). Hence, the MBC of citral for S. salivarius was confirmed as 2.5 μL/mL at one-fourth molar density to bacterial CFU/mL (approximately 2 × 108 cells per mL). Likewise, MBC of geraniol for E. faecalis was confirmed as 5 μL/mL (data not shown) at one-half molar density to bacterial CFU/mL (approximately 2 × 108 cells per mL).
Bacterial time kill assay: overall, since geraniol was found to be very effective on all four bacterial strains, bacterial growth dynamics were observed over 4 hours using a time kill assay with it. Geraniol showed the highest antibacterial activity against S. mutans within minutes of exposure ([Fig. 10C]). It had a bacteriostatic effect on both S. salivarius and E. faecalis for the first 2 hours of exposure and showed significant killing afterward ([Fig. 10A, D]). However, it had a bacteriostatic effect on M. luteus for the first 4 hours of exposure ([Fig. 10B]). Microsoft for Mac - Version 16.89 was used for statistical analysis of the data.

Discussion
Our previous study showed that lemon grass and Citronella Java volatile oils exhibited the highest antibacterial activity on common oral bacteria. We have also previously identified the major terpenes found in both these oils. Citronella Java was mainly composed of the terpenes citronellal, geraniol, and citronellol. Lemon grass was mainly composed of citral.[11] The aim of this preliminary study was to identify which terpenes are responsible for the antibacterial properties of these two volatile oils. We tested these terpenes on a panel of bacteria commonly found in the human oral microbiota, namely, M. luteus, E. faecalis, S. mutans, and S. salivarius.
Overall, while citral was highly effective on M. luteus and most effective on both oral Streptococcal strains, geraniol exhibited the highest killing on E. faecalis at one-half molar density to bacterial CFU/mL (approximately 2 × 108 cells per mL). Citral was able to kill M. luteus, S. mutans, and E. faecalis at half molar density to bacterial CFU/mL (approximately 2 × 108 cells per mL). However, citral was able to kill S. salivarius even at one-fourth molar density to bacterial CFU/mL (approximately 2 × 108 cells per mL) ([Figs. 4] [5] [6] [7] [8] [9] [10]). Our results further demonstrate the overall effectiveness of geraniol and citral against oral bacteria as comparable and even higher than traditional antibiotics like tetracycline. All of these are very encouraging findings. Also of noteworthy mention is the fact that these terpenes are highly effective against tetracycline-resistant S. salivarius strains such as the strain used in our study. Our results suggest that the combination of geraniol and citral in oral mouth rinses would provide the most broad-spectrum antibacterial effect, without the presence of any carcinogenic metabolites, unlike what is observed with the use of ethanol in alcohol-based mouthwashes for the elimination of oral bacteria ([Figs. 1] [2] [3] [4] [5] [6] [7] and [Tables 1] [2] [3] [4]). In addition, with these terpenes there is no known risk of generating multidrug-resistant bacterial strains, unlike what is observed with antibiotic usage.[11]
The production of ACH with the use of alcohol-based mouthwashes is problematic beyond the resulting increase in exposure of the oral mucosa to a carcinogenic compound. While it is proven that oral bacteria contribute significantly to the metabolism of ethanol into ACH, an even greater culprit in ACH production is oral Candida. Previous studies have shown that the presence of Candida yeast in the oral cavity is correlated to higher levels of ACH being subsequently observed in vivo.[3] [4] The risk of ACH production upon ethanol consumption is greater with dysbiosis in the oral cavity, and Candida yeast significantly contributes to causing this, thus leading to greater microbial metabolism of ethanol to ACH.[3] [4] Furthermore, it has observed that both Candida albicans and non-Candida yeast species can also produce ACH at carcinogenic concentrations.[4] Through its fermentation abilities, Candida yeast can produce both ethanol and ACH from carbon sources. Thus, yeast overgrowth poses a significant risk factor to the vicious cycle of poor oral health and ACH production.[4]
The target demographic of alcohol-based mouthwashes, and those who are most likely to overuse them, are heavy consumers of alcohol and tobacco, and those with poor oral hygiene.[1] [2] [3] [4] It is shown that this demographic presents with a higher rate of chronic oral Candida infections due to these lifestyle factors.[4] With consistent use of alcohol-based mouthwashes as an attempt to improve oral health conditions, a vicious cycle is perpetuated. The fermentative properties of oral Candida and the overgrowth of harmful, ACH-producing oral bacteria result in a consistent greater exposure of the oral mucosa to ACH over time, fueled by the very product advertised to improve oral health.[4]
We have shown that geraniol and citral are highly effective antibacterial agents against various oral bacteria, without the production of dangerous metabolites ([Figs. 4] [5] [6] [7] [8] [9] [10] and [Tables 1] [2] [3] [4]). Other studies have tested these terpenes against various strains of yeast and have demonstrated the striking antifungal properties that these compounds also possess.[9] [10] A study of palmarosa oil, of which the main component is geraniol, against Saccharomyces cerevisiae, demonstrated significant anti-yeast activity.[9] It is hypothesized that geraniol may be able to alter the yeast cell membrane and cause excessive leakage of potassium ions from yeast cells, resulting in their death.[9] Citral also appears to show significant antifungal properties, and the epoxide oxidation products of citral are shown to be effective in the treatment of fungal diseases.[9] Citral has also shown to produce a synergistic effect when used in combination with fluconazole against fluconazole-resistant C. albicans yeast strains. It is hypothesized that citral may induce apoptosis in the S phase of the cell cycle of C. albicans.[9] While further studies are needed to achieve a greater understanding of their underlying mechanisms, geraniol and citral show great promise in their use in oral health care, with the ability to solve the issue of chronic Candida infections in the at-risk demographic, thus preventing the production of higher concentrations of ACH with alcohol ingestion and putting an end to the cycle of ACH production that comes with the use of ethanol as an antibacterial agent, without introducing any harmful by-products into the oral mucosa.
The examination of geraniol and citral applied simultaneously or as a mixture, as opposed to in isolation, should also be explored. To achieve broad-spectrum antibacterial coverage, both terpenes are necessary. Their effectiveness together and alone must be tested and compared. The effect of these terpenes on probiotic bacteria, such as Lactobacillus strains, is also of interest. An antibacterial agent that causes minimal or no harm to probiotic oral bacteria while selectively killing harmful bacteria would be ideal for use in oral hygiene, as probiotic bacteria play a vital role in maintaining oral health. It is thought that probiotic bacteria help prevent the growth of harmful pathogens through competitive inhibition, the release of antibacterial substances, such as hydrogen peroxide, and the promotion of mucus production and tight junction expression in epithelial cells.[14] [15] A recent study by Boyapati et al even found that a probiotic mouthwash can be equally effective in improving oral health compared to chlorohexidine (CHX) mouthwash.[15] This highlights the immense importance of probiotic bacteria in the oral microbiome and further suggests that future studies must be done to assess the effects of citral and geraniol on common probiotic bacterial strains. We propose testing geraniol and citral against Lactobacillus strains as a logical next step in assessing these terpenes' potential use in oral health care.
Furthermore, a comparison of our terpenes to CHX would be helpful to gauge their effectiveness compared to the current standard antibacterial mouthwash. While CHX is an effective antiseptic solution, it can cause staining and allergic reactions in some users.[16] These considerations prompted Tulabandula et al to perform a comparison experiment of CHX and another volatile oil, tea tree oil. It was found that a 0.2% CHX solution was equally effective compared to a 5% solution of tea tree oil in killing pathogenic bacteria in the oral cavity.[16] This study further highlights the promise of volatile oil terpenes and their antibacterial and antifungal properties that can be harnessed for use in oral health care. For our terpenes, we propose a future study comparing citral and geraniol at various ratios and concentrations to CHX mouthwash. Not only would this assess their effectiveness in contrast to the standard prescription mouthwash, but it would also explore if concentrations lower than the 5% used by Tulabandula et al, closer to 0.2% of CHX, can be achieved whilst maintaining equal efficacy. Our determination of which specific terpenes are primarily responsible for the antibacterial properties of our volatile oils may allow for lower effective concentrations to be used. By removing other unnecessary components (inactive ingredients) from the volatile oils and using only the primary antibacterial and antifungal compounds (active ingredients), a more efficient solution may be possible.
Conclusion
There are three main conclusions from our study namely:
-
Citral and geraniol were identified as the main terpenes responsible for the antibacterial activity of lemon grass and Citronella Java volatile oils.
-
These terpenes also emerged as the most potent broad spectrum antibacterial agents among all four terpene candidates.
-
Citral was most effective on both oral streptococcal strains namely S. mutans and S. salivarius followed by geraniol, while geraniol exhibited the highest antibacterial activity against E. faecalis. Both terpenes showed a similar pattern of killing as seen with oral streptococci when tested against M. luteus.
The antibacterial and antifungal effects of geraniol and citral present great opportunity for further studies of the mechanisms behind both these properties, and their other potential applications. We propose testing geraniol and citral against Lactobacillus strains as a logical next step in assessing these terpenes' potential use in oral health care.
It is important to note that these terpenes are for topical, local use, not systemic ingestion. These terpenes are also potential candidates for use against skin bacteria and fungi. Their effectiveness against Candida yeast, which is also present on the skin, has been demonstrated; however, their antibacterial effects have not been tested against common skin bacteria.[9] [10] With both antifungal and antibacterial properties, geraniol and citral show potential as treatments for both bacterial and fungal acne in conjunction. A possible limitation from terpenes in these two volatile oils is occurrence of mild allergic reactions in the oral cavity. However, we believe that these minor setbacks can be addressed during repeated experimental trials with varying doses and combinations when our product goes for clinical study.
Conflict of Interest
None declared.
-
References
- 1 Perera M, Al-Hebshi NN, Speicher DJ, Perera I, Johnson NW. Emerging role of bacteria in oral carcinogenesis: a review with special reference to perio-pathogenic bacteria. J Oral Microbiol 2016; 8: 32762
- 2 Ustrell-Borràs M, Traboulsi-Garet B, Gay-Escoda C. Alcohol-based mouthwash as a risk factor of oral cancer: a systematic review. Med Oral Patol Oral Cir Bucal 2020; 25 (01) e1-e12
- 3 Kurkivuori J, Salaspuro V, Kaihovaara P. et al. Acetaldehyde production from ethanol by oral streptococci. Oral Oncol 2007; 43 (02) 181-186
- 4 Nieminen MT, Salaspuro M. Local acetaldehyde—an essential role in alcohol-related upper gastrointestinal tract carcinogenesis. Cancers (Basel) 2018; 10 (01) 11
- 5 Homann N, Jousimies-Somer H, Jokelainen K, Heine R, Salaspuro M. High acetaldehyde levels in saliva after ethanol consumption: methodological aspects and pathogenetic implications. J Carcinog 1997; 18 (09) 1739-1743
- 6 Lachenmeier DW, Gumbel-Mako S, Sohnius EM, Keck-Wilhelm A, Kratz E, Mildau G. Salivary acetaldehyde increase due to alcohol-containing mouthwash use: a risk factor for oral cancer. Int J Cancer 2009; 125 (03) 730-735
- 7 Wilson DF, Matschinsky FM. Ethanol metabolism: the good, the bad, and the ugly. Med Hypotheses 2020; 140: 109638
- 8 Pavlova SI, Jin L, Gasparovich SR, Tao L. Multiple alcohol dehydrogenases but no functional acetaldehyde dehydrogenase causing excessive acetaldehyde production from ethanol by oral streptococci. Microbiology (Reading) 2013; 159 (Pt 7): 1437-1446
- 9 Ganjewala D, Gupta AK. Lemongrass (Cymbopogon flexuosus Steud.) wats essential oil: overview and biological activities. In: Recent Progresses in Medicinal Plants Essential Oils-II. Vol. 37. India: Studium Press Pvt. Ltd; 2013: 233-274
- 10 Nagaki M, Nara T, Sakaiya S, Yamanouchi K, Tsujiguchi T, Chounan Y. Biotransformation of citronellal, geranial, citral and their analogs by fungus and their antimicrobial activity. Trans Mater Res Soc Jpn 2018; 43: 355-358
- 11 Narayanan N, Sabour J, Chiswell B, Weiland M. Evaluation of plant essential oils as natural alternatives for alcohol-based mouthwashes: spotlight-lemongrass and Citronella Java. Eur J Gen Dent 2024; 13: 60-68
- 12 Leboffe MJ, Pierce BE. Microbiology: Lab Theory and Application. Brief edition. Englewood, CO: Morton Publishing Company; 2008
- 13 Ribeaucourt D, Höfler GT, Yemloul M. et al. Tunable production of (R)- or (S)-citronellal from geraniol via a bienzymatic cascade using a copper radical alcohol oxidase and old yellow enzyme. ACS Catal 2022; 12 (02) 1111-1116
- 14 Latif A, Shehzad A, Niazi S. et al. Probiotics: mechanism of action, health benefits and their application in food industries. Front Microbiol 2023; 14: 1216674
- 15 Boyapati R, Peeta J, Dhulipalla R, Kolaparthy L, Adurty C, Cheruvu RNS. Comparative evaluation of the efficacy of probiotic, Aloe vera, povidine-iodine, and chlorhexidine mouthwashes in the treatment of gingival inflammation: a randomized controlled trial. Dent Med Probl 2024; 61 (02) 181-190
- 16 Tulabandula YS, Kumar KK, Rani GR, Chisty MHS, Ravindranath D, Ramanarayana B. Comparative evaluation of subgingivally delivered tea tree oil gel and 0.2% chlorhexidine gel adjunctive to scaling and root planing in chronic periodontitis. JBSMFS 2024; 20 (04) 28-33
Address for correspondence
Publication History
Article published online:
12 August 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Perera M, Al-Hebshi NN, Speicher DJ, Perera I, Johnson NW. Emerging role of bacteria in oral carcinogenesis: a review with special reference to perio-pathogenic bacteria. J Oral Microbiol 2016; 8: 32762
- 2 Ustrell-Borràs M, Traboulsi-Garet B, Gay-Escoda C. Alcohol-based mouthwash as a risk factor of oral cancer: a systematic review. Med Oral Patol Oral Cir Bucal 2020; 25 (01) e1-e12
- 3 Kurkivuori J, Salaspuro V, Kaihovaara P. et al. Acetaldehyde production from ethanol by oral streptococci. Oral Oncol 2007; 43 (02) 181-186
- 4 Nieminen MT, Salaspuro M. Local acetaldehyde—an essential role in alcohol-related upper gastrointestinal tract carcinogenesis. Cancers (Basel) 2018; 10 (01) 11
- 5 Homann N, Jousimies-Somer H, Jokelainen K, Heine R, Salaspuro M. High acetaldehyde levels in saliva after ethanol consumption: methodological aspects and pathogenetic implications. J Carcinog 1997; 18 (09) 1739-1743
- 6 Lachenmeier DW, Gumbel-Mako S, Sohnius EM, Keck-Wilhelm A, Kratz E, Mildau G. Salivary acetaldehyde increase due to alcohol-containing mouthwash use: a risk factor for oral cancer. Int J Cancer 2009; 125 (03) 730-735
- 7 Wilson DF, Matschinsky FM. Ethanol metabolism: the good, the bad, and the ugly. Med Hypotheses 2020; 140: 109638
- 8 Pavlova SI, Jin L, Gasparovich SR, Tao L. Multiple alcohol dehydrogenases but no functional acetaldehyde dehydrogenase causing excessive acetaldehyde production from ethanol by oral streptococci. Microbiology (Reading) 2013; 159 (Pt 7): 1437-1446
- 9 Ganjewala D, Gupta AK. Lemongrass (Cymbopogon flexuosus Steud.) wats essential oil: overview and biological activities. In: Recent Progresses in Medicinal Plants Essential Oils-II. Vol. 37. India: Studium Press Pvt. Ltd; 2013: 233-274
- 10 Nagaki M, Nara T, Sakaiya S, Yamanouchi K, Tsujiguchi T, Chounan Y. Biotransformation of citronellal, geranial, citral and their analogs by fungus and their antimicrobial activity. Trans Mater Res Soc Jpn 2018; 43: 355-358
- 11 Narayanan N, Sabour J, Chiswell B, Weiland M. Evaluation of plant essential oils as natural alternatives for alcohol-based mouthwashes: spotlight-lemongrass and Citronella Java. Eur J Gen Dent 2024; 13: 60-68
- 12 Leboffe MJ, Pierce BE. Microbiology: Lab Theory and Application. Brief edition. Englewood, CO: Morton Publishing Company; 2008
- 13 Ribeaucourt D, Höfler GT, Yemloul M. et al. Tunable production of (R)- or (S)-citronellal from geraniol via a bienzymatic cascade using a copper radical alcohol oxidase and old yellow enzyme. ACS Catal 2022; 12 (02) 1111-1116
- 14 Latif A, Shehzad A, Niazi S. et al. Probiotics: mechanism of action, health benefits and their application in food industries. Front Microbiol 2023; 14: 1216674
- 15 Boyapati R, Peeta J, Dhulipalla R, Kolaparthy L, Adurty C, Cheruvu RNS. Comparative evaluation of the efficacy of probiotic, Aloe vera, povidine-iodine, and chlorhexidine mouthwashes in the treatment of gingival inflammation: a randomized controlled trial. Dent Med Probl 2024; 61 (02) 181-190
- 16 Tulabandula YS, Kumar KK, Rani GR, Chisty MHS, Ravindranath D, Ramanarayana B. Comparative evaluation of subgingivally delivered tea tree oil gel and 0.2% chlorhexidine gel adjunctive to scaling and root planing in chronic periodontitis. JBSMFS 2024; 20 (04) 28-33